
Abstract
Objective:
The purpose of this study was to describe the potential and limits of school telemental health (TMH) to support a full continuum from mental health promotion to intervention, particularly for students less likely to access community care.
Methods:
A review of school TMH literature and model programs, and of data from focus groups with child psychiatry fellows, was undertaken to inform best practices and future directions for TMH in schools.
Results:
Existing data suggest that TMH with children and adolescents is promising and well received. Child and adolescent psychiatrists use various models for conducting school-based TMH, which differ in the level of direct care and types of services provided. Literature review and focus group data suggest that advantages of school TMH include greater efficiency, the capacity for higher volume, and increased access to care for many students who would be unlikely to reach traditional community mental healthcare because of barriers such as transportation and healthcare coverage. Disadvantages of school TMH service provision include patient concerns about their own privacy as well as concerns related to the psychiatrist's ability to effectively engage families in care without being present in person. Fellows also noted that the training experience of physically being in the school building and experiencing the school expectations and culture helps them move toward greater appreciation and understanding of the structures, policies, and opportunities and challenges for schools and school-based professionals. Most agreed that a “hybrid” model of care, with some in-person and some TMH care may be most beneficial to all parties, promoting both engagement and efficiency simultaneously.
Conclusions:
School TMH should be considered as part of a comprehensive service delivery system for students, in order to address shortages and gaps in specialty child and adolescent mental healthcare, and to maximize efficiency and productivity.
Introduction
T
Mental Health in Schools
The President's New Freedom Commission on Mental Health (Hogan 2003) identified school as an important setting for providing mental health services, with higher follow-up rates than in traditional community mental health settings. In one study, for example, 96% of students in school-based mental health care followed up with treatment services versus only 13% of students in a traditional community mental health center (Catron et al.1998). Shortage of specialty mental health providers, particularly child and adolescent psychiatrists, further supports the case for bringing behavioral healthcare to children's natural settings, including schools (Faulkner et al. 2011; Comer and Barlow 2014). Several national associations, including the American Psychological Association, the American Federation of Teachers, and Mental Health America, as well as numerous researchers and practitioners, have publicly stated support for increasing access to high quality mental health services in schools (Astor et al. 2012). Most recently, a presidential-appointed task force and President Obama have endorsed the need for increased mental healthcare in schools (Office of the White House 2013). Related to increased access, decreased stigma, opportunities to provide both mental health promotion and treatment, and greater outreach to youth with internalizing disorders, schools have proven a valuable site for mental healthcare provision. School- or district-employed student support staff (e.g., school psychologists or school social workers) often provide foundational support for students' mental health needs, particularly for those receiving special education programming. However, schools typically report significant need for additional student mental health supports within the school building, from mental health promotion to prevention to intervention, to meet the full continuum of student mental health needs. This need is often addressed through community-partnered models, in which community mental health agencies and providers contract with the district or individual schools to augment existing services (Paternite and Johnston 2005; Weist 2005).
Psychiatry in schools
When providing services in schools, it is important to have access to an interdisciplinary mental health team in order to address the broad array of concerns that may impact students. Examples of disciplines that can be represented in a school mental health team include: Social work, psychology, nursing, occupational therapy, counseling, and psychiatry, with psychiatry often the least-represented discipline on teams, because of high costs and shortage of providers. In fact, psychiatric consultation and medication management are the least commonly available services in school mental health. For example, in a survey conducted in the state of Maryland, a state with relatively progressive school mental health programming and reach, it was found that as a part of community-partnered school mental health programming only 50% of the 24 jurisdictions (n=12) were providing medication management, either by a psychiatrist or other health provider, and only 33% (n=8) were providing psychiatric consultations, which may or may not have involved direct treatment, as compared with 100% of jurisdictions offering individual counseling, and 83% (n=20) offering group counseling services. For jurisdictions with only school employees providing mental health services, 38% (n=9) were providing medication management and only 8% (n=2) were providing psychiatric consultation, as compared with 100% of jurisdictions offering individual counseling and 91% offering group counseling services (Maryland School Mental Health Survey 2009).
The type and extent of consultation provided by psychiatrists to schools varies tremendously (Walter and Berkivitz 2005). Given the shortage of child and adolescent psychiatrists, the amount of available psychiatry time is often quite limited, with some psychiatrists conducting school visits less than once per month for a given school or program. With such limited time, often psychiatrists only provide general clinical oversight and guidance to school mental health program leadership and/or staff (e.g., a psychiatrist may serve as the program medical director without providing direct services). Psychiatrists may offer general program or case consultation about individual students, often funded via school/district or mental health program funding, as opposed to fee-for-service activities. Some school mental health programs do engage psychiatrists as direct service providers, in which psychiatrists provide psychiatric clinical assessments, medication management, and assistance with treatment services, often for only a very small percentage of students with the most complex or intensive needs. Typically, when direct service provision by a psychiatrist is offered in schools, it is conducted in collaboration with an on-site school mental health therapist, either school employed or community partnered, who serves as the primary clinician for the student. The clinician typically coordinates all aspects of the appointment (e.g., setting up a time, outreach to family, collecting feedback from teachers, getting the student from class for the appointment), with the psychiatrist's time maximized for face-to-face provision. Even with this efficiency, a significant amount of time for the psychiatrists is lost traveling to and from the school setting and waiting for youth and families to show up for appointments. This travel burden, in turn, restricts psychiatrist availability for providing care to other children in need, illuminating the broader public health impact of requiring psychiatrists to travel, given their scarcity.
Telehealth and TMH in Schools
Over the past decade, telehealth services have become increasingly common in schools, both for the provision of physical and behavioral health. School-based health centers (SBHCs) have spearheaded much of this effort, with substantial funds being allocated toward their construction and operation in recent federal legislation (SBHC H.R. 2632—113th Congress 2013). For example, a school-based telemedicine program run by the Community Health Center of Branch County, Michigan, has been using telemedicine to perform primary care services for acute illnesses such as ear infections, strep throat, and influenza, as well as to identify medical issues such as cardiac abnormalities and musculoskeletal injuries (
Given the importance of schools as a venue for providing mental health support and treatment to youth, and the success of telehealth services in schools, TMH has been increasingly considered a mechanism to provide access to specialty mental health consultation and treatment. Use of TMH in schools may create the potential for greater efficiency and productivity, while still maintaining client satisfaction and effectiveness and allowing greater choice for students in how they access services (Grealish et al. 2005; Hilty et al. 2013). Further, by making psychiatric care in schools more feasible, TMH can offer greater opportunity to support a multidisciplinary team approach to school mental healthcare, bringing together psychiatrists with educators, and other health and mental health professionals.
There is already evidence for the effectiveness of TMH with children and adolescents, and for youth and family satisfaction with the use of TMH delivered to natural settings, including primary care settings (Myers et al. 2008; Hilty et al. 2013) and home settings (e.g., Comer et al. 2014). In fact, some studies have found that clients prefer and share more information with the use of technology than they do in person (Grealish et al. 2005; Hilty et al. 2013). Although often implemented in rural settings, school-based TMH has demonstrated success in urban settings as well, with many of the same benefits. Models of urban TMH have proven helpful to enhancing service access for youth and families, specifically (Spaulding et al. 2011). In both rural and urban settings, school-based TMH may help improve appointment compliance (because the child is already in school), provide seamless coordination with the therapists embedded in the schools, and improve communication with teachers and administrators. Even in an urban setting, TMH eliminates the barrier of travel to various sites, allowing the child psychiatrist to see and consult about more students in more schools, thereby increasing access to a larger population.
School TMH offers many potential advantages to families. Access to TMH in schools may reduce parental travel time (schools are most often zoned according to home address), resulting in financial savings from decreased travel expenses as well as reducing the amount of parental time lost from work. There is even the possibility for parents to join the psychiatrist–student session remotely from their workplace or home. Additionally, parents are familiar with the school environment and staff, and this may promote better provider connectedness and treatment engagement, with less stigma. For parents with other school-age children, appointments during the school day at the school can make it easier for the parents to not have to negotiate child care for their other children when they have appointments. With the ability to have multiple participants in a session, including teachers, administrators, and student support staff, parents may be able to hear directly from school personnel about their child's daily behavior, peer interactions, and learning issues, to ensure that the academic and behavioral health concerns are well integrated into treatment strategies.
Consistent with other models of school-based psychiatric support, school TMH is not limited to medication management. For example, school TMH can be used to evaluate students for support services (e.g., individualized education program [IEP], 504 planning), or brief psychotherapy), to clarify diagnoses and assist with case conceptualization, consider physical factors that are impacting mental health, and promote more integrated care in collaboration with teachers, school administrators, and outside providers. Psychoeducation on psychopathology and medications may be provided to school clinicians to promote accurate diagnoses and treatment planning, and referrals for educational and/or psychological testing. TMH can also be used to facilitate professional development by off-site providers, such as educational seminars for teachers, other school staff, and administrators.
School TMH Program Examples
Following the expansion of telehealth for physical healthcare in schools, school TMH programs are increasingly being established. In the absence of a database or repository of existing school TMH programs, it is difficult to determine the reach of current services. Therefore, we will describe a few long-standing school TMH programs that reflect diversity of intervention and audience.
In 2006, the University of Texas Medical Branch established TMH services in seven Galveston area schools with the aim of increasing access to behavioral healthcare. This program connects TMH services to established school-based primary care clinics called “Teen Health Centers,” and provides mental health assessment as well as on-site case management. The program also utilizes a web-based electronic medical record system that is accessible from any location, and promotes interprofessional collaborative care to achieve better health outcomes (
In addition to direct clinical care and consultation, TMH technology has been used in schools to enhance the capacity of school professionals to support student mental health. Videoteleconferencing (VTC) equipment allows the opportunity for staff, regardless of their location (rural or urban), to participate in new and ongoing training opportunities. According to Barnett et al. (2012), when school staff are geographically removed from treatment centers, they often have little to no accessibility to professional development workshops. VTC provides a cost-effective opportunity to train groups of teachers, administrators, and other appropriate school staff in important and emerging topics, allowing for open discussions and exchange of ideas and strategies.
University of Maryland School TMH Spotlight
History
Since 2004, the National Center for School Mental Health at the University of Maryland School of Medicine has been utilizing telehealth services in three of its clinical programs. Initially, videoconferencing systems were installed in the downtown Baltimore medical school campus and at two public schools, one elementary/middle and one high school. In an effort to pilot the technology, the equipment was first used by medical professionals to provide educational programming to students in a high school health class and in a small middle school peer group on health topics, including alcohol and tobacco prevention. The early videoconferencing equipment was cumbersome because of its weight and size (it was stored in a large, heavy cabinet, limiting mobility). In addition, it took considerable effort and resources to install lines at each individual school with the necessary bandwidth to conduct TMH. Despite these challenges, feedback about the technology and its facilitation of access to the medical campus was overwhelmingly positive among school staff, students, and medical professionals. Since the initial pilot, updated and improved videoconferencing equipment has now been installed in several schools across the Maryland programs, and is utilized for a variety of services to support student mental health, including classroom trainings on mental health in schools, consultation with school mental health staff and teams, and direct service provision.
Model
Two of the Maryland programs with TMH services are supported by a partnership of the state and local education authorities, and provide multidisciplinary (psychiatry, psychology, social work, counseling, case management, family support) care to students with complex emotional and behavioral difficulties who are at risk of moving to more restrictive educational placements. For these students, the education system funders mandate that psychiatric consultation be offered as part of the service array, and TMH was the most feasible way of offering this care with consideration of geography and scheduling demands. Given limited access to psychiatry time, eliminating the need for travel and creating a streamlined service structure has maximized clinical service provision and consultation time.
Psychiatry fellows as school TMH providers
Current child and adolescent psychiatry fellowships are not consistently designed to provide training in school-based or TMH work. As part of the University of Maryland School of Medicine Child and Adolescent Psychiatry Fellowship, the Center for School Mental Health faculty and staff have developed a comprehensive model of interdisciplinary school mental health training that considers unique skills, knowledge, and guiding principles for effectively providing school-based services, including school TMH. All second year psychiatry fellows participate in a year-long school mental health rotation, which includes some time spent providing TMH to students in schools across Maryland, including in both rural and urban settings. Figure 1highlights the clinical rotation expectations within the school mental health program for child and adolescent psychiatry fellows. It is expected that across the school year, fellows will have exposure to all training components, with items in the center of the circle (see Fig. 1) occurring at the greatest frequency during the training experience. TMH is currently being used to conduct many of these activities, including psychiatric consultations, mental status examinations, cross stakeholder collaboration, medication management, and participation in team meetings. All of these training efforts appear to positively impact the workforce with respect to readiness to provide and interest in providing school-based care, including school TMH; 26% of the 31 child and adolescent psychiatry graduates over the past 5 years are working or have worked in a school-based mental health program, and 20% are involved in TMH. Several graduates have incorporated TMH into their private practice by providing direct care both to local clients and to rural health centers.
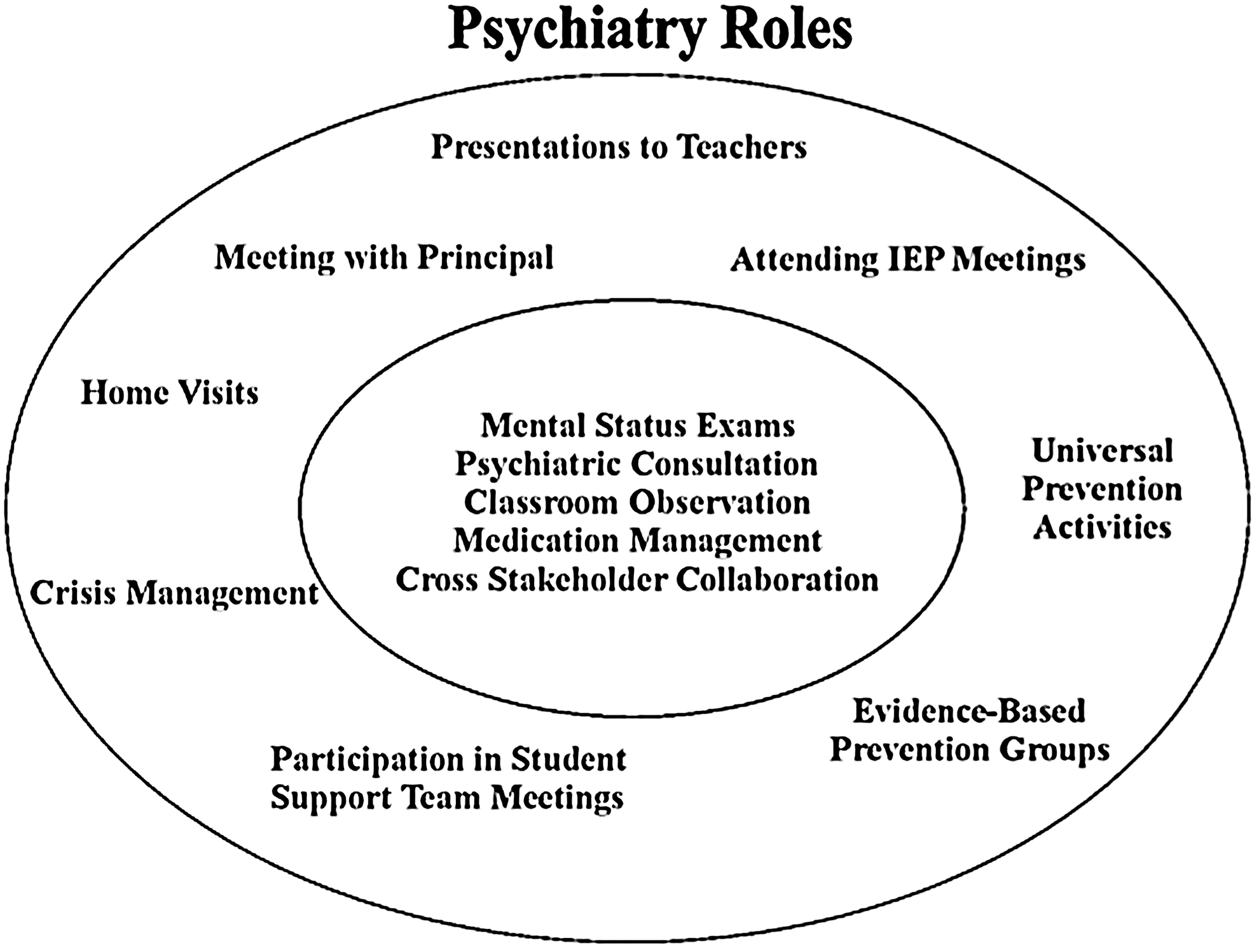
Primary and secondary roles for psychiatrists in schools.
Consultation protocol
Child and adolescent psychiatry fellows, all supervised by a senior faculty psychiatrist, are scheduled into a regular TMH time block, during which they are able to provide consultation to school staff and direct consultation to students and families. Each participating school has a primary clinician, usually a social worker or counselor, who is employed by the Maryland clinical program. This clinician serves as the primary clinician for the clients who will be served through the TMH. The clinician coordinates all logistical aspects of the TMH session from scheduling, collecting, and sharing necessary data with the psychiatrist, to ensuring that youth and families are in attendance. The clinician ensures efficiency and works with the psychiatrist, family, and school team to best maximize the use of the psychiatric face-to-face time with students and families.
Typically, clinical considerations discussed as part of the TMH consultation with psychiatrists involve differential diagnosis, medical issues that may underlie or be comorbid with psychiatric presentation, psychotropic medication considerations, and connection to community providers, including community-based psychiatrists and primary care providers. Consultations related to the need for, effectiveness of, or response to medications are often considered during consultations, although prescribing or ongoing medication management is very rare within the TMH service within the two programs; it is preferred that medication management occur through community service providers who can have more regular contact and are in closer proximity to the youth. In these cases, a consultation report from the TMH session(s) may be shared with the prescribing physician. On rare occasions, a prescription may be provided to bridge the time between the TMH session and the time that the patient can be seen by a psychiatrist or other medical practitioner. Direct care is documented in the student's mental health record, which is maintained by the school clinician in accordance with outpatient mental health center privacy regulations, and kept separate from their school academic records.
Parent involvement
Parental consent is obtained for direct consultation on cases, but not when the psychiatrist is consulting to school staff about an unidentified student or about more pervasive issues within a classroom or school setting. The amount of parental involvement reflects the nature of interaction. For example, parents are part of a session when conducting an individual session related to case conceptualization or medication, but may not be part of a session when the psychiatrist is providing more general school consultation.
Equipment and technical support
Currently, this TMH service uses standards-grade equipment with secure point-to-point connectivity such as a T1 line. Should technical problems and questions arise, TMH providers can receive support from the telehealth department in the school program's affiliated hospital system as well as from the technology/information system division within the school.
Future directions
Although the University of Maryland programs have primarily provided consultation services to date, plans are underway to further integrate TMH into direct care services. For the 2015–16 school year, faculty will test the relative feasibility, impact and satisfaction with three different models of school-based psychiatric care: In person, TMH only, and a “hybrid” model combining in person care with TMH. In all models, medication management will follow current prescribing considerations for schools, which generally dictate prescribing and management of only relatively low-risk medications, including stimulants, α agonists and antidepressants (selective serotonin reuptake inhibitors [SSRIs]). When students need multiple medications or medications that require more frequent monitoring, they are typically referred to providers in the community.
Experience and Recommendations of School TMH Providers
A recent focus group with six psychiatry fellows at the University of Maryland Division of Child and Adolescent Psychiatry provided insight into their overall experience using school TMH, including advantages and disadvantages of this service delivery model. Their views were relatively consistent with the literature from children, families, and providers on the perceived advantages and disadvantages of TMH (Grealish et al. 2005; Myers et al., 2008; Hilty et al. 2013). Reported advantages included greater efficiency (decreased commute time, easier scheduling), the capacity for higher volume (by serving several schools in one afternoon), and increased access to care for many students who would be unlikely to make it to traditional community mental healthcare facilities because of barriers such as transportation and lack of healthcare coverage. Reported disadvantages of school TMH service provision included patient concerns about their own privacy (even though all protocols fall within accepted federal privacy regulations) as well as concerns related to the psychiatrist's ability to effectively engage families in care without being face to face with them in person. Finally, the fellows noted that the training experience of physically being in the school building and experiencing the school expectations and culture is critical to the psychiatry workforce and to their professional development, helping them move toward greater appreciation and understanding of the structures, policies, and opportunities and challenges for schools and school-based professionals. Most agreed that a “hybrid” model of care, with some in-person and some TMH care, may be most beneficial to all parties, promoting both engagement and efficiency simultaneously.
TMH Considerations in Schools
Technology
It cannot be assumed that schools will have the infrastructure and resources to support advanced technology that may be required by TMH, or that school-based staff will have the technology understanding and skills to successful negotiate the TMH equipment. For example, within one of our clinical programs, it took a year to negotiate the necessary wiring and Internet requirements with the school technology team and the university. Many schools, particularly in more rural and poorer urban communities, may lack the infrastructure and finances needed to support more sophisticated TMH technology such as larger scale VTC systems with high definition, point-to-point-connectivity with 1.27–2.28 meter TVs, security that supports the systems, and data centers with infrastructure to ensure encryption of all information. Some schools may not have access to high-speed Internet technology, and fire walls to protect privacy may make it difficult to access the Internet and needed technology within the school building. As TMH technology has evolved, however, the infrastructure needs have lessened, allowing for greater access by schools with less-than-sophisticated equipment capacity. TMH can be conducted using consumer-grade technology such as desktops, laptops, or tablets with an inexpensive web camera as long as both rooms being used (one for the practitioner and one for the patient) are private and sound-proofed in order to protect patient privacy. Unfortunately, finding confidential, private, and secure space to hold TMH conversations and even to safely store equipment can be quite challenging in overcrowded schools where space is very limited.
School policies and structures
Providing school TMH services requires collaboration with and respect for school personnel, and must reflect and be considerate of the policies, structures, and cultures of school settings. One necessary consideration within the school context is the school calendar and how to provide continuity of care during non-school times (e.g., after school, summer, vacations, professional development days). For example, some school TMH programs have found success in providing services during non-school hours by offering before- and after-school appointments, scheduling a TMH access 1 or 2 days per week during the summer, and offering occasional evening and weekend appointments. Collaboration with primary care physicians to provide coverage during non-school times is another option. Additionally, appointment times should be respectful of student class schedules, ideally prioritizing TMH services being conducted during non-“core” classes.
As with in-person school mental healthcare, school TMH requires an understanding of school culture, language, protocol, and policy. For example, understanding the special education process, including timelines, evaluation, and clinical service provision and how TMH services may and may not be included as part of the IEP process are all critical in providing TMH in schools. It will also be important for psychiatrists to be well versed in the existing systems of support in schools in order to properly refer and utilize available services and resources. In this regard, it may be helpful to use TMH equipment to allow psychiatrists to join IEP and other student support meetings.
On-site clinical support
In order to promote good patient care as well as efficient use of psychiatry time, it is recommended that school TMH be offered only when an on-site (in-school) mental health provider is available to coordinate and support service provision. The Maryland program examples described detail many of the protocol components established within this on-site/off-site collaborative process between a school clinician and a psychiatrist consulting via TMH. For example, the on-site clinician should be responsible for determining the appropriateness of a telepsychiatric consultation based on the scope of practice of the consulting psychiatrist. Within the Maryland model, for example, clinicians are trained on “appropriate topics of discussion with the psychiatrist,” which include: Medication issues/information (i.e., side effects, ineffectiveness, appropriate uses/dosages, health effects), when further evaluation (beyond the on-site clinician) is needed, if hospitalization would be warranted or beneficial, information on comorbid diagnoses, and/or psychoeducation on diagnoses or medications. The on-site clinician then provides several pieces of information to the psychiatrist prior to a session, including diagnostic information, prior and current service utilization, family dynamics (including external stressors on the family system), medical history, and reason for referral to TMH consultation. The on-site clinician is then responsible for scheduling the student/family during the psychiatrist's available time, and for ensuring that all participating individuals are ready for the appointment at the scheduled time. The presence of an on-site clinician also provides a mechanism for acute and ongoing support when issues of safety (e.g., suicidality) arise during a TMH session.
Conclusions
Schools offer a natural venue for children to receive mental healthcare, with evidence to suggest that school-based mental healthcare promotes greater follow through and access to care, particularly among underserved youth. While shortages of child psychiatry in underserved communities are expected to continue, rapid growth and improved and more affordable high-speed and sophisticated technology present greater opportunities for TMH to be realistically and effectively used in school and community settings (Katon et al. 2010; Yellowlees and Nafiz 2010; Grady et al. 2011a; Hilty et al. 2013). School TMH could become an essential service delivery model to address the growing mental health needs of students by providing access to an interdisciplinary, comprehensive system of support.
Existing data suggest that school TMH is well received by both providers and recipients of consultation and care, although further study would help advance understanding of the unique considerations for providing TMH in schools. A helpful initial step would be the development of a database of existing school TMH efforts in order to document current breadth and scope of services. Future research should encourage examination of policies, procedures, best practices and strategies that contribute to the greater efficiency and effectiveness in TMH, while still promoting school, youth and family engagement.
Clinical Significance
TMH has the potential to improve care while lowering costs for all parties; psychiatrists and families do not have to travel to appointments, parents/caregivers find it easier to make appointments at schools rather than traveling to another location, and students' needs are met at a location that is convenient to them (Alicata et al. 2006; Harper 2006). Although school TMH has some shortcomings from the provider's perspective, it continues to offer great potential to serve as a meaningful method to increase access to mental health care services for youth, especially in underserved areas (Grady et al. 2011b). That being said, it remains essential to consider the relative value of in-person care in comparison to TMH in schools, both with respect to the importance of exposing psychiatrists to the “real world” setting of schools, and related to opportunities to meaningfully engage students, families, and school personnel that may be more feasible with in-person service. Ultimately, we need to prioritize randomized, controlled studies comparing school-based in-person, TMH, and “hybrid” models to determine which demonstrates the greatest impact, and for which clients and presenting concerns.
Footnotes
Disclosures
No competing financial interests exist.