
Abstract
Objective:
The purpose of this study was to compare the short-term efficacy, tolerability, and 1-year adherence in Chinese children and adolescents with attention-deficit/hyperactivity disorder (ADHD) treated with either osmotic release oral system methylphenidate (OROS MPH) or atomoxetine (ATX).
Methods:
Children and adolescents meeting Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria for ADHD were randomly assigned to receive either OROS MPH (n = 119) or ATX (n = 118). Participants underwent a 1–4 week dose titration period to determine optimal dose, and then were maintained on that dose for 4 weeks (maintenance period). Assessment for efficacy was conducted every week over the titration period and at the end of the maintenance period. The primary efficacy measure was the investigator-rated total ADHD Rating Scale-IV (ADHD-RS-IV) score. Response was further classified as remission (ADHD-RS-IV [18 or 9 items] average score ≤1), robust improvement (ADHD-RS-IV ≥40% decrease in total score), or improvement (≥ 25% decrease in total score) at the end of maintenance period. Medication adherence (taking medication at least 5 days in 1 week) and reasons for nonadherence were evaluated every week over the titration period, at the end of maintenance period, and then at 3, 6, and 12 months.
Results:
At the end of maintenance period, both OROS MPH and ATX were associated with significant and similar reductions from baseline in ADHD symptoms. Percentages achieving remission, robust improvement, and improvement were comparable for OROS MPH and ATX treatment (35.3% vs. 37.1%, 45.4% vs. 44.8%, 65.5% vs. 66.4%). Medication use decreased over time for both treatments; however, at end of maintenance period, 3 month, 6 month, and 1 year follow-ups, subjects in the OROS MPH group were more likely to be compliant with treatment (74.8%, 50.4%, 38.7%, and 21.8% for OROS MPH vs. 52.5%, 33.9%, 12.7%, and 3.4% for ATX) ( p < 0.05). The most common reasons for nonadherence were adverse events and lack of efficacy.
Conclusions:
Both OROS MPH and ATX resulted in similar reductions in ADHD symptoms in Chinese children and adolescents with ADHD. Long-term adherence with medication was poor in general, although somewhat better with OROS MPH than with ATX.
Clinical Trial Registration:
Introduction
A
Several comparative efficacy studies conducted in American and European populations suggest that OROS MPH resulted in greater reduction in ADHD symptoms than ATX (Kemner et al. 2005; Newcorn et al. 2008; Yildiz et al. 2011). Both of Kemner et al. and Newcorn et al. reported that previous stimulant history influenced response in comparative studies. Kemner et al. found that MPH (n = 378) and ATX (n = 139) produced similar symptom rating scale score reductions at weeks 1 and 2 in the treatment-naive subgroup (n = 517) in the multicenter, randomized, open-label study in 1323 American children (Kemner et al. 2005). Subsequently, Newcorn et al. also conducted a large placebo-controlled, double-blind, randomized study for 6 weeks in America. It also found that the response rates for OROS MPH and ATX were not significantly different, but that they were superior to the rate for placebo in the treatment-naive subgroup at the end-point (Newcorn et al. 2008).
In contrast to in America or Europe where pharmacological treatment for ADHD has been well established, in China the majority of ADHD youth are treatment naive. This provides an opportunity for conducting head-to-head comparisons between these two medications, which are less likely to be influenced by previous treatment history. Moreover, there is a need to evaluate ADHD treatment in different ethnic groups and cultures, as genetic and biological differences and culture can affect the dosage requirement, treatment response, and side effect profiles of psychotropic medications. For example, Asians displayed significantly more side effects with antipsychotics than Caucasians during an initial fixed-dose phase, and required smaller doses during the clinically determined, variable-dose phase (Darmansjah and Muchtar 1992; Collazo et al. 1996; Lin 2001; Pi and Simpson 2005). However, little is known about how these factors influence dose, response, and side effect profiles for ADHD medications. Consequently, we seek to examine the efficacy and tolerability for two ADHD medications in Chinese children and adolescents with ADHD.
In previous studies, response was based on the change score or percentage reduction in scale scores from baseline (Kemner et al. 2005; Newcorn et al. 2008; Yildiz et al. 2011), but was not adjusted for differences in the initial severity of ADHD. For children with severe symptoms of ADHD, robust changes may represent statistically significant improvements, yet leave them quite impaired, whereas those with less severe symptoms may attain normalization after only modest percentage reductions in core symptoms of ADHD. Therefore, it is meaningful to subcategorize response as symptomatic remission, which should be minimal or asymptomatic, equivalent to a loss of diagnostic status and optimal functioning (Steele et al. 2006). We believe that this is the first study to compare the efficacy of OROS MPH and ATX in a Chinese population that emphasizes remission as the main outcome, in addition to changes in symptoms scores.
In addition to examining the short-term efficacy of OROS MPH and ATX, we also assess adherence, or the extent to which a patient acts in accordance with the prescribed treatment (Cramer et al. 2008). In ADHD, adherence is often poor (Charach et al. 2004); estimates of nonadherence to stimulant treatment range from 20% to 65% (Swanson 2003). Therefore, we will also assess and compare 1 year adherence and the reasons of nonadherence in a sample of Chinese children and adolescents with ADHD.
Methods
Patients
Participants included 262 children and adolescents, 6–16 years of age, recruited from the Child and Adolescent Psychiatric Outpatient Department of Beijing University Sixth Hospital. All met Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV-TR) (American Psychiatric Association 2000) criteria for ADHD (any subtype) as assessed by clinical history, and confirmed by a structured interview, the Clinical Diagnostic Interview Scale (CDIS) (Barkley 1998). The CDIS is based on the DSM-IV and assesses childhood behavioral and emotional disorders, such as ADHD, oppositional defiant disorder (ODD), conduct disorder (CD), affective disorders, tic disorder (TD). It was translated into Chinese by our group members (Yang et al. 2001, 2004). Similar to DSM-IV, the ADHD subscale recognizes three subtypes of ADHD: ADHD inattentive type (ADHD-I), ADHD hyperactive-impulsive type (ADHD-HI), and ADHD combined type (ADHD-C). Assessment of comorbidity was also based on the CDIS. Subjects were either treatment naive (n = 253) or had been untreated for at least 6 months (n = 9). For ethical reasons, subjects were excluded if they had a history of poor response with adequate treatment or intolerance to either MPH or ATX. Subjects who had medical contraindications to stimulants (i.e., narrow-angle glaucoma, cardiovascular disease) or who had seizure disorder or an abnormal electroencephalogram (EEG) associated with epilepsy, bipolar disorder, psychosis, anxiety disorder, depression disorder, TD, pervasive developmental disorder, or an intelligence quotient (IQ) <70 based on the Chinese-Wechsler Intelligence Scale for Children (C-WISC) (Gong and Cai 1993) were excluded from the study. In addition, subjects taking concomitant psychoactive medications including dietary supplements with central nervous system (CNS) activity in the past 30 days were also excluded. Subjects were not allowed to receive psychosocial treatment, such as behavior therapy, for ADHD symptoms during the short-term efficacy study, so that we could better evaluate the impact of the study medications. Moreover, behavioral treatments are not readily accessible in China.
The study was approved by the Beijing University Sixth Hospital Institutional Review Board. Parents signed the written informed consent form and the youth provided their assent.
Study design
This was a randomized, parallel-design, comparative study employing open-label titration of OROS MPH and ATX. After a pretreatment assessment and initial screening visit, patients were randomly assigned to receive one of the two medications. The randomization ratio was 1:1 for OROS MPH and ATX, respectively.
OROS MPH was initiated at 18 mg once daily (q.d.) in the morning, which could increase to 36 mg/day for week 2 and 54 mg/day for week 3. ATX was initiated at a dose of 0.5 mg/kg/day, which could increase to 0.8mg/kg/day for week 2, and 1.2mg/kg/day for weeks 3 and 4. If the efficacy was still dissatisfactory and the adverse events (AEs) were tolerable, 1.4 mg/kg/day (or 100 mg maximum) could be used in week 5. ATX was initially administered once daily (q.d.) in the morning, and could be switched to being administered twice daily (b.i.d.) when the AEs were intolerable. The maximum doses of two drugs were determined according to the drug instructions approved by China Food and Drug Administration (CFDA). 1
The flexible-dose titrating procedure was performed depending upon individual response and tolerability. The optimal dose for the subjects in this study was defined as the dose associated with maximum clinical improvement with tolerable AEs. If we found that the higher dose produced intolerable AEs or no more improvement in terms of the efficacy measures to be described, we would reduce the dose to the previous one that had been considered to be the optimal dose. Some patients achieved the optimal dose and finished titration after the first week, whereas others needed up to 4 weeks. Once an optimal dose was determined, it was maintained for 4 weeks, which were regarded as the maintenance period. Assessment for efficacy and AEs was conducted every week over the titration period, and at the end of maintenance period.
Subsequently, participants continued their regular outpatient treatment monthly, and clinicians could adjust doses as necessary in response to AEs and efficacy at each clinic visit. We tracked 1 year medication adherence. Adherence was defined as taking medication for ≥5 days per week throughout the follow-up period (Charach et al. 2004). In our study, all patients were asked to take OROS MPH or ATX continuously each day. Those taking medication <5 days per week, even during extended school breaks, would be considered nonadherent.
We collected the adherence information via face-to-face or telephone interviews with parents. If a subject was nonadherent, we asked about common reasons found by previous literature (Faraone et al. 2007; Gau et al. 2008; Chacko et al. 2010). Families were contacted every week over the titration period, at the end of the maintenance period, and at 3, 6, and 12 month follow-up. To confirm the parents' reports, we also examined the adherence information by checking outpatient medical records. If there was inconsistency between prescription dates and office visit dates, the former would prevail. It was difficult to use the pill-count method to assess medication adherence, as patients had to buy medication themselves with prescriptions over the whole course of study (e.g., both before and after maintenance period).
Measures
The primary efficacy measure was the investigator-rated ADHD Rating Scale-IV (ADHD-RS-IV), an 18 item scale corresponding to DSM-IV symptoms of ADHD (DuPaul et al. 1998). Ratings on the instrument were used to measure ADHD symptom severity during the past week. Item scores range from 0 (never or rarely) to 3 (very often). The secondary outcome measure was the investigator completed Clinical Global Impressions-ADHD-Severity scale (CGI-ADHD-S) (Guy 1976) to assess severity of impairment. The CGI-ADHD-S is a seven point scale (1 = not at all ill, 2 = minimally ill, to 7 = maximal impairment). The clinician scored the scales based on information obtained from the parent- and teacher-rated scales combining with the patients' face-to-face interview. (The CGI-ADHD-I subscale was not collected in our study.)
Response was subcategorized further as remission using three definitions: 1) An ADHD-RS-IV average score ≤1 (18 items for ADHD-combined subtype, 9 items for ADHD-inattentive or hyperactive/impulsive subtype) (Stein et al. 2003); 2) an ADHD-RS-IV each item score ≤1 (Steele et al. 2006); or 3) a CGI-ADHD-S scale score ≤2 (Kelsey et al. 2004). Robust improvement in ADHD symptoms was defined as ≥40% reduction and improvement was defined as ≥25% reduction from baseline in the total scores of investigator-rated ADHD-RS-IV at the end of maintenance period (DuPaul et al. 1998; Dickson et al. 2011).
During the initial visit, each participant received a physical examination, and parents reported the medical history. Vital signs (including blood pressure, heart rate, height, and weight) were recorded at each visit during the short-term efficacy study. Adverse events were assessed with the Barkley's Side Effects Rating Scale (SERS) (Barkley 1998). The SERS is a 17 item scale composed of a variety of CNS stimulant side effects. The severity of each symptom was rated by parents and confirmed by an investigator on a 10 point (0–9) scale ranging from absent to serious. Following the recommendations of Barkley et al. (1990), ratings of ≥7 were indicated a severe side effect (Stein et al. 2003).
Adherence to medication was defined as taking medication ≥5 days per week throughout the follow-up period (Charach et al. 2004). In other words, a patient with 1 week of taking medication <5 days would be labeled as nonadherent. We used such a stringent definition for the following reasons: First, in clinic, the prescribed medical treatment requires patients take medication no less than 5 days per week in order to cover the hours they were in school. Second, with this definition, we could focus on patients taking medication regularly, avoiding the potential effect of different medication-taking behavior on efficacy evaluation in the study. Reasons for nonadherence were subcategorized into the following 10 categories, including AEs, lack of efficacy, economic reasons, families' objection, patients' refusal to take medication, safety concerns, winter or summer vacation, condition improved, lost to follow-up, or other (Faraone et al. 2007; Gau et al. 2008; Chacko et al. 2010).
Statistics
The change scores from baseline of ADHD-RS-IV and CGI-ADHD-S in each visit were tested both within each medication group and between groups. Primary analyses were performed in the intent-to-treat (ITT) patients. In the ITT patients, data from dropout subjects were carried over by last observation carried forward (LOCF). The data with normal and non-normal distribution were analyzed by t test and nonparametric Wilcoxon signed rank test, respectively. Another response analysis was conducted examining the percentage of youth who achieved remission, robust improvement, and improvement at the end of the maintenance period. The rates of remission, robust improvement, and improvement were compared between groups by χ2 test. The abovementioned analyses were also performed in the per-protocol (PP) patients.
The incidence rates of AEs during the short-term efficacy period were compared between groups by χ2 test. The adherence rate (number of adherent patients/number of patients) and the nonadherence rates for different reasons (number of nonadherent patients for certain reason/number of patients) at each visit were also compared between groups by χ2 test.
All statistical tests were two tailed. An α level of 0.05 was used to assert statistical significance. Multiple-testing correction for p values was computed by step-down Bonferroni correction (Shaffer 1986). We calculated all above statistics using SPSS 16.0.
Results
Participants included 262 children and adolescents meeting inclusion criteria who were randomized to either OROS MPH or ATX treatment. Before beginning treatment, 21 patients withdrew consents (10 for OROS MPH and 11 for ATX) and 4 were lost to follow-up (1 for OROS MPH and 3 for ATX). Of the remaining 237 patients, 119 in OROS MPH group and 118 in ATX group received study medication and had at least one posttreatment measurement (ITT patients). Of the 237 subjects in ITT patients, only 142 (59.9%) completed the drug titration, maintenance, and all of the short-term efficacy assessments (PP patients). Of the PP patients, 85 were in OROS MPH group, and 57 in were in the ATX group. There were no significant pretreatment differences found between the OROS MPH and ATX treated groups in terms of sex, age, IQ, ADHD-RS-IV score, CGI-ADHD-S score, and comorbidity for either ITT patients or PP patients. However, the ratio of ADHD-combined subtype was higher for the OROS MPH group than that for the ATX group in the ITT patients (p = 0.02), but was not significantly different in the PP sample (p > 0.05) (Table 1). Before completing the maintenance period, 95 patients (40.1%) dropped out of the study. There were no significant differences in baseline characteristics between those patients who discontinued study participation and those who completed the maintenance period (PP patients) (p > 0.05).
p < 0.05
The data for the baseline characteristics of the PP patients were the same as in the former publication on executive function of this study.
Non-normal distribution.
OROS MPH, osmotic release oral system methylphenidate; ATX, atomoxetine; ITT, intent-to-treat; PP, per-protocol; IQ, intelligence quotient; ADHD, attention-deficit/hyperactivity disorder; ADHD-RS, ADHD Rating Scale; CGI-ADHD-S, Clinical Global Impression-ADHD-Severity; ODD, oppositional defiant disorder.
Efficacy and dose
For both ITT and PP patients, the ADHD-RS-IV total scores and CGI-ADHD-S scores were significantly lower at each post-treatment assessment (the ends of the week 1, titration period, and maintenance period) compared with pretreatment for both OROS MPH and ATX (p < 0.001). The difference between the two medication groups was not significant (Figs. 1, 2, 3, and 4, and Supplementary Table 1; Supplementary Data are available online at
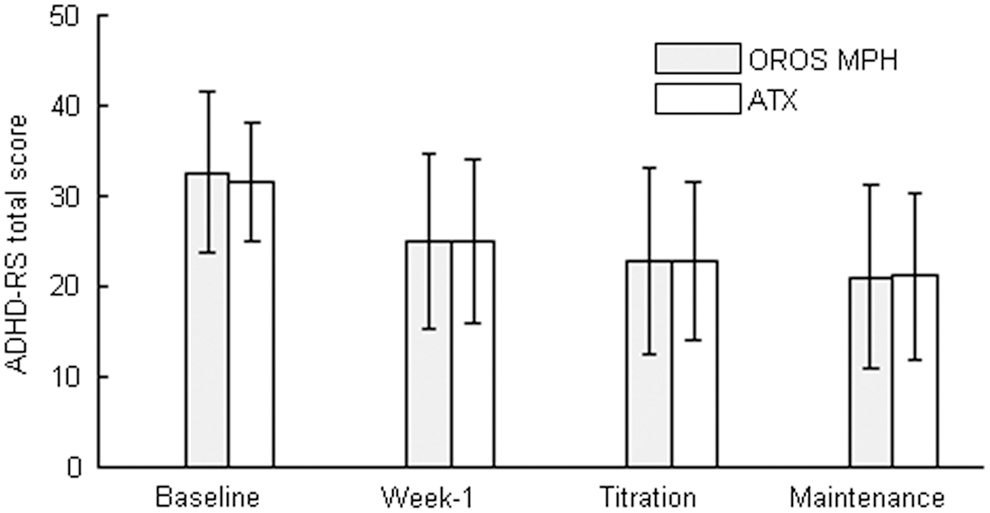
Comparison of Attention-Deficit/Hyperactivity Disorder Rating Scale (ADHD-RS) scores between the osmotic release oral system methylphenidate (OROS MPH) and atomoxetine (ATX) groups in intent-to-treat (ITT) patients.
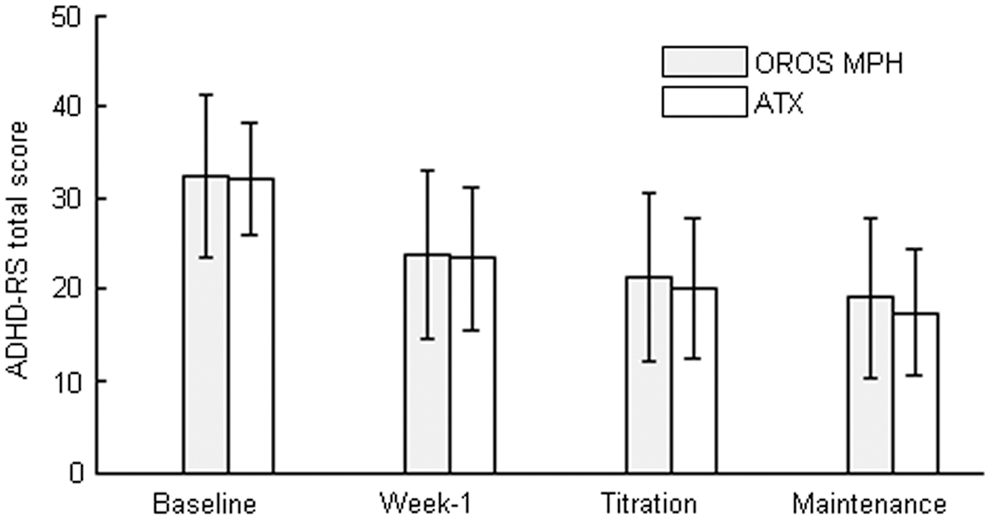
Comparison of Attention-Deficit/Hyperactivity Disorder Rating Scale (ADHD-RS) scores between the osmotic release oral system methylphenidate (OROS MPH) and atomoxetine (ATX) groups in per-protocol (PP) patients.
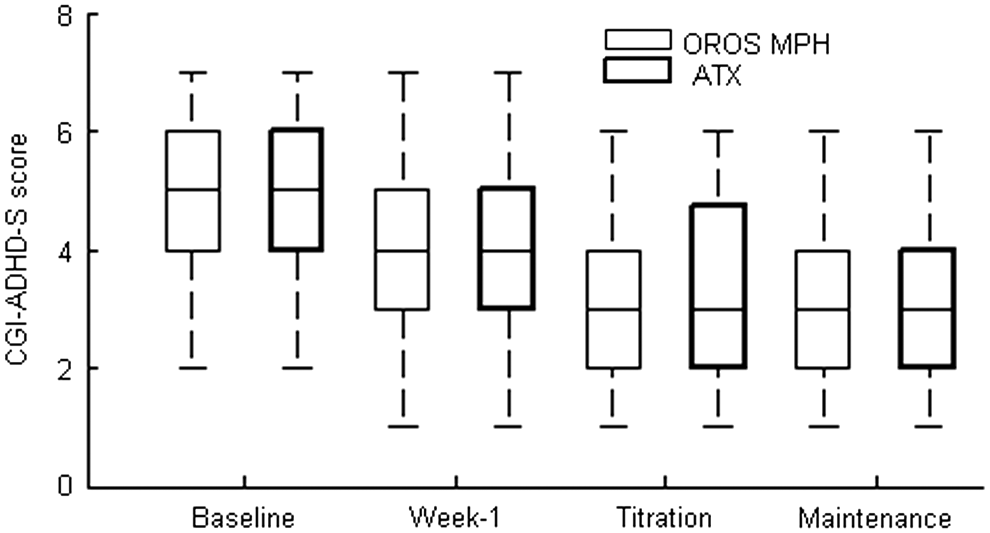
The comparison of Clinical Global Impressions-Attention-Deficit/Hyperactivity Disorder-Severity scale (CGI-ADHD-S) scores between osmotic release oral system methylphenidate (OROS MPH) and atomoxetine (ATX) groups in intent-to-treat (ITT) patients.
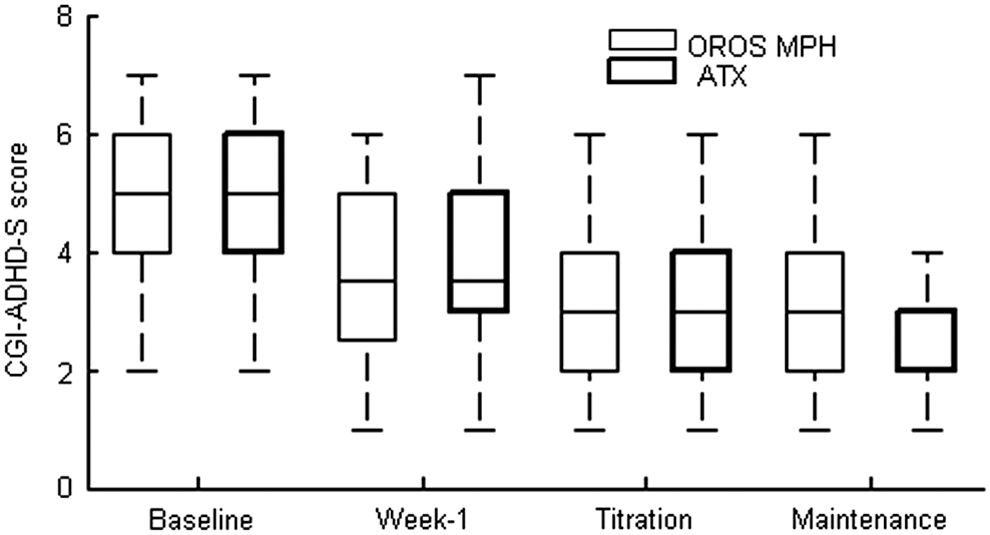
The comparison of Clinical Global Impressions-Attention-Deficit/Hyperactivity Disorder-Severity scale (CGI-ADHD-S) scores between osmotic release oral system methylphenidate (OROS MPH) and atomoxetine (ATX) groups in per-protocol (PP) patients.
At the end of maintenance period, there were no significant differences in the rates of remission, robust improvement, and improvement between subjects treated with OROS MPH and those treated with ATX (p > 0.05) (Table 2). Furthermore, there were no differences in drug effects when stratified by ADHD subtypes (p > 0.05).
OROS MPH, osmotic release oral system methylphenidate; ATX, atomoxetine; ITT, intent-to-treat; PP, per-protocol; ADHD-RS, Attention-Deficit/Hyperactivity Disorder Rating Scale; CGI-ADHD-S: Clinical Global Impressions-Attention-Deficit/Hyperactivity Disorder-Severity.
The most common titrated dose for OROS MPH was 18 mg/day (18 mg, 58 patients [68.2%]; 36 mg, 21 patients [24.7%]; 54 mg, 6 patients [7.1%]). For ATX, the mean dose was (36.70 ± 13.73) mg/day. Computed by kilograms of body weight, the mean doses were (0.69 ± 0.19) mg/kg/day for OROS MPH and (1.01 ± 0.23) mg/kg/day for ATX.
Tolerability
The two medications were associated with different AE profiles. AEs (Table 3), which occurred in at least 5% of patients receiving OROS MPH, were decreased appetite (84.2%), insomnia or trouble sleeping (44.7%), biting fingernails (35.1%), stomachaches (34.2%), and proneness to crying (33.3%). For ATX, the most common AEs included decreased appetite (80.4%), drowsiness (72.0%), dizziness (45.8%), stomachaches (43.9%), and headaches (43.0%). Those that had incidences markedly different between the OROS MPH and ATX groups included drowsiness (33.3% vs. 72.0%), dizziness (32.5% vs. 45.8%), proneness to crying (33.3% vs. 20.6%), anxiety (29.8% vs. 17.8%), and tics (6.1% vs. 0.0%) (p < 0.05). Adverse events rated as severe occurred in 14% of the OROS MPH group and 18.7% of the ATX group during a short-term efficacy trial (p > 0.05). The common severe AEs for OROS MPH were decreased appetite (13.2%), insomnia or trouble sleeping (3.5%), irritability (1.8%), drowsiness (1.8%), and proneness to crying (1.8%). For ATX, they were decreased appetite (16.8%), drowsiness (6.5%), dizziness (2.8%), and headaches (1.9%).
There were 16 patients who were impatient with the evaluation procedure without valid data on adverse events (5 patients for OROS MPH and 11for ATX).
Boldface denotes significant differences.
OROS MPH, osmotic release oral system methylphenidate; ATX, atomoxetine.
Adherence
Adherence rates to both medications were low (see Table 4). Subjects were adherent to OROS MPH treatment for a mean of 20.66 weeks (SD, 18.34), as compared with a mean of 10.92 weeks (SD, 11.52) for ATX during 1 year.
χ 2, p and p′ values were computed for adherence rates.
Multiple-testing correction for p values was computed by step-down Bonferroni correction.
Nine patients who were excluded from the per-protocol group because of invalid evaluation were adherent to medication. (Four patients for OROS MPH and five for ATX).
Boldface denotes significant differences.
OROS MPH, osmotic release oral system methylphenidate; ATX, atomoxetine.
At the end of titration period, 78.2% and 65.3% of patients were adherent to OROS MPH and ATX, respectively. This difference was marginally significant at this phase (p = 0.027, corrected p′ = 0.082). However, at the end of the maintenance period, and at 3 month, 6 month, and 1 year follow-ups, the difference was significant (p′ = 0.002, 0.040, < 0.001, < 0.001). Subjects receiving OROS MPH were more likely to be adherent to pharmacotherapy (74.8%, 50.4%, 38.7% vs. 21.8%) than children receiving ATX (52.5%, 33.9%, 12.7% vs. 3.4%).
Factors associated with nonadherence are reported in Table 5. For both medications, AEs and lack of efficacy were the primary reasons reported. At 1 year follow-up, 78.2% of the total patients were not compliant with OROS MPH treatment; in 31.9% and 20.2% of patients this was because of AEs and lack of efficacy, respectively. For those assigned to the ATX group, 96.6% of patients were not compliant; in 36.4% and 33.9% of patients this was because of AEs and lack of efficacy, respectively.
Boldface denotes significant differences.
OROS MPH, osmotic release oral system methylphenidate; ATX, atomoxetine.
AEs as a factor contributing to nonadherence were most prevalent early in the study and reduced gradually, whereas lack of efficacy increased over time. Because of intolerance to AEs, OROS MPH and ATX lost 27 (22.7%) and 35 (29.7%) compliant patients during the first 3 months, respectively (p > 0.05), whereas only 11 (9.2%) and 8 (6.7%) compliant patients were lost in the following 9 months, respectively (p > 0.05). In contrast, because of lack of efficacy, OROS MPH and ATX lost 9 (7.6%) and 19 (16.1%) compliant patients during the first 3 months, respectively (p < 0.05), and also lost 15 (12.6%) and 21 (17.8%) compliant patients in the following 9 months, respectively (p < 0.05).
Discussion
This study reported the results of a head-to-head, naturalistic comparison of the short-term efficacy, tolerability, and 1 year adherence of OROS MPH and ATX in a large sample of Chinese children and adolescents with ADHD. Similar to previous studies conducted in children of European and American ancestry (Wolraich et al. 2001; Kelsey et al. 2004; Kemner et al. 2005; Newcorn et al. 2008; Yildiz et al. 2011), both OROS MPH and ATX were associated with a rapid and clinically significant reduction in ADHD symptoms. However, we also had several findings that appear to be unique to Chinese children and adolescents with ADHD.
First, the average optimal dose of OROS MPH (or ATX) for the Chinese children and adolescents was relatively low compared with that in studies conducted in North America and Europe. For OROS MPH, the average optimal dose for Chinese children of 24.99 ± 11.14 mg/day was much lower compared with that in European or American samples; for example 39.9 ± 14 mg/day (Kemner et al. 2005) or 32.7 ± 12.1 mg/day (Newcorn et al. 2008). This difference cannot be explained primarily by differences in weight, as the mean weight-based dose of OROS MPH for Chinese children was 0.69 ± 0.19 mg/kg/day, which was also lower. Similarly, for ATX, the average optimal dose for Chinese children was 1.01 ± 0.23 mg/kg/day, which was also lower than the 1.3 ± 0.2 mg/kg/day reported by Michelson et al. (2002), the 1.25 ± 0.35 mg/kg/day reported by Kratochvil et al. (2007), or the 1.45 ± 0.32 mg/kg/day reported in another study (Newcorn et al. 2008). Nonetheless, the minimum daily dose for our participants was still within the suggested clinically effective dose range of MPH (Solanto 2000). Interestingly, our OROS MPH dose was similar to that reported by Lee et al. in a study of Korean children (Lee et al. 2007).
Our study used the recommend maximum doses approved by CFDA, which are 54 mg/day and 1.4 mg/kg/day (or 100 mg maximum) for OROS MPH and ATX, respectively. The maximum dose for OROS MPH was the same as in the Newcorn et al.'s study but was lower than the 72 mg/day used in Kemner et al.'s study, whereas the maximum dose for ATX was smaller than the 1.8 mg/kg/day used in Newcorn et al.'s study. However, the low optimal doses for the Chinese population were not the result of the relatively low maximum doses. In our study, the optimal doses of 93% patients with OROS MPH were <54 mg/day, demonstrating that few patients could be increased to a dose ≥54 mg/day. Here, both being optimized at lower doses and experiencing intolerable side effects at higher doses contributed to the relatively low optimal dose determined for most patients, although we do not have detailed data to quantify the effect of each cause. For ATX, no patients could be increased to above the maximum dose when the optimal dose had been achieved. In addition, no participant received behavioral services as well as school-based supports which may have led to lower doses during the short-term efficacy study.
It is unclear what factors contributed to the relatively low but effective doses utilized in our study. There are multiple determinants of dose, including both patient and provider characteristics, such as experience and training. One hypothesis is that, in contrast to the studies conducted in the United States, the biological homogeneity of the Chinese population may contribute to less variability in dose response. Perhaps Asians may be more sensitive to lower doses of OROS MPH and ATX, as has been suggested in previous studies on other psychotropic medications (Lin and Finder 1983; Collazo et al. 1996), perhaps because of genetic biological differences in pharmacokinetics or pharmacodynamics (Collazo et al. 1996), or other biological factors involved that are yet to be explored. For example, although cytochrome P450 2D6 (CYP2D6) is not involved in stimulant metabolism, it does moderate response to ATX. It is of note that differences in CYP2D6 allele frequencies have been demonstrated from studies across many countries. Although the CYP2D6 poor metabolizer phenotype is less frequent in Asians than in Western populations (e.g., ∼1% in Asians versus 5–10% in Caucasians), the prevalence of the CYP2D6*10 allele in Asians plays an important role in drug metabolism in Asian populations. CYP2D6*10 may be present in as much as 50% of Asians, but only in 5% of Caucasians, which might be responsible for the diminished enzyme activity and lower metabolic rates of Asians (Lin 2001; Cui et al. 2007).
Another possible factor contributing to relatively lower optimal doses is that nearly a half of participants in our study had ADHD-Inattentive subtype, which has fewer symptoms. It has been previously reported that attention symptoms respond to lower MPH doses than do hyperactive impulsive symptoms (Stein et al. 2003); therefore, this could be the result of the clinical composition of our sample. Although our study contained a sizably larger percentage of inattentive subtype participants (48.1%) than American studies (such as the 28.3% in Newcorn et al.'s study), the rate of ODD was comparable. Moreover, the percentage of inattentive subtype and the rate of comorbid ODD in our study were consistent with a previous study in China (Yang et al. 2004). A possible explanation is that Chinese parents tend to exhibit more inappropriate parenting practices, which is a risk factor of ADHD comorbid with ODD in Chinese population (Liu et al. 2007). However, the potential reasons still need to be further explored in a cross-cultural study.
Furthermore, there may also be cultural factors that contributed to the low but effective doses utilized in our study. For example, there is increased concern of potential AEs, which is not surprising given the recent awareness of ADHD and limited experience with ADHD medication in China. Moreover, there is a widely held cultural belief that many Western medicines are harmful to health, contributing to parental anxiety and sensitivity to AEs. Perhaps parents in China have a different view of the risk–benefit ratio, and prefer lower doses with fewer AEs, instead of higher doses with increased AEs and possible better efficacy. Certainly, further research is needed to clarify the factors contributing to the different doses between studies conducted in China and those conducted in the United States. It may be helpful to conduct fixed dose-response studies in addition to flexible dose titrations studies to evaluate drug effects more specifically.
Second, the short-term efficacy for OROS MPH and ATX were similar. During the titration and maintenance periods, no difference was found in ADHD-RS-IV total scores, and rates of remission, robust improvement, and improvement between the two medication groups. Our findings differ from those of previous comparative studies that found tha tOROS MPH provided better acute efficacy (Kemner et al. 2005; Newcorn et al. 2008; Yildiz et al. 2011).
A rapid reduction in symptoms was observed in the 1st week after treatment initiation with either OROS MPH or ATX, which was similar to many previous studies (Kelsey et al. 2004; Kemner et al. 2005; Wang et al. 2007; Newcorn et al. 2008). It is noteworthy that ATX was initiated at a dose of 0.5 mg/kg/day in the 1st week according to the drug instruction approved by CFDA in our study, which was lower than that in other studies. This fast response at lower dose may be caused by an expectancy effect, which was not controlled with a placebo group. It cannot be ruled out, however, that genetically determined biological factors also contributed to the fast response of ATX at a low dose, given the average lower optimal dose for Chinese children compared with their Western counterparts. Therefore, a large sample placebo-control study is needed.
It is unclear why the efficacy of two medications was similar in our study. Possibly, the low maintenance dose for Chinese patients (as explained) made efficacy difference less apparent in a short-term study. Second, previous studies have suggested that differential response was greater when there was a previous medication history, and that the response rates of the two drugs were more similar in naive subjects (Kemner et al. 2005; Newcorn et al. 2008). For example, Newcorn et al.'s study showed that the response rates (i.e., the robust improvement rates in our study) and the ADHD-RS-IV total scores were not significantly different between OROS MPH and ATX for a stimulant-naive subgroup (Newcorn et al. 2008). In our sample, the vast majority had not been previously treated.
Third, at 1 year follow-up, very few children were still compliant with either MPH or ATX. In our study, we found that only 21.8% and 3.4% patients were compliant at 1 year for OROS MPH and ATX treatments, respectively. The adherence rates of Chinese children were lower than those reported in other counties (Charach et al. 2004; Faraone et al. 2007, Wehmeier et al. 2015). For example, the study conducted with multiethnic populations found that 74.7% patients spent ≥75% of the studied days on medication (Faraone et al. 2007). The COMPLY observational study in Germany showed that 67.5% of patients in the ATX arm and 74.2% in psychostimulant arm were compliant with their study medication after 12 months (Wehmeier et al. 2015).
In contrast to in other studies, in our study, patients were not provided study medications (including during the short-term efficacy phase) and obtained the drug from their own physicians. Nonetheless, few patients stopped the treatment for economic reasons (Table 5). This implied that the poor adherence was the result of factors other than that of lacking incentives (e.g., not receiving medications at no cost). The main reasons for nonadherence reported by parents were similar for the two drugs in our study: Intolerance to AEs and lack of efficacy. We also observed that children receiving OROS MPH treatment had relatively better adherence than those receiving ATX, which is consistent with a German study (Wehmeier et al. 2015).
Comparing the rates of AEs (Table 3) with that reported in prior study, which also used the SERS (Stein et al. 2003), we found that, with the exception of decreased appetite, fingernail biting, euphoria/unusual happiness, and dizziness, the majority of side effects occurred with low/similar frequency in Chinese patients with OROS MPH treatment, compared with their Western counterparts. Cultural factors may contribute to the low tolerability of AEs; perhaps Chinese patients and families are less willing to tolerate mild to moderate AEs.
Global multicenter research is needed to determine the relative contributions of barriers to sustained treatment and to improve our understanding of the cultural and biological determinants of adherence. Future clinical trials should incorporate psychoeducation about the track record of safety, and medical monitoring during the trial, in order to reduce parental anxiety, and, possibly, improve adherence. More importantly, the clinician should prepare parents for potential AEs that are likely to occur during titration. Future placebo-controlled, double-blind studies are needed to confirm the results and to identify individual predictors for nonadherence and differential response, including genetic predictors, as we move toward personalized ADHD treatment. Moreover, further study is needed to examine to what extent the parental perceptions affect the efficacy of medications.
Limitations
This open-label design study did not include a placebo-control group, as we were primarily interested in comparative efficacy in this population, and several placebo controlled trials had already been conducted. Lack of a placebo arm may serve to inflate the efficacy for both medications, at least initially. Moreover, patients, parents, and investigators were aware which medication they were receiving. Therefore, there may have been potential for bias based on parents or investigators' expectancies. Raters were also not blind to group assignment. Given that ADHD treatment was novel in China and that most of the population was treatment naive, we presumed expectance effects or rater bias to be minimal. Although we did not collect the SERS in the unmedicated state, we examined the AEs via parents and children's reports combined with the clinical records.
Although our analysis on adherence indicates that efficacy difference might emerge over time, further research is needed to verify this indication through collecting and analyzing changes in mean dose over time and long-term efficacy data in even larger sample.
Conclusions
Both OROS MPH and ATX were effective in reducing ADHD symptoms in a large sample of Chinese children and adolescents with ADHD. Subjects were more somewhat likely to remain on OROS MPH, although the majority of participants were not compliant with ADHD treatments after 6 months.
Clinical Significance
There is a paucity of studies comparing the efficacy and adherence of OROS MPH and ATX for the treatment of Chinese patients with ADHD. Although several studies have compared the short-term efficacy of OROS MPH and ATX in America and Europe, little is known about cross- cultural differences in response to ADHD treatment. In the absence of such information, there is no objective basis for Chinese clinicians to know which drug to use with an individual patient. The study suggested that the short-term efficacy of OROS MPH and ATX was similar in China. The majority of Chinese children with ADHD are treatment naive, which perhaps this accounted for the similar efficacy when either medication is tried first.
The average optimal dose of OROS MPH (or ATX) was relatively low compared with that in studies conducted in North America. It is unclear if this is caused by biological or cultural factors. Perhaps Chinese parents have a different view of the risk–benefit ratio, and a prefer lower dose with fewer AEs.
Finally, adherence to either medicine was poor, as the majority of patients were not compliant with treatment within 6 months. Educating parents about the course of untreated ADHD and the track record of safety, as well as medical monitoring, may help reduce parental anxiety and improve adherence.
Footnotes
Acknowledgments
We thank the Clinical Epidemiology Research Centre of Beijing University Third Hospital for assistance in generating the randomization envelope. We also thank Drs. Lu Liu and Ning Ji for helping to collect data.
Disclosures
Dr. Yufeng Wang was supported by Xi'an Janssen's research grant. She has served on advisory boards of Xi'an Janssen Pharmaceutical Ltd and Eli Lilly Company. Dr. Li Yang received consulting fees from Eli Lilly and lecture fees from Xi'an Janssen Pharmaceutical Ltd. Dr. Stein is an advisor to Alcobra and Ironshores pharmaceuticals and received research support from Alcobra, Pfizer, and Shire. Drs. Qingjiu Cao and Yi Su have no financial relationships with any pharmaceutical company. Dr. Yi Su, as the first author, analyzed the data, and drafted and revised the manuscript. There was no honorarium, grant, or other form of payment given to anyone to produce the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.