
Abstract
Objective:
The purpose of this study was to investigate the influence of CYP2D6 gene polymorphisms on plasma concentrations of risperidone and its metabolite in Thai children and adolescents with autism spectrum disorder (ASD).
Methods:
All 97 autism spectrum disorder patients included in this study had been receiving risperidone at least for 1 month. The CYP2D6 genotypes were determined by real-time polymerase chain reaction (PCR)-based allelic discrimination for CYP2D6*4, *10, and *41 alleles. Plasma concentrations of risperidone and 9-hydroxyrisperidone were measured using liquid chromatography-tandem mass spectrometry (LC-MS/MS).
Results:
Among the 97 patients, the most important nonfunctional alleles (CYP2D6*4 and *5) were detected, whereas the most common allele was CYP2D6*10 (55.9%). CYP2D6 genotyping revealed 90 (92.78%) patients to be extensive metabolizers (EM) and 7 (7.22%) to be intermediate metabolizers (IM). Plasma levels of risperidone were significantly higher in individuals with CYP2D6*5/*10 (p = 0.02), CYP2D6*10/*10 (p = 0.04), and CYP2D6*10/*41 (p = 0.04). Additionally, the plasma concentration of risperidone/9-OH risperidone ratio in patients with a CYP2D6 activity score of 0.5 were significantly higher than those with a CYP2D6 activity score of 2 (p = 0.04). Conversely, no significant influence was found among CYP2D6 polymorphisms, plasma concentrations of 9-hydroxyrisperidone, and the total active moiety.
Conclusions:
This is the first study to investigate the effects of CYP2D6 genetic polymorphisms on the plasma concentrations of risperidone in Thai children with ASD. The findings indicate that CYP2D6 polymorphisms affect the plasma concentrations of risperidone and the risperidone/9-hydroxyrisperidone ratio. Genetic screening for CYP2D6 polymorphisms could help to predict unexpected adverse events caused by the higher plasma concentration of risperidone.
Introduction
R
The CYP2D6 gene is located at chromosome 22q13.1 and consists of nine exons (Zanger et al. 2004; Gaedigk 2013). The role of CYP2D6 polymorphisms is extensively studied, because of the differences in pharmacokinetics, clinical outcome, and adverse events (Ingelman-Sundberg 2005; Zhou 2009a,b; Ingelman-Sundberg and Sim 2010). The CYP2D6 gene, being the most highly polymorphic among the CYPs, exhibits the largest phenotypic variability. Recently, >100 allelic variants and subvariants of the CYP2D6 gene have been reported, and are associated with the absence, decrease, increase, or normal enzyme activity according to the Human Cytochrome P450 Allele Nomenclature Committee (
The frequency of CYP2D6 variations varies among different ethnic populations (Hicks et al. 2013; LLerena et al. 2014). Generally, the CYP2D6*1 (wild-type) allele is the most commonly occurring allele in different populations (Hicks et al. 2013). CYP2D6*1 is reported with a frequency of 38% in East Asian populations. Among the CYP2D6 variant alleles, CYP2D6*10 is the most common allele found in Asian populations (Gan et al. 2002). In Thai ASD patients, CYP2D6*1, *2, and *10 alleles had a frequency of 22.78%, 11.39%, and 54.43%, respectively. Moreover, we reported allelic frequencies of 0.02%, 5.15%, and 2.58% for the polymorphic alleles *4, *5, and *41, respectively, in Thai population (Suwannarat et al. 2013).
The functional phenotypes of the CYP2D6 genotype include poor metabolizers (PM), intermediate metabolizers (IM), extensive metabolizers (EM), and ultrarapid metabolizers (UM), predicted by the biallelic expression of alleles (Gaedigk 2013; Hicks et al. 2014). The two copies of the nonfunctional alleles of CYP2D6 are considered to be PM, whereas the IM is caused by a combination of one nonfunctional and one reduced function allele. An individual carrying two functional alleles, two reduced function alleles, one functional and one nonfunctional allele, or one functional and one reduced function allele are considered to be EM. Lastly, individuals carrying more than two functional gene copies are considered to be the UM phenotype (Hicks et al. 2013).
The effect of CYP2D6 polymorphisms on steady-state plasma level of RIS, 9-OH-RIS, active moiety concentration, and RIS/9-OH-RIS has been reported in previous studies (Scordo et al. 1999; Yasui-Furukori et al. 2004; Gunes et al. 2008; Jovanovic et al. 2010; Locatelli et al. 2010). However, one study of the association between CYP2D6 genotypes and the plasma RIS levels in ASD children has been reported (Youngster et al. 2014). To our knowledge, no study has examined CYP2D6 polymorphisms affecting RIS metabolism in the Southeast Asian ASD population. To further establish the relationship between CYP2D6 status and plasma RIS levels, we investigated the influence of the CYP2D6 genotypes on the steady-state plasma concentrations of RIS, 9-OH-RIS, RIS/9-OH-RIS ratio, and total active moiety plasma level in Thai ASD patients.
Methods
Subjects
In this study, the outpatients who were regularly followed up at Yuwaprasart Waithayopathum Child Psychiatric Hospital, Samutprakan, Thailand were enrolled. The subjects comprised 97 (88 males and 9 females) Thai ASD patients who fulfilled Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria (American Psychiatric Association 1994). All the patients had received RIS for >4 weeks before the study. The RIS doses were administered according to weight: 1) 0.25–0.5 mg/day for patients with body weight <20 kg and 2) 0.5–1 mg/day for patients with body weight ≥20 kg (Janssen Pharmaceuticals 2014). The patients' compliance was confirmed by the nursing staff.
Patients who were unable to take medicine regularly or for whom medication needed to be changed were excluded. Moreover, patients receiving CYP2D6 substrates affecting RIS metabolism were not included, because these drugs are known to modulate the RIS metabolism and its plasma levels (de Leon et al. 2008). This study was approved by Ramathibodi Ethics Committee, Bangkok, Thailand. After the study was completely described, the parents of all children involved in the study gave informed written consent to participate and undergo genetic analysis.
Sample preparation and DNA extraction
After an overnight fast, blood samples were obtained before the morning dose in ethylenediaminetetraacetic acid (EDTA) tubes for genotype analysis and measurement of steady-state plasma concentrations of RIS and 9-OH-RIS. Genomic DNA was isolated with MagNA Pure compact system (Roche Diagnostics GmbH, Germany). Genomic DNA was quantified by a NanoDrop™ 1000 spectrophotometer at 260 nm (Thermo Fisher Scientific, Wilmington, DE).
CYP2D6 genotyping and predicted phenotypes
CYP2D6 genotypes were identified in all the patients by TaqMan® allelic discrimination methods real-time PCR assays (Applied Biosystems, Foster City, CA) that discriminate among CYP2D6 *4, *10, and *41, which are frequently found in the Thai population (Suwannarat et al. 2013). CYP2D6 genotyping was detected by TaqMan single nucleotide polymorphism (SNP) genotyping assays, which were performed with primers of CYP2D6*4 (1846G>A, rs3892097, assay ID: C_27102431_00), CYP2D6*10 (100C>T, rs1065852, assay ID: C_11484460_40), and CYP2D6*41 (2988G>A, rs28371725, assay ID: C_34816116_20). The CYP2D6 gene copy number variation was genotyped using TaqMan Copy Number Assays (assay ID: Hs04083572_cn) in all samples. A copy number variation (CNV) result of 0 or 1, as compared with the normal 2, indicates CYP2D6 gene deletion, which is inferred as CYP2D6*5 according to the Human Cytochrome P450 Allele Nomenclature Committee (
The CYP2D6-predicted phenotypes were determined following the activity score system (Gaedigk et al. 2008). Patients with the activity score 0 were classified as PM. Patients with the activity score 0.5 were classified as IM, those with a value of 1.0–2.0 were classified as EM, and those with a value >2 were classified as UM (Hicks et al. 2013).
Assay of plasma RIS and 9-OH-RIS concentrations
Steady-state of RIS and its main active metabolite 9-OH-RIS trough plasma concentrations were measured using an early morning sample by a validated liquid chromatography tandem-mass spectrometry (LC-MS/MS) method with slightly modifications of previously published methods (Zhang et al. 2010). The liquid chromatograph was an Agilent 1260 HPLC system consisting of a binary pump, a system controller, and an autoinjector. The chromatographic system was connected to an API 3200 (AB Sciex) with an internal diverter (Valco valve). Chromatographic separation was performed on a Waters Atlantis dC18 column (4.6 cm × 50 mm; 1.8 μm particle size), which was protected by an Atlantis dC18 4.6 × 12.5 mm guard column.
Mobile phase A consisted of ammonium acetate (10 mmol/L) containing 0.1% formic acid. Mobile phase B consisted of 100% acetonitrile. Separation of RIS and 9-OH-RIS derivatives was performed at a flow rate of 0.40 mL/min. Ionization was achieved in the positive-ion mode with 5500V ionization. The heater probe was set up at 500°C. Sample analysis was performed in the multiple-reaction monitoring mode with the transitions m/z 411–191 for RIS, m/z 428–207 for 9-OH-RIS derivative, and m/z 328–270 for clozapine. Collision energy was set up at 38 V for RIS and 40 V for 9-OH-RIS. One sample was injected every 6 minutes. Integration of peak areas and determination of the concentrations was performed with Analyst 1.5.2 software (Applied Biosystems, CA). Quadratic regression with 1/× weighted concentrations was used.
The mean inter- and intra-assay accuracy for both RIS and 9-OH-RIS was set within ±15.0% relative error (RE) of nominal, and precision ≤15.0% relative standard deviation (RSD) (Whitmire et al. 2011).
Statistical analysis
Data were expressed as median (interquartile range [IQR]). Descriptive statistics were used to describe the clinical characteristics of the subjects. Power and Sample Size, version 1.01 (Dupont and Plummer), was used to calculate sample size. After testing for normality, a Mann–Whitney U test was used to compare between two groups, and a Kruskal–Wallis test was used to make comparisons among three groups. P values <0.05 were considered statistically significant. Statistical analyses were performed by using SPSS version 18.0 (SPSS Inc., Chicago, IL).
Results
Study population
The demographic and clinical characteristics of the patients, including age, sex, concurrent medication use, and RIS dosage are summarized in Table 1. Among 97 patients, the sample was predominantly male (n = 88; 90.72%), and the median age was 10 years (IQR: 7.00–12.15). In the total sample, the median RIS dose was 0.6 mg/day. The median concentration of RIS was 1.01 ng/mL (IQR: 0.02–2.98), and that of 9-OH-RIS was 6.84 ng/mL (IQR: 3.76–12.90), whereas active moiety concentration was 8.17 ng/mL (IQR: 5.67–14.19). The concentration ratio of RIS/9-OH-RIS was 0.15 (IQR: 0.00–0.34). Forty-nine patients (50.52%) also received co-medications in this study. The medications that were concomitantly prescribed to patients were methylphenidate (n = 25; 25.77%), valproic acid (n = 21; 21.65%), carbamazepine (n = 2; 2.06%), benzhexol (n = 2; 2.06%), diazepam (n = 2; 2.06%), and topiramate (n = 1; 1.03%).
IQR, interquartile range.
CYP2D6 genotype analysis
The allele frequencies of CYP2D6*1, CYP2D6*4, CYP2D6*5, CYP2D6*10, and CYP2D6*41 are shown in Table 2. Of the possible nonfunctional CYP2D6 alleles, only *4 and *5 were detected. The allele frequency for CYP2D6*4 was 1.55%, whereas CYP2D6*5 had a frequency of 5.67%. Two polymorphic CYP2D6 alleles associated with decreased CYP2D6 enzyme activity, *10 and *41, constituted 54.12% and 4.12%, respectively (Table 2).
CYP2D6 major genetic variant according to
SNP, single nucleotide polymorphism.
In addition, ninety patients (92.78%) with CYP2D6*1/*1 (n = 9; 9.27%), CYP2D6*1/*10 (n = 39; 40.21), CYP2D6*1/*41 (n = 3; 3.09%), CYP2D6*10/*10 (n = 27; 27.83%), CYP2D6*10/*41 (n = 5; 5.15%), and CYP2D6*1/*5 (n = 7; 7.22%) were classified as EM. Seven patients (7.22%) with CYP2D6*4/*10 (n = 3; 3.09%) and CYP2D6*5/*10 (n = 4; 4.12%) were classified as IM. The CYP2D6 genotypes and predicated phenotypes in the 97 patients under study are presented in Table 3.
Statistical significance was calculated by Mann–Whitney U test.
CYP2D6 activity score according to Gaedigk et al. (2008).
CYP2D6 predicted phenotype according to Hicks et al. (2013).
*1/*1: reference.
p value <0.05.
IQR, interquartile range; EM, extensive metabolizer; IM, intermediate metabolizer.
Relationship between CYP2D6 polymorphisms and the plasma concentrations of RIS and its metabolites
The plasma concentration of RIS in subjects with CYP2D6*5/*10 (4.34 ng/mL, p = 0.02), CYP2D6*10/*10 (1.85 ng/mL, p = 0.04), and CYP2D6*10/*41 (2.24 ng/mL, p = 0.04) were significantly higher than those with the homozygous wild type genotype CYP2D6*1/*1 (Fig. 1). CYP2D6*4/*10 (0.65 ng/mL, p = 0.60) did not show a significantly higher level of RIS plasma concentration as compared with the CYP2D6*1/*1 genotypes. No significant difference was found for the median of plasma concentration of 9-OH-RIS, total active moiety, and RIS/9-OH-RIS ratio among the subjects with CYP2D6 genotypes (Table 3).
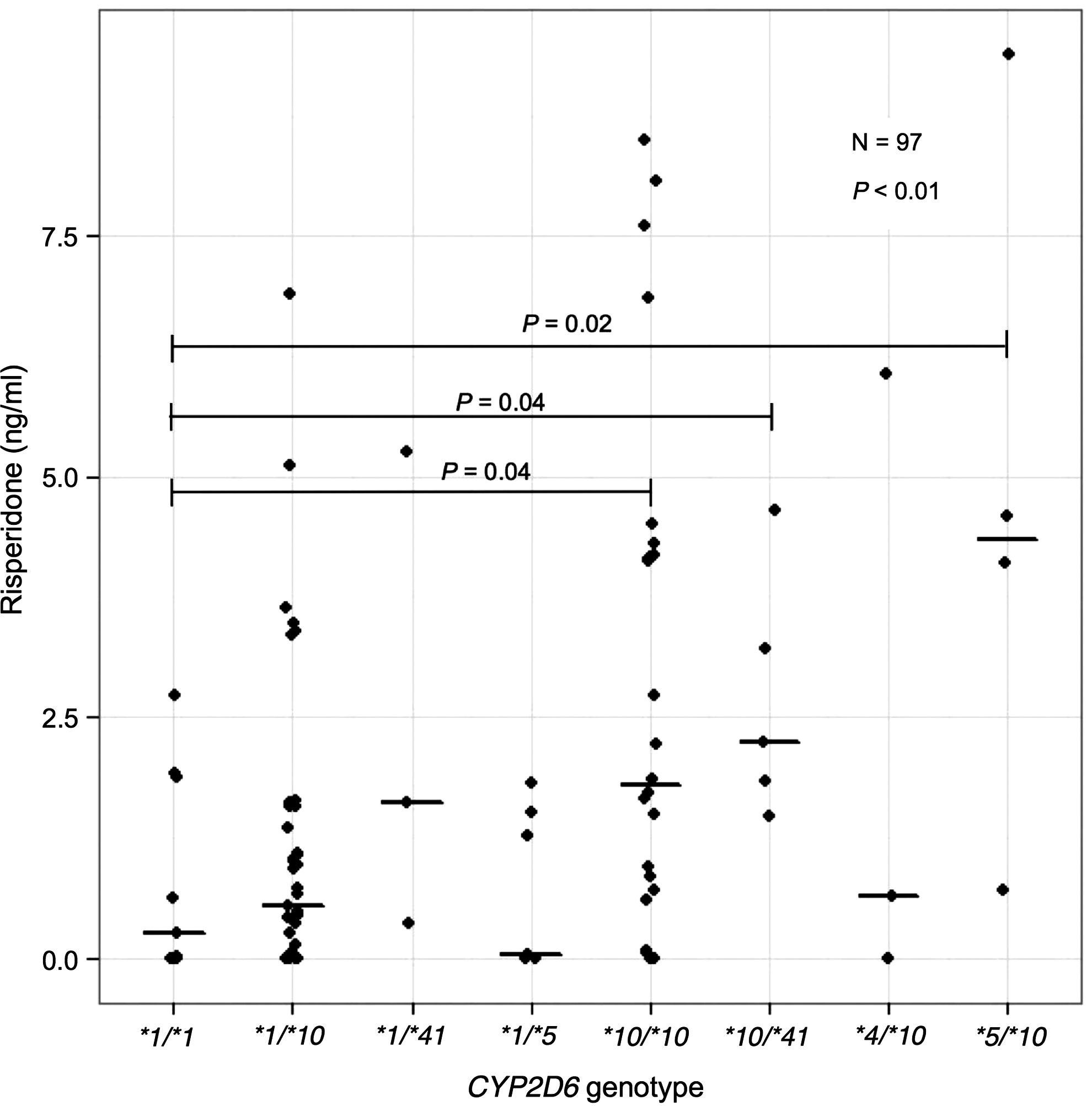
Relationship between CYP2D6 genotype and risperidone level.
Relationship between CYP2D6 activity score and plasma concentrations of RIS and its metabolites
The patients were combined into four groups based on the CYP2D6 activity score (Table 4). Most of patients (43%) had a CYP2D6 activity score of 1.5, the second most (40%) had a CYP2D6 activity score of 1, whereas a score of 2 and 0.5 was present for 10% and 7% of the patients, respectively (Table 4). The RIS/9-OH RIS in patients with a CYP2D6 activity score of 0.5 were significantly higher than those with a CYP2D6 activity score of 2 (p = 0.04). There were no statistically significant differences in RIS concentration between the patients with a CYP2D6 activity score of 0.5 and those with a CYP2D6 activity score of 2; however, there was a tendency for significant differences in RIS concentration among them (p = 0.055) (Fig. 2).
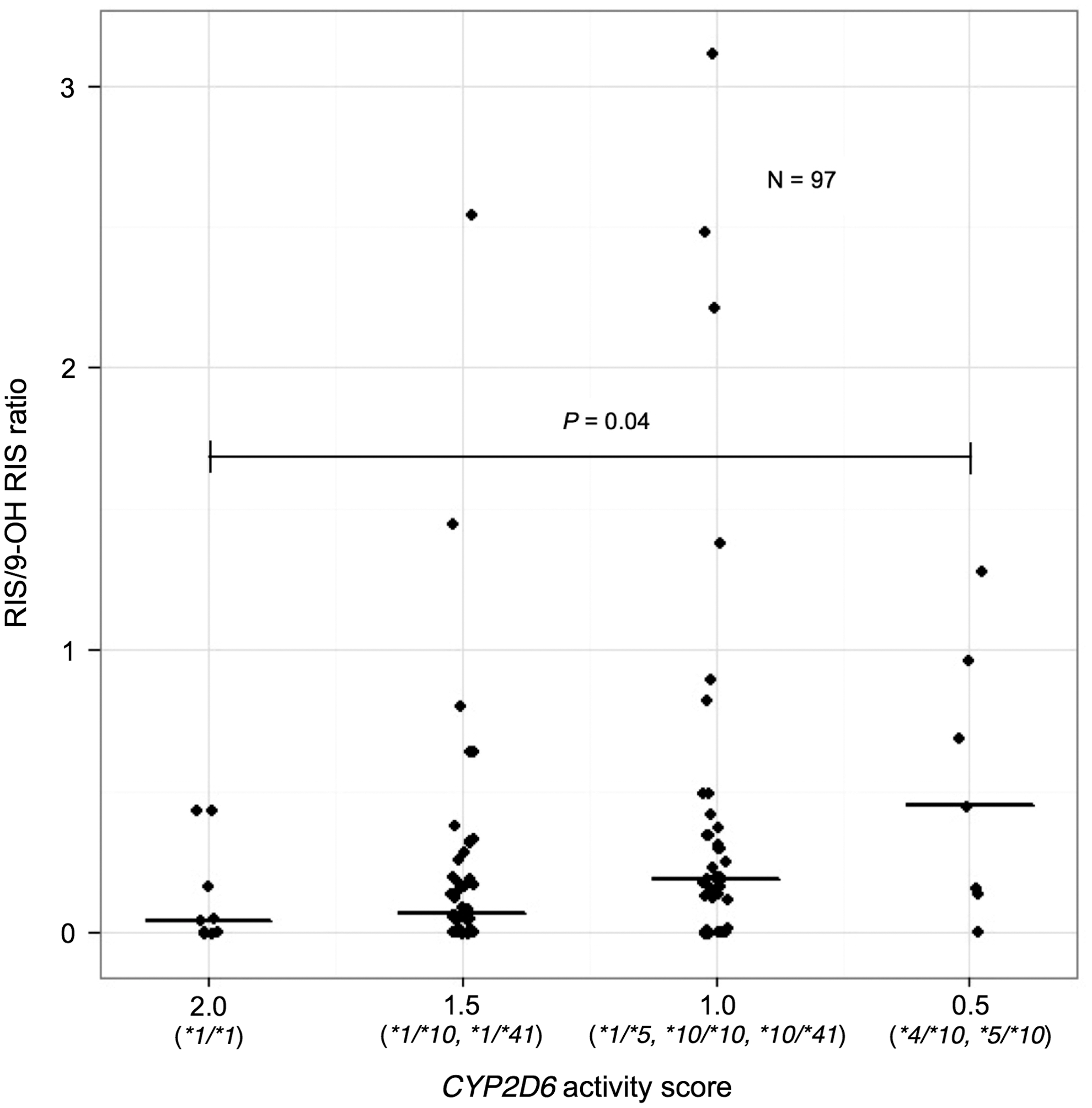
Relationship between CYP2D6 activity score and risperidone/9-hydroxyrisperidone ratio.
Statistical significance was calculated by Mann–Whitney U test.
CYP2D6 activity score 2: reference.
CYP2D6 activity score according to Gaedigk et al. (2008).
p value <0.05.
IQR, interquartile range.
Discussion
Risperidone is the approved drug in the treatment of behavioral symptoms in autism, and is primarily metabolized into the active metabolite, 9-OH-RIS, via 9-hydroxylation by the highly polymorphic CYP2D6 enzyme (Canitano and Scandurra 2011; Yoo et al. 2011). Several studies have reported the influence of CYP2D6 genotype on the metabolism of RIS. CYP2D6 genotypes contributed to the variability in the steady-state plasma concentration of RIS, and metabolic ratio (RIS/9-OH-RIS) (Yasui-Furukori et al. 2003; Kang et al. 2009; Yoo et al. 2011). We investigated the effects of CYP2D6 polymorphisms on RIS, its metabolite 9-OH-RIS, active moiety concentration, and metabolic ratio (RIS/9-OH-RIS) in Thai ASD patients. Our results suggest that CYP2D6 genetic polymorphisms affect plasma RIS levels.
In the present study, plasma concentrations of RIS and metabolic ratio of RIS/9-OH-RIS were significantly associated with the CYP2D6*10 allele, but plasma concentration of 9-OH-RIS and active moiety were not found to be significantly correlated. Our result was also consistent with previous studies in adults, which reported the influence of CYP2D6 polymorphisms on plasma concentration of RIS, but not for 9-OH-RIS and active moiety (Yasui-Furukori et al. 2003; Xiang et al. 2010; Suzuki et al. 2012). This suggests the accumulation of RIS, which leads us to postulate the lower metabolic activity of CYP2D6 enzyme among the carriers of CYP2D6 polymorphisms. Our study confirms the findings of a recent study in pediatric patients with ASD treated with RIS: PMs had significantly higher RIS plasma levels (p = 0.03) and RIS/9-OH-RIS ratio (p = 0.02) (Youngster et al. 2014). The enzyme activity is measured by a metabolic ratio, and it might be a useful biomarker to predict individuals with poor or ultrarapid metabolism, which might facilitate personalized therapy (Mannheimer et al. 2014). The significant influence of the CYP2D6 polymorphisms on metabolic ratio might also be an important indicator for a change in dose of RIS, and reduce adverse drug reactions (ADR) related to higher plasma concentration of RIS. Moreover, plasma levels of RIS were significantly higher in individuals with CYP2D6*5/*10 as compared with the homozygous wild type genotype. However, CYP2D6*4/*10 did not show a significantly higher level of RIS plasma concentration than did the homozygous wild type genotype, which possibly indicates the influence of CYP3A and ABCB1, which intervene in RIS pharmacokinetics (Gunes et al. 2008; Kang et al. 2009).
Even though the level of the active moiety is not significantly associated with the CYP2D6 polymorphism; active moiety can influence therapeutic efficacy and side effects. There are differences between RIS and 9-OH-RIS in binding affinity for the receptors and pharmacological activity, which suggests the importance of individual components in predicting efficacy and side effects (Cartwright et al. 2013). Previous studies showed ADR among CYP2D6 PMs in RIS-treated patients (de Leon et al. 2005; Youngster et al. 2014). The CYP2D6 poor metabolizer phenotype was associated with threefold increased moderate to marked adverse effects (de Leon et al. 2005). Higher plasma level of RIS also predicted the incidence of extrapyramidal side effects (Riedel et al. 2005). To date, there are dosing recommendations for tricyclic antidepressants based on genotype-predicted CYP2D6 phenotype. One should consider a 25% reduction of the recommended starting dose for the patient with CYP2D6 IMs and consider an alternative drug not metabolized by CYP2D6 for the patient with CYP2D6 PMs or UMs. For the patient with CYP2D6 EMs, one should considered initiating therapy with the recommended starting dose (Hicks et al. 2013). However, there are inadequate data to allow calculation of dose adjustment for risperidone. According to Swen et al., the selection of an alternative drug (e.g., quetiapine, olanzapine, clozapine) or being especially alert to ADR and adjusting the dose to clinical response for RIS may be considered (Swen et al. 2011).
ASD is more common in males than in females, with a male to female ratio of 4.3:1 (Fombonne 2009). However, we observed a male to female ratio of 10:1 in this study. Our study also indicates that gender has a major impact on RIS plasma levels. The previous study found that in the group of adolescents, females exhibited significantly higher active moiety concentration than males, even though they were treated with a similar dose of RIS (Aichhorn et al. 2007). Further studies enrolling a larger number of patients are necessary to evaluate gender differences in children and adolescents in addition to obtaining significant results despite highly varying interindividual enzyme activities.
Apart from the predominant CYP2D6 enzyme, there is evidence of biotransformation of RIS by CYP3A4 and CYP3A5 enzymes, which modulate pharmacokinetic characteristics, albeit in smaller quantity (Yasui-Furukori et al. 2001; Kang et al. 2009). A number of genetic polymorphisms of CYP3A genes have been identified. The important polymorphic alleles include CYP3A5*3 (A6986G), CYP3A4*1G, and CYP3A4*15, which have been studied previously in Asian populations (Kang et al. 2009; Du et al. 2010). In addition to the CYP enzymes, the drug transporter protein P-glycoprotein (P-gp) (multi-drug resistant gene [MDR1], ABCB1) can alter the pharmacokinetic profile of RIS with changes in steady-state plasma concentration of RIS, 9-OH-RIS, and active moiety (Gunes et al. 2008; Jovanovic et al. 2010; Suzuki et al. 2013). Therefore, a specific interpretation of the CYP3A and MDR1 genotypes needs to be evaluated in further studies to optimize blood levels in patients treated with RIS, and minimize the influence on analysis.
To our knowledge, this is the first study to investigate the effects of CYP2D6 genetic polymorphisms on the plasma concentrations of RIS in Thai children with ASD. The small number of patients is one of the limitations in this study. To confirm the relationship, larger samples and comprehensively designed trials in Thai autistic children are required. The number of subjects in each genotype groups and the number of CYP2D6*4 and *41 alleles is small in this population.
Conclusions
The present study suggests that CYP2D6 polymorphisms affect the plasma concentrations of RIS and the metabolic ratio RIS/9-OH-RIS. Our research findings may provide useful information to determine clinical outcomes to further predict an individual's phenotype rather reliably, which could help clinicians provide better treatment for every Thai child with ASD, reduce adverse reactions or therapeutic failure, and improve therapeutic efficiency. CYP2D6 testing before RIS administration may be considered in guiding dosage adjustments in patients who would be treated with RIS, which might help avoid adverse effects. Otherwise the alternative therapy, which is not affected by CYP2D6 variants (olanzapine, quetiapine, or ziprasidone) might be considered for patients with reduced CYP2D6 metabolic capacity. Further studies should evaluate the combined influence of the CYP3A, ABCB1, and CYP2D6 genotypes, to optimize blood levels in patients treated with RIS. The cost effectiveness and clinical utility of the genetic testing must also be analyzed, for personalized treatment of the patients.
Footnotes
Acknowledgments
The authors thank all staff in Yuwaprasart Waithayopathum Child and Adolescent Psychiatric Hospital and all the children and adolescents with ASD who participated in the study.
Disclosures
No competing financial interests exist.