
Abstract
Objective:
Given that childhood anxiety disorders are common and frequently undertreated, novel treatment platforms are needed. The current article explores the potential for mobile device-based (m-health) applications, to expand access to evidence-based treatment.
Methods:
This article reviews the relevant literature regarding barriers to disseminating evidence-based treatment, the potential benefits of the m-health platform, standards for evaluating m-health interventions, and currently available applications.
Results:
Although a large number of m-health applications for anxiety are available, the vast majority of them are inconsistent with therapy protocols supported by the child anxiety treatment literature. The relatively few m-health applications based on evidence-based practice have not yet been examined empirically.
Conclusions:
Realizing the potential of m-health for child anxiety will require addressing the uncertainty around the necessary and sufficient components of cognitive-behavioral therapy (CBT), as well as the common challenges associated with delivering interventions via information and communication technology. Mayo Clinic Anxiety Coach is an m-health application designed by the author and colleagues to be consistent with exposure-based CBT and principles for effective intervention delivery via information and communication technology. Recommendations for identifying, using, and developing m-health applications for childhood anxiety disorders are presented.
Introduction
A
One of the primary barriers to children receiving effective care for anxiety is the lack of therapists providing evidence-based treatments (EBTs) (Goisman et al. 1993; Goisman et al. 1999; Freiheit et al. 2004; Craske et al. 2009; Kazdin and Blase 2011; Hipol and Deacon 2013). For child anxiety, a general consensus exists that EBT includes the use of exposure therapy (Marks 1969; Barlow 1988; Silverman and Kurtines 1996; Kazdin and Weisz 1998; Clark 1999; Beidel et al. 2000; Davis and Ollendick 2005; Kendall et al. 2005; Carey 2011; Tiwari et al. 2013). However, practitioners in clinical settings rarely use in vivo exposure (33%) relative to other cognitive-behavioral therapy (CBT) strategies such as cognitive restructuring (97%) and relaxation (80%) (Freiheit et al. 2004; Hipol and Deacon 2013). Even if more practitioners provided EBTs, their numbers are insufficient to meet the population's psychiatric needs (Kazdin and Blase 2011). Therefore, in order to adequately treat anxious children, new technologies will need to not only improve the quality of care provided in traditional settings, but also allow patients to receive interventions with minimal professional contact.
The Potential of m-Health Applications
Mobile device-based (m-health) applications present a promising medium for providing empirically supported treatments to therapists and directly to patients. To begin with, smart phones provide a platform that can reach a large portion of the population, including underserved groups. As of January 2014, 58% of the United States population owned a smart phone (Pew Research Center 2014). In underserved populations, rates are 47% for low-income households, 43% for rural areas, and are higher for minorities than for Caucasians. Moreover, the vast majority of the population will likely own smartphones in the near future, as 90% currently own a cell phone, and the percentage of smart phones versus traditional cell phones has been rising (Nielsenwire 2012; Pew Research Center 2014). Overall, these data suggest that smart phones are currently, and will be increasingly, a convenient medium for reaching individuals of all ethnicities and income levels, and from all geographic regions.
Given the ubiquity of smart phones, m-health applications may be a cost-efficient means of disseminating EBTs for childhood anxiety disorders. Moreover, m-health application have a number of capabilities that have been associated with successful interventions utilizing information and communication technology (ICT), including: 1) Scheduled reminders to engage in therapeutic exercises (Glasgow et al. 2004), 2) point of performance support (Heron and Smyth 2010), 3) individually tailored information (Fjeldsoe et al. 2009; Bauer et al. 2010; Burke et al. 2011), 4) real-time symptom assessment (Piasecki et al. 2007), 5) readily accessible asynchronous communication (Fjeldsoe et al. 2009), and 6) attractiveness to youth through increased sense of autonomy (Boushey et al. 2009; Long et al. 2010). As such, m-health applications present a readily accessible and engaging platform for reaching therapists and patients.
Standards for Developing Child Anxiety m-Health Applications
Regardless of the availability and technological versatility of smart phones, m-health application will only be as effective as their clinical content. As such, providing effective care via m-heath applications must begin by adapting the traditional EBT literature to this novel platform. Exposure-based CBT for childhood anxiety is the therapy with the most empirical support (Manassis et al. 2010) and is a natural starting point for m-health development. These protocols typically begin with six to nine sessions of anxiety management strategies (emotion identification, relaxation, problem solving) followed by six to eight sessions of exposure (i.e., (Kendall 2000; Walkup et al. 2008).
Unfortunately, the empirical support for the child anxiety CBT model is less developed than that for other fields, and there is not a clear consensus on the necessary and sufficient treatment components ( James et al. 2009; Ale and Whiteside 2015). For example, child anxiety CBT is not consistently more effective than other forms of therapeutic contact (Silverman et al. 1999; James et al. 2009), treatment as usual (Barrington et al. 2005; Southam-Gerow et al. 2010), or medication (Walkup et al. 2008), standards that have been met by CBT for other disorders (Gould et al. 1995; Gould et al. 1997b; Barlow et al. 2000; Abramowitz et al. 2005; Gilboa-Schechtman et al. 2010; Storch et al. 2013). This shortcoming likely results from the emphasis on cognitive and relaxation strategies, which may not improve outcomes above providing exposure alone (Feske and Chambless 1995; Gould et al. 1997a; Ollendick and King 1998; Deacon and Abramowitz 2004) and might reduce effectiveness ( Foa et al. 1999; Schmidt et al. 2000; Foa et al. 2005; Craske et al. 2006; Vande Voort et al. 2010). Therefore, although the traditional treatment outcome studies can guide the content of m-health applications for childhood anxiety, this literature is not definitive.
In addition to having a foundation in established therapeutic principles, m-health applications must also capitalize on the literature pertaining to the design and testing of ICT for health behavior change (Ritterband et al. 2009; Proudfoot et al. 2011). For example, given that retention can be a challenge for ICT interventions (Rosser et al. 2009), m-health applications should be engaging to users, minimize burden by incorporating appealing colors and screen layouts, provide intuitive and concise functionality, encourage interactivity through self-tests and self-monitoring, and allow for human support (Brouwer et al. 2008; Ritterband et al. 2009; Rosser et al. 2009). In addition, to maximize behavior change, applications should include individually tailored content, point of performance feedback, and personally relevant information (Brouwer et al. 2008; Fjeldsoe et al. 2009; Burke et al. 2011).
Ultimately, m-health applications must be held to the same efficacy standards as other ICT interventions. These include the gold-standard randomized controlled trials establishing symptom reduction superior to waitlist or placebo. Moreover, empirical investigations should a) quantify the appropriate dose of intervention and the degree of professional assistance needed to benefit from the application, b) measure behavior change (i.e., exposure) hypothesized to lead to symptom improvement, and c) assess safety, data security, and tolerability (Ritterband et al. 2009; Proudfoot et al. 2011).
In summary, there are at least three general standards that can be used to evaluate m-health applications for child anxiety: 1) Consistency with the traditional treatment literature (e.g., exposure-based CBT); 2) design and functionality that maximizes engagement and retention; and 3) empirical evidence demonstrating the degree of improvement that can be obtained with the prescribed level of use and support.
Existing m-Health Applications for Anxiety
Available m-health applications can be divided into three groups, none of which meet the above-described standards. The largest group includes hundreds of applications that can be easily found through a search of the App store, Google play, and the Internet. The majority are directed at adults or do not specify an age range, with a much smaller number being specifically designed for children. These programs typically do not target a specific anxiety disorder, but rather refer to unspecified anxiety, worry, or stress. They most commonly provide instruction and guidance in relaxation strategies and self-hypnosis. As such, the vast majority of the available m-health applications do not meet the first criteria of being consistent with the literature on EBTs for childhood anxiety disorders, i.e., exposure-based CBT.
A second group consists of only a handful of applications offering CBT principles. For example, Smartphone-enhanced Child Anxiety Treatment (SmartCAT) is an application on the Android platform designed to be used with therapist-provided face-to-face treatment (Pramana et al. 2014). MindShift is another example of an m-health application that is generally consistent with CBT principles and includes exposure activities. However, although these applications meet the first criteria of consistency with CBT, they reflect the uncertainties of the traditional treatment literature and present exposure as one of multiple treatment components. As such, users (like therapists) may be more apt to use relaxation and cognitive tools, rather than using exposure, even though the latter is more likely to be effective in the long term. A final group of applications have a clear focus on exposure. These applications tend to focus on a single disorder such as Live OCD Free for children and adults with obsessive compulsive disorder or PE Coach (Reger et al. 2013) designed to augment therapist-directed prolonged exposure for adults with posttraumatic stress disorder.
The existing CBT-based m-health applications for child anxiety vary in the degree to which they meet the second standard regarding design and functionality. The majority of them promote interaction through self-tests, ratings, and entry of symptom-related information. However, at this time, no m-health applications have sufficient research support to meet the third standard. Of those mentioned, SmartCAT has data supporting its acceptability to therapists and youth when used in conjunction with face-to-face therapy (Pramana et al. 2014). The only successful randomized controlled trial to date supported the superiority of a CBT m-health application for adult social anxiety disorder compared with an interpersonal psychotherapy application (Dagoo et al. 2014). In contrast, an attention modification training application has been found to be more effective than waitlist, but not more effective than a control training condition (Enock et al. 2014). Beyond these studies, there are only cases studies describing the use of Mayo Clinic Anxiety Coach for pediatric obsessive compulsive disorder, and a serious game application for adult specific phobia (Botella et al. 2011; Whiteside et al. 2014).
Mayo Clinic Anxiety Coach
Mayo Clinic Anxiety Coach is a self-help application on iOS (the operating system for the iPhone, iPad, and iPod Touch) designed to meet the need for m-health tools consistent with exposure-based CBT and research on effective ICT interventions (see Fig. 1). The content consists of three modules: Self-Evaluation, Psychoeducation, and Exposure. The Self-Evaluation module measures the frequency of anxiety symptoms with a self-report Likert-type scale. Users of the application can also track their progress over time by providing daily ratings of their symptom severity. The second module contains psychoeducational material on the use of the application, the cognitive-behavioral conceptualization of anxiety, descriptions of each anxiety disorder, explanations of CBT, and guidance for accessing other forms of treatment.
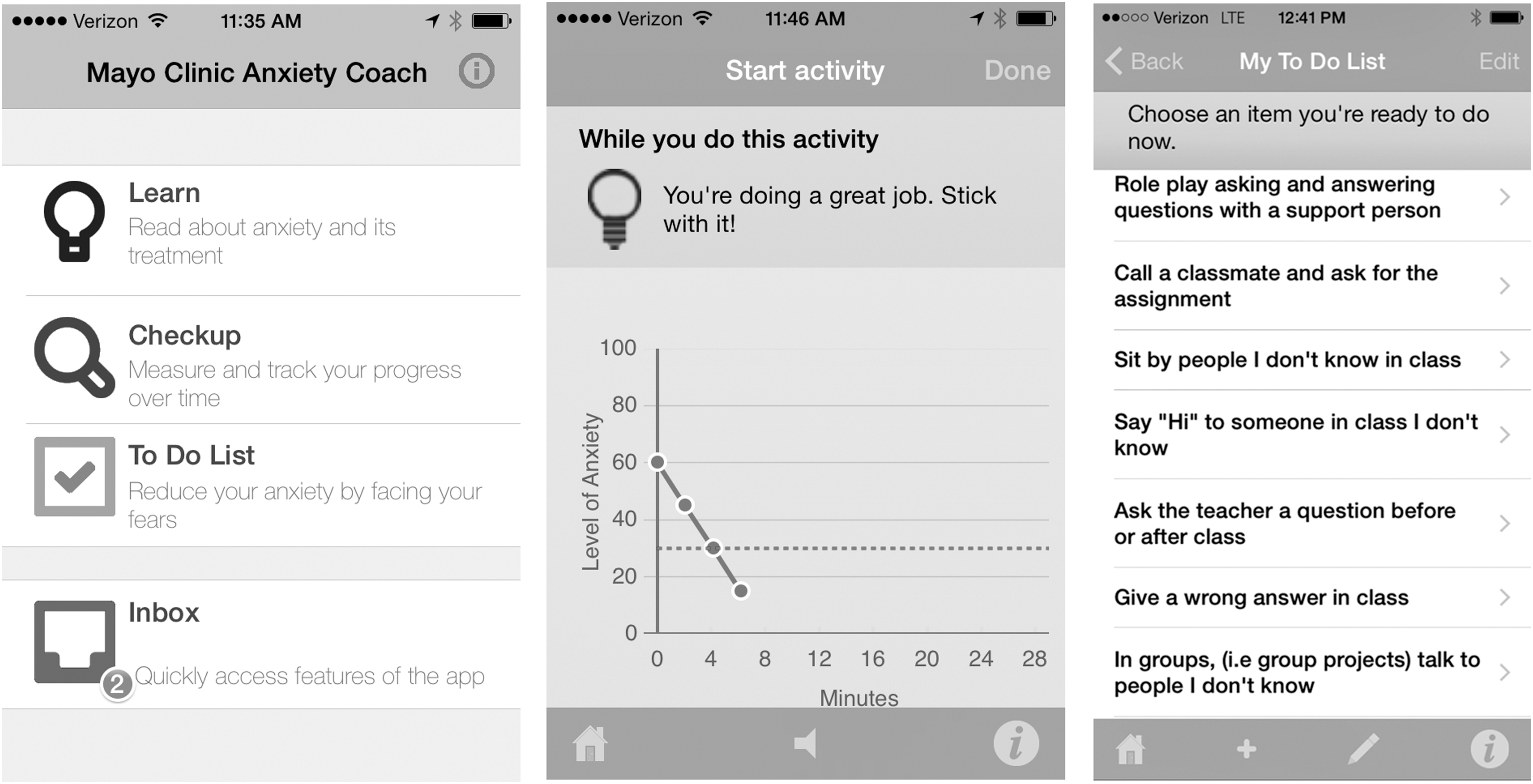
Mayo Clinic Anxiety Coach screen shots.
The central component of Anxiety Coach is the third module, which guides users (adults, adolescents, or children with the help of a parent) through exposure exercises. Individuals can select from ∼ 100 pre-made fear hierarchies that outline graduated exposure exercises for a wide variety of anxiety symptoms (fear of social situations, panic attacks, fear of separation from parents, general worry, obsessions and compulsions, trauma, and specific fears) or create their own. Once a hierarchy is established, Anxiety Coach guides the individual through the completion of exposure in real-world situations. This process includes assessing the likelihood and severity of negative outcomes, tracking anxiety graphically during an exposure (in vivo, imaginary, or interoceptive), receiving prompts to continue until the anxiety has decreased, and evaluating the outcome of the exposure. Users can record their success by marking items of the fear hierarchy as mastered, and reviewing their history of completed exposures.
Mayo Clinic Anxiety Coach has four features that differentiate it from other m-health programs for anxiety. To begin with the material is applicable to individuals across the age range and covers the full spectrum of anxiety symptoms, including 24 fear hierarchies related to social, separation, and specific phobias commonly associated with children and adolescents. Second, the clinical content has a clear focus on exposure, the evidence-based active ingredient of treatment. Third, the library of exposure hierarchies provides detailed guidance on how to plan and execute exposure for different symptoms. Finally, results from the self-assessment and creation of a unique fear ladder provide interactivity and personally relevant content to foster retention.
Examination of the user data for the first year that Anxiety Coach was available indicates that at least 169 children and adolescents (likely with a parent) downloaded the application. These subjects ranged in age from 5 to 17 (mean=13.86, SD=3.1) and were primarily girls (65.1%). The median number of usages was 7, with the majority (∼70%) accessing the application between 4 and 20 times. These data suggest that most children (or parents) found the application engaging enough to return to multiple times. Examination of usage patterns of all users (2449 adults and children and adolescents) suggests that users were more likely to take the self-assessment (62.3%) than to create a fear ladder (37.4%) or complete an exposure (4.7%). Further data are needed to understand how individuals used the application, what their experience was like, and how to engage them more fully with the application.
Conclusions and Future Directions
In summary, m-health applications hold great promise for improving the treatment of children and adolescents with anxiety disorders, by increasing access to exposure-based CBT. Rather than replacing clinician-administered therapy, m-health may be most beneficial by enhancing therapy. For example, m-health can facilitate the adoption of evidence-based treatment procedures by community therapists, and provide the clinician with more information about patient adherence between sessions. As such, m-health applications may help clinicians treat children more effectively and efficiently. Realizing this potential will require addressing the uncertainty around the necessary and sufficient components of CBT, as well as the challenges common with ICT interventions (i.e., low retention). Although there has been a flurry of activity developing such applications, much more needs to be done in evaluating the utility of these applications.
Disclosures
Dr. Stephen Whiteside and the Mayo Clinic receive royalties from the sale of Mayo Clinic Anxiety Coach.