
Abstract
Objective:
This study investigated the gender differences in behavioral symptoms, as rated by various informants, and in neuropsychological performance, among patients with attention-deficit/hyperactivity disorder (ADHD) treated with methylphenidate during 24 months in a clinical setting.
Methods:
Study participants comprised 128 boys (mean age: 13.2±2.4 years) and 26 girls (mean age: 12.8±1.0 years) with ADHD. All patients were prescribed short-acting oral methylphenidate, taken two or three times daily; each dose ranged between 0.3 and 1.0 mg/kg. At the baseline and 6, 12, 18, and 24 months later, behavioral symptoms were evaluated using the parent and teacher forms of the Swanson, Nolan, and Pelham Version IV (SNAP-IV) scale for ADHD and the ADHD Rating Scale (completed by a child psychiatrist). In addition, neuropsychological function was assessed using the Test of Variables of Attention (TOVA) at each interval.
Results:
Although both the boys and girls exhibited a significant decrease in the ADHD symptoms observed by parents and clinicians, the girls improved more than the boys did. Based on the teacher reports, neither the boys nor the girls exhibited significant decreases in ADHD symptoms. The symptoms rated by teachers were more severe in the boys than in the girls throughout the first 12 months; however, the gender difference lessened after 12 months. Based on the TOVA assessment, a composite score (containing response time, response time variability, and ADHD score obtained using the TOVA) did not indicate differences between genders. However, another composite score (containing omission errors, commission errors, and response sensitivity) suggested significant improvement only in the boys.
Conclusions:
The results suggested that according to a longitudinal follow-up, behavioral and neuropsychological changes among patients with ADHD might differ between genders. Gathering multidimensional information from patients with ADHD is essential in determining how gender modifies the functional outcome of ADHD.
Introduction
A
Although numerous studies had demonstrated that females with ADHD differ from males in important ways, little research exists that evaluates gender differences in treatment response during long-term follow-up (Nussbaum 2012). A 3-year follow-up of the Multimodal Treatment Study of Children with ADHD (MTA) study suggested that gender does not influence the long-term treatment responses among children (Jensen et al. 2007). Monuteaux et al. (2010) reported that boys and girls exhibited a similar course of ADHD symptomatology during a 4–10-year follow-up. Most of the aforementioned studies assessed the treatment response or clinical course of ADHD according to parental observation or clinician rating. Nevertheless, the behavioral symptoms of ADHD patients might vary according to different settings (McConaughy et al. 2010) or to different observers' perceptions (Breuer et al. 2011). For example, teachers reported more severe hyperactivity and impulsivity symptoms in boys than in girls; however, the difference between genders was less marked according to parental reports (Ullebo et al. 2012). A comprehensive literature review determined that longitudinal study comparing the gender difference in ADHD symptoms noted by multiple informants is still scarce.
Psychostimulant drugs, which can effectively reduce ADHD symptoms and enhance cognitive functioning, are typically the first-line treatment for ADHD (Huang and Tsai 2011; Coghill et al. 2014). Short-term administration of methylphenidate (MPH) is comparably efficacious for behavioral symptoms in both boys and girls with ADHD (Cornforth et al. 2010). Regarding the gender difference in MPH effect on neuropsychological functions, Zhang et al. (2011) reported that MPH can enhance intellectual performance within a 6 month period, and did not observe a significant difference between boys and girls. However, another study indicated that the impulse control and perceptual sensitivity of male patients improved more significantly than did that of female patients during clinical MPH treatment for 12 months (Huang et al. 2012). In sum, little is known about whether neuropsychological functioning differs between boys and girls who are treated with MPH for ADHD after 12 months. The long-term response to MPH might vary between genders because of genetic variability (Dafny and Yang 2006). Determining a gender differences in the longitudinal course of ADHD would enable clinicians to form accurate prognoses and provide adequate intervention for patients. Therefore, this study examined potential gender differences in behavioral symptoms and neuropsychological functioning among youth treated with MPH for ADHD.
Methods
Study participants
The research protocol was approved by the Institutional Review Board at Chang Gung Hospital in Taiwan. Eligible patients with ADHD treated in the Outpatient Department of Child Psychiatry at Chang Gung Children's Hospital in Taiwan were recruited to participate in this study if they 1) were between 6 and 18 years of age, and 2) were clinically diagnosed with ADHD by two senior child psychiatrists based on the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) (American Psychiatric Association 2000), after structured interviews during which the Chinese version of the Schedule for Affective Disorder and Schizophrenia for School-Age Children, Epidemiologic Version (K-SADS-E) (Kaufman et al. 1997). The Chinese version of K-SADS-E was developed by the Child Psychiatry Research Group in Taiwan (Gau and Soong 1999). They were also required to have been newly diagnosed with ADHD, or to have an existing diagnosis, but not have used ADHD medication for a minimum of 6 months.
Patients were excluded if they 1) had a history of comorbid pervasive developmental disorders, mental retardation, bipolar disorder, psychosis, epilepsy, or brain injury; or 2) required additional behavioral or family therapy in addition to the standard therapy at the Outpatient Department of Child Psychiatry.
Measurements
The Swanson, Nolan, and Pelham Version IV Scale (SNAP-IV), a 26 item questionnaire that is used to evaluate ADHD symptoms and severity, was completed by parents or teachers (Bussing et al. 2008). The 26 items include 18 items related to ADHD symptoms (9 for inattention and 9 for hyperactivity and impulsivity), and 8 pertaining to the oppositional defiant disorder symptoms defined in the DSM-IV-TR. Each item is scored on a three point Likert scale. The Chinese version of the SNAP-IV parent form (Gau et al. 2008b) and the SNAP-IV teacher form (Gau et al. 2009) have been reported to have satisfactory levels of reliability and concurrent validity. In this study, only the subscales of inattention and hyperactivity and impulsivity were analyzed.
The ADHD Rating Scale (ADHD-RS), a validated instrument used by clinicians to assign ratings based on information obtained from the parent(s) and child (Reid et al. 1998), comprises 18 items derived from the criteria outlined in the DSM-IV to diagnose ADHD. Each of the items is scored on a four point Likert scale. A total score from the ADHD-RS can be obtained, and the scale can be divided into an inattentiveness subscale and a hyperactivity and impulsivity subscale. Higher scores indicate a greater severity of ADHD. The scale is reported to have adequate interrater reliability (Zhang et al. 2005).
The Test of Variables of Attention (TOVA) was applied to assess the neurocognitive function of the ADHD patients. The TOVA is a computerized, continual performance test comprising a target stimulus and a nontarget stimulus (Greenberg 1996). The TOVA stimuli are colored squares containing a small black square that is adjacent to either the top or the bottom edge of the colored square. The stimuli appear individually and randomly at a predetermined ratio. The tested participant must press a button immediately on seeing a target, but refrain from pressing the button when a nontarget appears. The test continues for 22.6 minutes and is preceded by a 2.5 minute practice session. The TOVA is reported to have satisfactory levels of reliability and concurrent validity among Taiwanese children with ADHD (Wu et al. 2007). The indices measured in the TOVA include the following: Omission errors, commission errors, response time (in microseconds), response time variability, response sensitivity (d’) and ADHD score. The ADHD score is calculated by comparing individual scores on the TOVA with the scores from an ADHD sample. The score indicates the similarity between the patient performance and the ADHD profile.
Study procedure
The study was a 24 month, nonrandomized, prospective study. Each patient received the same assessment five times. At Month 0, all patients were drug naïve or had not taken ADHD medication for a minimum of 6 months. Experienced child psychologists administered the TOVA to ADHD patients individually in a room that was designed to reduce variability in testing conditions. The SNAP-IV parent form, SNAP-IV teacher form, and the ADHD-RS were completed by the parents, one teacher, and a child psychiatrist, respectively. These informants rated patient symptoms based on the patient behavior over the previous 7 days.
The ADHD patients were prescribed oral immediate release methylphenidate (IR-MPH), taken two or three times daily in doses ranging between 0.3 and 1.0 mg/kg, based on the severity of clinical symptoms, age, height, and body weight. Concomitant medications were prohibited. Patients were typically reassessed by a child psychiatrist at the outpatient department once per month, and modification of the MPH dose was allowed. The second, third, fourth, and fifth assessments were performed 6, 12, 18, and 24 months after initial treatment with MPH, respectively. To avoid the bias caused by the time of medication administration, patients did not take MPH on the day of the TOVA assessment. The assessment procedures administered at Month 0 were repeated.
Statistical analysis
Data were analyzed using the statistical software package SPSS, Version 16.0 (SPSS Inc., Chicago, IL). Variables were presented as either the mean (standard deviation) or frequency. The TOVA results were reported as standard deviations (Z score), which indicated the extent of deviation from the norm. The χ2 test or t test was used to compare the variables at baseline between boys and girls.
Numerous parameters of measures for ADHD were used in this study, creating a risk of type I errors. To reduce this risk, the behavioral symptoms, which were measured by parents, teachers, and clinicians, and the TOVA results were condensed using principal component analysis (PCA) with a set of weights for a composite ADHD score for each factor. The factors yielding eigenvalues >1.00 were retained for varimax rotation, and the extent of the composite ADHD score for each identified factor was investigated.
Data missing during the follow-up were accounted for by using the last observation carried forward method. The longitudinal data were analyzed using a linear mixed model, and the maximum likelihood estimation method and autoregression covariance matrix were employed as the primary analytic strategy. The dependent variables in linear mixed models were set as the composite ADHD scores that were retained for PCA. This study investigated the extent of the potential gender differences in changes of behavioral symptoms and neuropsychological performance within a 24 month MPH treatment; age, ADHD subtypes, and mean doses of MPH over the course of study were controlled for by including them as covariates in the analyses. The hypothesis that a differential change would occur in dependent measures over 24 months was supported by significant interactions of gender×time. The post-hoc tests for gender differences in composite ADHD scores at each time point were employed for repeated-measure analysis of variance (ANOVA), followed by a least significant difference (LSD) test. Two-tailed p values of <0.05 were considered statistically significant.
Results
A total of 154 patients with ADHD (mean age: 13.1±2.3 years) were recruited in this study. Table 1 lists the characteristics of participants at baseline. Of the patients, 128 (83.1%) were boys (mean age: 13.2±2.4 years) and 26 (16.9%) were girls (mean age: 12.8±1.0 years). Distribution of the ADHD subtypes differed between genders (χ 2=6.91, p=0.032); a higher proportion of boys were classified into the hyperactive–impulsive or combined subtype (n=69, 53.9%), whereas girls were more likely to be classified into the inattentive subtype (n=19, 73.1%). The inattention scores and hyperactivity/impulsivity scores rated by teachers were significantly higher among boys than among girls. No significant differences in other indices were noted at baseline. Among the patients, 87 (68.0%) boys and 19 (73.1%) girls completed the study (χ 2=0.26, p=0.608). The mean dose of MPH prescribed to the patients at Months 6, 12, 18, and 24 was 18.1±9.3 mg, 21.1±10.8 mg, 23.6±11.6 mg, and 26.3±12.1 mg for boys; and 17.2±8.3 mg, 18.9±9.0 mg, 20.9±8.9 mg, and 21.9±10.7 mg for girls, respectively. No significant gender differences in the mean doses of MPH over the course of study were noted (t=1.54, p=0.124).
Test of Variables of Attention (TOVA) results are reported as standard deviations from the norm.
Data are expressed as mean±SD or n (%); aStatistical values are expressed as t values or χ 2.
p<0.05.
ADHD, attention-deficit/hyperactivity disorder; SNAP-IV, Swanson, Nolan, and Pelham Version IV; ADHD-RS, ADHD Rating Scale; I, inattention scores; H, hyperactivity/impulsivity scores.
Table 2 shows the weights for the measures of each of the four factors (composite ADHD scores) that yielded eigenvalues >1.00 and retained for PCA. The four factors, which had eigenvalues of 3.70, 2.97, 1.37, and 1.27, accounted for 77.6% of the total matrix variance. The resulting four factors (composite ADHD scores) were labelled according to their clinical meaning: Factor 1 primarily consisted of inattention scores and hyperactivity/impulsivity scores rated by parents and clinicians, and was labelled Parent–Clinician Ratings. Factor 2 contained response time, response time variability, and ADHD score in the TOVA, and was labelled TOVA Sluggish Response. The main component of Factor 3 included omission errors, commission errors, and response sensitivity (d’) in TOVA, and was labelled TOVA Detectability. Factor 4 comprised inattention scores and hyperactivity/impulsivity scores rated by teachers, and was labelled Teacher Ratings. Figure 1 displays the trends of the four factors during the 24 month MPH treatment period.
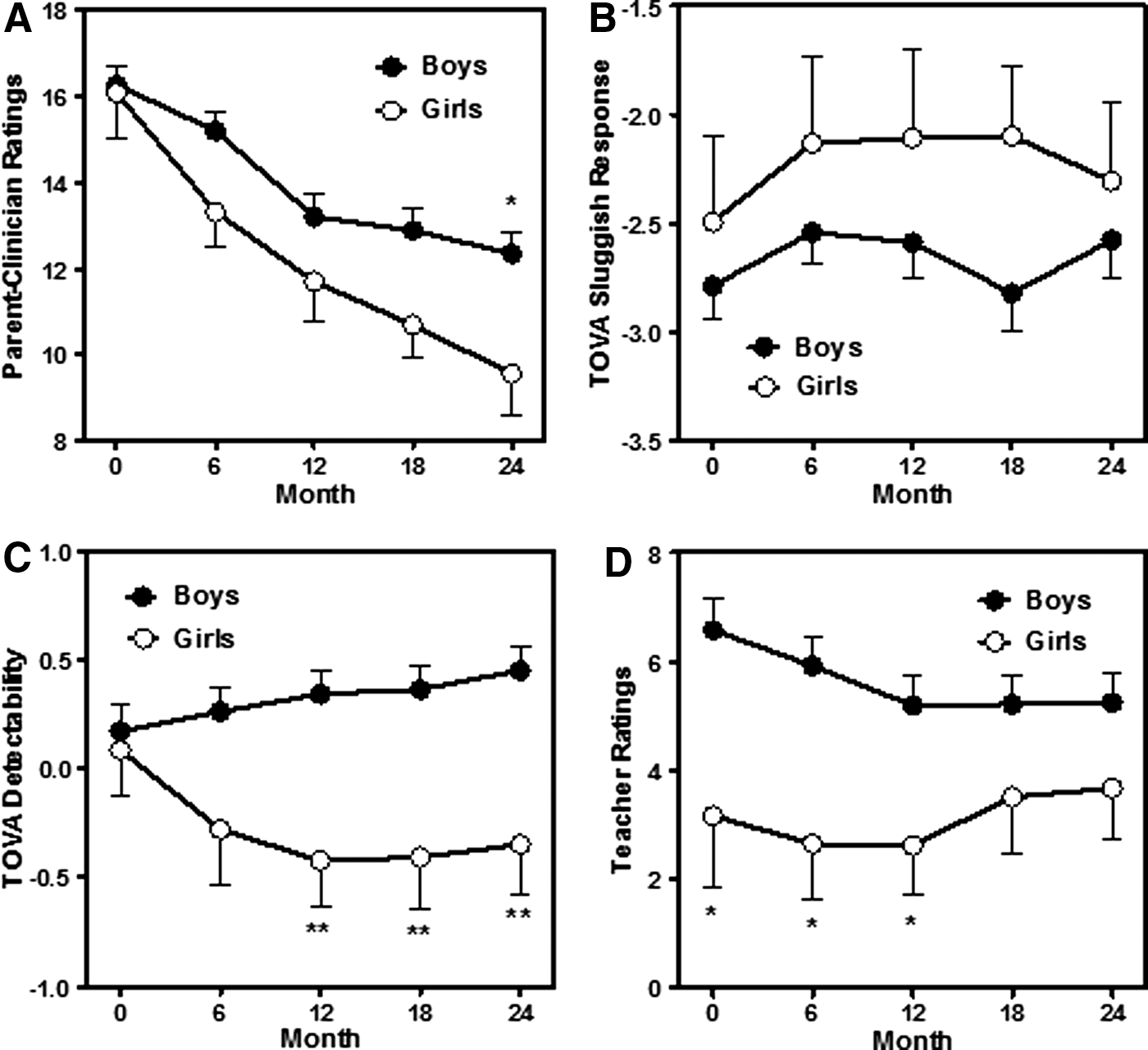
Changes over time in clinical symptoms and neuropsychological performance (Test of Variables of Attention [TOVA]) in boys (n=128) and girls (n=26) with attention-deficit/hyperactivity disorder (ADHD) during 24 months of methylphenidate (MPH) treatment. The Y axis represents the four composite scores of ADHD measurements reduced through principal component analysis:
Rotation method was Varimax with Kaiser Normalization.
Absolute value of factor loadings exceeding 0.50 are represented in boldface type.
TOVA, Test of Variables of Attention; ADHD, attention-deficit/hyperactivity disorder; ADHD-RS, ADHD Rating Scale; SNAP-IV, the Swanson, Nolan, and Pelham, Version IV Scale I, inattention scores; H, hyperactivity/impulsivity scores.
Table 3 demonstrates the effects of gender, time, and interactions of gender×time on each ADHD composite score; age, ADHD subtypes and mean doses of MPH were controlled for by including them as covariates in the analyses. According to Parent–Clinician Ratings, boys (β=−0.98, p<0.001) and girls (β=−1.62, p<0.001) significantly improved during the 24 month treatment with MPH. No significant difference was observed between genders; however, a significant interaction between gender and time (β=0.64, p=0.048) was noted. Post-hoc tests indicated that Parent–Clinician Ratings at Month 24 for girls were lower than the ratings for boys (β=2.79, p=0.018). The TOVA Sluggish Response in boys and girls did not significantly change over time. In addition, differences between genders and an interaction between gender and time were not observed. For TOVA Detectability, significant effects of gender and time were not noted; however, a significant interaction between gender and time occurred (β=0.17, p=0.031). Post-hoc tests suggested that TOVA Detectability significantly improved in boys (β=0.07, p=0.043), but not in girls. At Months 12, 18, and 24, girls performed worse than boys did in TOVA Detectability. Although a significant difference between genders was observed in Teacher Ratings during the study period (β=3.52, p=0.029), no significant interaction occurred between gender and time. Only boys exhibited a borderline significant improvement in Teacher Ratings (β=−0.33, p=0.053). Post-hoc tests indicated that Teacher Ratings were higher for boys than for girls at Months 0, 6, and 12; however, no significant difference was noted between genders at Months 18 and 24.
Data were analyzed using linear mixed model analysis
The post-hoc tests used repeated-measure analysis of variance (ANOVA), followed by a least significant difference (LSD) test.
p<0.05, ** p<0.01, *** p<0.001.
ADHD, attention-deficit/hyperactivity disorder; TOVA, Test of Variables of Attention.
Discussion
In the clinical sample of patients with ADHD over a 24 month treatment with MPH, the symptoms observed by parents and clinicians in both boys and girls substantially decreased; girls seemed to improve more than boys did. However, according to the teacher observations, the symptoms of the boys and girls did not decrease. Although boys were rated as exhibiting more severe symptoms by the teachers than were girls were during the first 12 months, the gender difference attenuated after 12 months. According to the neuropsychological test performance (TOVA), the trend of sluggish responses did not differ between genders. Nevertheless, TOVA Detectability improved among boys, but not among girls.
Gender differences in behavioral assessments by various informants
Previous studies have reported almost equal effects and safety profiles for both genders after short-term MPH administration (Cornforth et al. 2010). In addition, longitudinal studies that investigated the course of ADHD using behavioral assessments by parents or clinicians have suggested that males with ADHD are more similar than dissimilar to females with ADHD (Jensen et al. 2007; Monuteaux et al. 2010). The results of the present study differed from those of previous studies; parent-rated and clinician-rated symptoms improved more among girls than among boys. Possible explanations for this inconsistency are as follows. First, the study population was older (mean age: 13.1 years) than the mean age of participants in the aforementioned studies, and the sample size of girls was relatively small; the study population was nearer to being adolescents than young children, and the proportion of ADHD inattentive type (46.1%) was relatively higher than reported in previous surveys (Gau et al. 2008a; Willcutt 2012). In addition, the patients in our study received treatment with MPH. By contrast, the patients in previous longitudinal studies were either observed in a natural setting (Monuteaux et al. 2010) or received multimodal treatment (Jensen et al. 2007). The discrepancy in sampling and regimen might contribute to dissimilar findings. Moreover, Factor 1 derived from PCA in this study comprised parent ratings and clinician observations. Clinician-rated scores typically are based on temporary observation in a clinical setting and reports from caregivers (McConaughy et al. 2010). Boys with ADHD are often more fidgety and disruptive than girls at home and in clinical settings. Therefore, girls might appear to be improving more than boys during treatment.
Teachers might be more familiar with age-appropriate behaviors than parents are, and can compare patients with ADHD to their peers (de Nijs et al. 2004). Studies have demonstrated that the agreement between ADHD scores rated by parents and by teachers is low (Murray et al. 2007; Lavigne et al. 2012). Teacher reports, therefore, might particularly reflect first-hand observation of patient-learning situations and be more accurate than parental reports (Tripp et al. 2006; Wang et al. 2015). Based on the teacher reports in this study, the ADHD symptoms of boys only marginally improved; however, no improvement was noted among girls. Possible explanations for these results are that neither boys nor girls improved substantially in school during the long-term follow-up. Factor 4 (Teacher Ratings) comprised inattentive symptoms and hyperactive/impulsive symptoms. Boys were rated higher than girls at beginning of the study; however, the difference lessened after the 12th month of follow-up, possibly because of a regression to the mean. Moreover, in the study sample, a higher proportion of girls were classified as inattentive (73.1%). Hyperactive symptoms frequently lessen earlier than distractibility in the natural course of ADHD (Spencer et al. 2007). Compared with boys (who had more hyperactive/impulsive symptoms), improvement among girls was more difficult for teachers to observe. Although the ADHD subtypes were set as a covariate in the statistical analyses, the patient characteristics at baseline might still have influenced the trend of teacher reports.
Gender difference in trend of neuropsychological performance
Observational studies have suggested that stimulant medication produces long-term benefits in several cognitive dimensions of patients with ADHD (Epstein et al. 2006; Swanson et al. 2011). Cross-sectional comparisons have indicated that various neurocognitive profiles differ between males and females with ADHD (Gershon 2002; Hasson and Fine 2012). However, few studies have investigated gender differences in neuropsychological function during long-term MPH treatment (Zhang et al. 2011; Huang et al. 2012). The current study is the first to determine that the neuropsychological changes under MPH treatment over 24 months are possibly dissimilar between genders.
The TOVA, which is classified as a CPT, was used for neuropsychological assessment in this study. The data suggested that the composite score (Factor 2), containing response time, response time variability, and ADHD score according to the TOVA, did not significantly change over time among both genders. However, another composite score (Factor 3), which consisted of omission errors, commission errors, and response sensitivity (d’), improved only in boys. These results suggested that boys might benefit more in TOVA Detectability based on receiving MPH treatment for 24 months. This was a nonrandomized and open-label study. Therefore, whether the improvement observed in boys was derived from the greater effect of treatment with MPH, higher practice effects, or faster natural maturation in boys than in girls remains unclear. This gender-differentiated trend observed in TOVA Detectability contrasted with parent–clinician-rated ADHD behavioral symptoms (according to which girls improved more than boys). Neuropsychological functioning is not necessarily correlated with every domain of clinical ADHD symptoms (Epstein et al. 2003). Whether neuropsychological tests can serve as an indicator of functional impairment for ADHD remains controversial (Healey et al. 2011).
Limitations
This study had certain limitations. First, the sample size was small, particularly in the female group. Analysis of the gender effects associated with behavioral and neuropsychological changes had a low statistical power. Moreover, to avoid the confounding effects of nonpharmacological therapy, we excluded patients who required additional behavioral or family therapy. Given the exclusiveness of the sample, the generalizability of the sample might be limited. Second, information related to various critical factors that might influence the functional outcome (e.g., psychiatric comorbidities, intelligence quotient) was lacking. In addition, we did not identify whether or not female subjects were menstruating, at which stage in the menstrual cycle they were in at each test point, or whether or not they were taking contraceptives that could influence sex steroid levels. Furthermore, the treatment procedure of MPH was not standardized in this study. Drug adherence and additional nonpharmacological therapy were difficult to monitor over the long study period. These factors might have affected the estimation of gender differences. Third, because the design of this study was nonrandomized and open label, the behavioral changes might have been vulnerably inflated by a placebo effect and the normal development of the patients. Fourth, the severity of ADHD behavioral symptoms was measured using raw scores; however, the TOVA performance was analyzed using a Z score (age adjusted). Moreover, the TOVA was administered at a single time on a day when patients had not taken medication, and the ratings for the behavioral symptoms of patients might have been based on general impressions over the previous few days. Therefore, comparisons of the trends in behavioral symptoms and TOVA performance might not have been completely unbiased. Finally, although the ratings of behavioral symptoms were performed by the same informants at each visit, some of the teachers might have changed because the patients moved to a higher grade in school. These inevitable variations in interrater reliability might have affected the results.
Conclusions
The results of this study suggested the potential gender effects on behavioral profiles established according to information from multiple informants and neuropsychological performance in patients with ADHD over 24 months of MPH treatment. The clinical symptoms of boys and girls obtained from parents and clinicians differed from those observed by teachers; the genders differed among various composite indices of TOVA performance. Therefore, gathering comprehensive information from patients with ADHD is essential to determining the functional outcome for patients and differences between genders. A future longitudinal study containing a large sample size is warranted to ascertain how gender modifies the functional outcome of ADHD.
Clinical Significance
Gender might modify the behavioral trends observed by various informants and the neuropsychological performance of ADHD patients during long-term treatment with MPH. According to parents and clinicians, girls' ADHD symptoms improved more than boys' did. However, teachers did not perceive significant improvement in ADHD symptoms in either gender. Based on neuropsychological test performance (TOVA), a composite score consisting of omission errors, commission errors, and response sensitivity (d’) significantly improved in boys, but not in girls. Gathering multidimensional information from patients with ADHD is essential to determining the functional outcome for patients and differences between genders.
Footnotes
Acknowledgments
The authors thank Wei-Tsun Soong for providing the Chinese version of the K-SADS, and Shur-Fen Gau for providing the Chinese version of the SNAP-IV scale.
Disclosures
No competing financial interests exist.