
Abstract
Objective:
The efficacy of both methylphenidate and atomoxetine has been established in placebo-controlled trials. The present study aimed to directly compare the efficacy of methylphenidate and atomoxetine in improving symptoms among children with attention-deficit/hyperactivity disorder (ADHD).
Methods:
The study sample included 160 drug-naïve children and adolescents 7–16 years of age, with DSM-IV-defined ADHD, randomly assigned to osmotic-release oral system methylphenidate (OROS-methylphenidate) (n=80) and atomoxetine (n=80) in a 24 week, open-label, head-to-head clinical trial. The primary efficacy measure was the score of the ADHD Rating Scale-IV Parents Version: Investigator Administered and Scored (ADHD-RS-IV). The secondary efficacy measures included the Clinical Global Impressions–ADHD–Severity (CGI-ADHD-S) and Chinese Swanson, Nolan, and Pelham IV scale (SNAP-IV), based on the ratings of investigators, parents, teachers, and subjects.
Results:
At week 24, mean changes in ADHD-RS-IV Inattention scores were 13.58 points (Cohen's d, −3.08) for OROS-methylphenidate and 12.65 points (Cohen's d, −3.05) for atomoxetine; and mean changes in ADHD-RS-IV Hyperactivity-Impulsivity scores were 10.16 points (Cohen's d, −1.75) for OROS-methylphenidate and 10.68 points (Cohen's d, −1.87) for atomoxetine. In terms of parent-, teacher-, and self-ratings on behavioral symptoms, both of the two treatment groups significantly decreased on the SNAP-IV scores at the end-point, with effect sizes ranging from 0.9 to 0.96 on the Inattention subscale and from 0.61 to 0.8 on the Hyperactivity/Impulsivity subscale for OROS-methylphenidate; and from 0.51 to 0.88 on the Inattention subscale and from 0.29 to 0.57 on the Hyperactivity/Impulsivity subscale for atomoxetine. No statistically significant differences between treatment groups were observed on the outcome measures. Vomiting, somnolence, and dizziness were reported more often for atomoxetine than for OROS-methylphenidate, whereas insomnia was reported more often for OROS-methylphenidate than for atomoxetine.
Conclusions:
After 24 weeks of treatment, OROS-methylphenidate and atomoxetine had comparable efficacy in reducing core ADHD symptoms in drug-naïve children and adolescents with ADHD.
Introduction
A
Results from double-blinded, randomized, placebo-controlled trials show that the effect sizes for methylphenidate in patients with ADHD range from 0.5 to 1.0 (Wolraich et al. 2001; Wilens et al. 2006), whereas those for atomoxetine range from 0.6 to 1.3 (Svanborg et al. 2009; Martenyi et al. 2010). Given the remarkable variability in methods among ADHD treatment studies (Faraone et al. 2006), a direct comparative trial is required to identify differential medication efficacy.
Although results from several head-to-head trials of methylphenidate and atomoxetine show that responses to these two drugs are not different (Kratochvil et al. 2002; Sangal et al. 2006; Wang et al. 2007), others demonstrate statistically significant differences favoring methylphenidate (Kemner et al. 2005; Newcorn et al. 2008; Yildiz et al. 2011). Interpretation of those results is constrained by small sample size (Yildiz et al. 2011), short duration (Kemner et al. 2005), and the unequal cell sizes (Kratochvil et al. 2002; Kemner et al. 2005). Because of these contradicting results, further information indicating whether these two drugs have comparable efficacy in reducing core ADHD symptom in children is required.
The present study aimed to directly compare the treatment response in terms of ADHD symptoms of osmotic-release oral system (OROS)-methylphenidate and atomoxetine in drug-naïve children and adolescents with ADHD in a head-to-head, open-label, 24 week randomized clinical trial. The study also investigated the tolerability profiles of OROS-methylphenidate and atomoxetine.
Methods
Participants
Children and adolescents, 7–16 years old, were eligible to participate if they met the Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) diagnostic criteria for ADHD, as assessed by the investigator's clinical evaluation, and confirmed by the Chinese version of the Schedule for Affective Disorders and Schizophrenia for School-Age Children–Epidemiological Version (K-SADSE) (American Psychiatric Association 1994; Gau et al. 2005). To participate, patients had to have a Clinical Global Impressions-ADHD Severity Scale (CGI-ADHD-S) score of at least 4 (moderately ill or worse). Participants were excluded if they had a serious medical illness, such as a cardiovascular disease; had a Full-Scale Intelligence Quotient (IQ) score <80; had a history of bipolar I or II disorder, psychosis, any substance abuse, or pervasive developmental disorder; had depression or anxiety disorders based on the DSM-IV criteria at study entry; had a history of any seizure disorder or prior electroencephalogram abnormalities related to epilepsy; or had ever used any psychotropic medications before the study.
Study design and procedures
The Research Ethics Committee of National Taiwan University Hospital, Taiwan (IRB ID, 200812153M; ClinicalTrials.gov number, NCT00916786) approved this study prior to implementation. The potential subjects who met the recruitment criteria received a comprehensive explanation of the purpose and procedure of this study, as well as reassurance of confidentiality. Written informed consent was obtained from all the participants.
This was a 24 week open-label, head-to-head randomized clinical trial. Participants were assigned to either the OROS-methylphenidate or the atomoxetine group at a 1:1 ratio, which was determined by a computer-generated random sequence. They would receive seven assessments at baseline (visit 1), week 2 (visit 2), week 4 (visit 3), week 8 (visit 4), week 12 (visit 5), week 16 (visit 6), and week 24 (visit 7). Participants started to take medication at visit 1 with OROS-methylphenidate (an initial dosage of 18 mg per day, administered as a single morning dose) or atomoxetine (an initial dosage of 0.5 mg/kg per day, administered as once-daily dose). Drug dosage would be titrated at visits 2–7 (weeks 2–24) depending upon clinical response and adverse effects (maximum daily dosage of OROS-methylphenidate=54 mg daily; maximum daily dosage of atomoxetine=1.2 mg/kg daily). Data on body weight, body height, blood pressure, heart rate, ADHD Rating Scale-IV–Parent version: Investigator-Administered and Scored (ADHD-RS-IV), the CGI-ADHD-S, and parent-, teacher-, and self-reported Swanson, Nolan and Pelman-IV (SNAP-IV) for ADHD symptoms, were gathered at each visit, from visit 1 through visit 7 (weeks 0–24). The side effects of medications were investigated from visit 2 through 7 (weeks 2–24).
Primary efficacy measure (ADHD-RS-IV)
The primary efficacy measure was the ADHDRS-IV (DuPaul et al. 1998), a validated 18 item scale based on a semistructured interview with the patient's parent by the investigators to assess symptom severity over the past week. Each item, corresponding to one of the 18 DSM-IV diagnostic criteria, is rated on a four point scale (0=never or rarely, 1=sometimes, 2=often, 3=very often). This scale has been shown to be a reliable and valid instrument to assess the severity of ADHD symptoms in clinical research in Western countries (Faries et al. 2001) and also in Taiwan (Gau et al. 2007).
Secondary efficacy measures
The secondary outcome measures included the CGI-ADHD-S and the Chinese SNAP-IV (Parent Form, Teacher Form, and Self-Report Form).
CGI-ADHD-S
The CGI-ADHD-S, rated by the investigators, is a single-item rating of the clinician's assessment of the global severity of ADHD symptoms in relation to the clinician's total experience with other ADHD patients. Severity is rated on a seven point scale (from 1=normal, not at all ill, to 7=among the most extremely ill). The Chinese CGI-ADHD-S has been used widely in treatment studies on ADHD in Taiwan (Gau et al. 2007; Gau and Shang 2010).
SNAP-IV
The SNAP-IV, a 26 item scale, consists of Inattention (Items 1–9) and Hyperactivity/Impulsivity (Items 10–18), and Oppositionality (Items 19–26), corresponding to the core symptoms of DSM-IV ADHD and oppositional defiant disorder (ODD), respectively (Swanson et al. 2001). The 26 items of the SNAP-IV are rated on a four point Likert scale, with scores of 0–3 representing “not at all,” “just a little,” “quite a bit,” and “very much,” respectively. The Chinese SNAP-IV-Parent (Gau et al. 2008) and -Teacher (Gau et al. 2009) Forms have good validity and reliability, and have been widely used in clinical trials to assess the efficacy of OROS-methylphenidate (Chou et al. 2009) and atomoxetine (Gau and Shang 2010) in children with ADHD.
Safety measures
Safety measures, including decreased appetite, vomiting, insomnia, somnolence, dizziness, stomachaches, headaches, palpitations, and dry mouth, were assessed at each visit by open-ended questions during a clinical interview first, followed by a structured interview based on a standard questionnaire listing all the potential adverse effects by the investigators. Vital signs and body weight were regularly monitored at each visit.
Adherence
Subjective and objective assessments were used to determine whether the participants were adherent to OROS-methylphenidate and atomoxetine. The subjective assessment was based on retrospective feedback from the parents and participants themselves. The objective assessment of the daily occurrence and frequency of missed doses was based on pill count by research assistants and a standard interview conducted by the investigators. If the data based on the two methods were not consistent with each other, the investigators would interview the parents and participants again and discuss the difference between parent-reports or self-reports and pill count, and then would determine the days of taking medication. We compared adherence between the two treatment groups based on average days of taking medication per week.
Data analysis
SAS version 9.2 was used to conduct data analysis. The α value was preselected at the level of p<0.05. The intent-to-treat principle was used in the statistical analysis. Mean scores and SD were presented for continuous variables, and number and percentage were presented for categorical variables in the demographic and baseline assessments. One way repeated-measures analysis of variance (ANOVA) using the mixed procedure was used to determine differences in behavioral symptoms. Hierarchical linear mixed-effect models were employed to address the lack of statistical independence of repeated measurements of the same participants over time. In particular, both intercepts and slope (time) effects in the linear mixed model with time-dependent variables were treated as random effects, to account for variations among subjects in baseline values, and slopes for individual trajectories of symptom changes over seven assessments, in addition to the main treatment and fixed-time effect of the two treatment groups. In addition, Cohen's d was used to compute the effect sizes for the comparisons of the scores of the ADHD-RS-IV, CGI-ADHD-S, and SNAP-IV-Parent, Teacher, and Self Forms between the two treatment groups at each visit.
Results
Sample description and medication
Of the 174 patients screened, 160 entered our study and were randomly assigned to the OROS-methylphenidate (n=80) (age, 9.64±2.42; 70 males, 87.5%) and atomoxetine groups (n=80) (age, 9.90±2.78; 70 males, 87.5%). Patient characteristics and baseline symptom measures were not significantly different between treatment groups (Table 1).
ADHD, attention-deficit/hyperactivity disorder; ADHD-RS-IV, ADHD Rating Scale-IV–Parent version: Investigator-Administered and Scored; CGI-ADHD-S, Clinical Global Impressions–ADHD–Severity; SNAP-IV, Swanson, Nolan, and Pelham IV scale.
The overall study completion rates were 82.5% (66/80) for OROS-methylphenidate and 80% (64/80) for atomoxetine at week 24 (visit 7) (Fig. 1). There was no obvious significant difference in follow-up compliance between the two groups. There was no significant baseline difference between ADHD participants who dropped out and those who completed the trial with regard to demographics and clinical severity for the OROS-methylphenidate and atomoxetine groups, or for the whole sample. In the OROS-methylphenidate group, participants dropped out of the study because of loss of contact (n=6), treatment-emergent adverse events (n=3, including decreased appetite [2] and insomnia [1]), and for personal reasons (n=5). In the atomoxetine group, participants dropped out of the study because of loss of contact (n=9), treatment-emergent adverse events (n=3, including decreased appetite [1] and somnolence [2]), and for personal reasons (n=4).
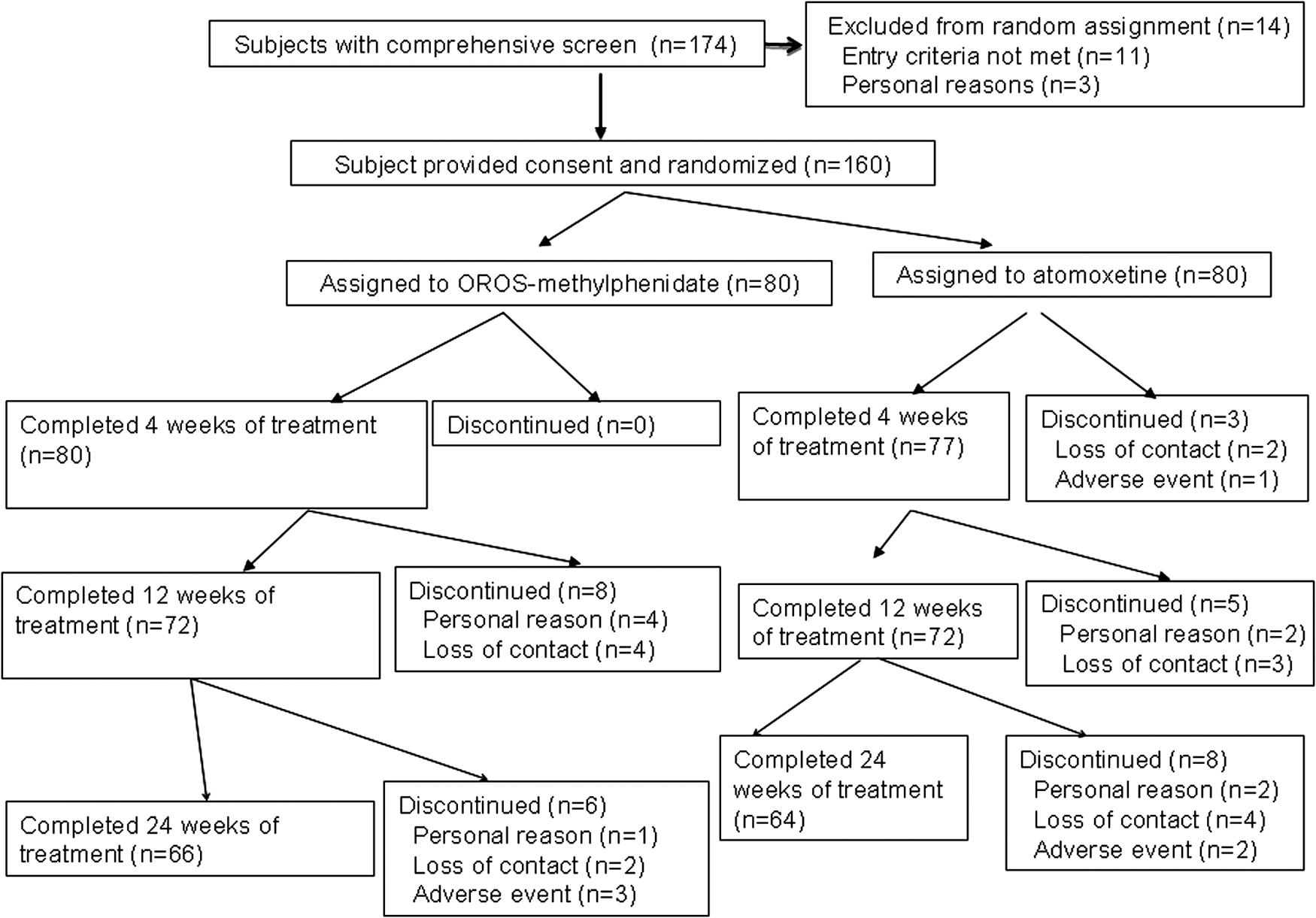
Flow diagram of the randomization procedure and outcome of all recruited subjects.
The mean final administered dose for OROS-methylphenidate was 27.83 (SD=12.44) mg/day or 0.82 (SD=0.34) mg/kg per day. The mean final administered dose for atomoxetine was 31.74 (SD=10.34) mg/day or 0.98 (SD=0.28) mg/kg per day. There was no significant difference in drug adherence between the two treatment groups.
Efficacy of ADHD-RS-IV
Our results showed that, compared with baseline scores, both treatment groups showed statistically significant reductions in ADHD symptoms at each time point (Table 2). At week 8, mean changes from baseline in ADHD-RS-IV Inattention scores were 13.25 points (Cohen's d, −3.13) for OROS-methylphenidate and 12.26 points (Cohen's d, −3.06) for atomoxetine; and mean changes from baseline in ADHD-RS-IV Hyperactivity-Impulsivity scores were 9.38 points (Cohen's d, −1.55) for OROS-methylphenidate and 9.74 points (Cohen's d, −1.77) for atomoxetine (Table 2). At week 24, mean changes from baseline in ADHD-RS-IV Inattention scores were 13.58 points (Cohen's d, −3.08) for OROS-methylphenidate and 12.65 points (Cohen's d, −3.05) for atomoxetine; and mean changes from baseline in ADHD-RS-IV Hyperactivity-Impulsivity scores were 10.16 points (Cohen's d, −1.75) for OROS-methylphenidate and 10.68 points (Cohen's d, −1.87) for atomoxetine (Table 2).
ADHD, attention deficit hyperactivity disorder; ADHDRS-IV, ADHD Rating Scale-IV–Parent version: Investigator-Administered and Scored; CGI-ADHD-S, Clinical Global Impressions–ADHD–Severity; OROS, osmotic-release oral system; SNAP-IV, Swanson, Nolan, and Pelham IV scale.
The analysis of mean changes in ADHD-RS-IV from baseline to week 8 and from baseline to the end-point showed no significant differences between the two treatment groups (Table 2, Fig. 2A for inattention, and Fig. 2 B for hyperactivity/impulsivity). In addition, there were no significant differences in ADHD symptoms at each time point between the two treatment groups, except that the ADHD-RS-IV Inattention score was significantly lower for the OROS-methylphenidate group than for the atomoxetine group at week 2 (visit 2) (Cohen's d=0.46; p=0.004, Fig. 2A). However, analysis of slope differences revealed no significant group difference in the slope of the mean score reduction for the ADHD-RS-IV Inattention (F 1,708=0.08, p=0.78) and Hyperactivity-Impulsivity (F 1,708=1.25, p=0.26) subscales.

Efficacy of CGI-ADHD-S and SNAP-IV
Beginning at week 2 after initiation of treatment and continuing to the end-point, both treatment groups showed significant decreases in global ADHD symptoms severity based on the CGI-ADHD-S. At week 8, mean changes from baseline in CGI-ADHD-S scores were 2.45 points (Cohen's d, −3.4) for the OROS-methylphenidate group and 2.34 points (Cohen's d, −3.46) for the atomoxetine group. At the end-point, mean changes from baseline in CGI-ADHD-S scores were 2.57 points (Cohen's d, −3.2) for the OROS-methylphenidate group and 2.4 points (Cohen's d, −3.15) for the atomoxetine group. No significant group differences in mean reductions in the CGI-ADHD-S from baseline to week 8 (p=0.465) and to the end-point (p=0.308) were found between the two treatment groups (Table 2).
In terms of parent-, teacher-, and self-ratings on behavioral symptoms, both treatment groups had significantly decreased scores on the SNAP-IV from baseline to the end-point, with treatment effect sizes ranging from 0.9 to 0.96 in the Inattention subscale and from 0.61 to 0.8 on the Hyperactivity/Impulsivity subscale for the OROS-methylphenidate group; and from 0.51 to 0.88 on the Inattention subscale and from 0.29 to 0.57 on the Hyperactivity/Impulsivity subscale for the atomoxetine group. No significant group differences in the mean reductions of the SNAP-IV total and subscores from baseline to week 8 and to the end-point were found between the two treatment groups (Table 2).
Safety
Treatment-emergent adverse events reported in >1% of subjects in either treatment group were summarized in Table 3. Among these adverse events, vomiting (p=0.017), somnolence (p<0.001), and dizziness (p=0.009) were reported more often for atomoxetine, whereas insomnia (p=0.035) was reported more often for OROS-methylphenidate (Table 3). No drug-related severe adverse event was reported during our study period. Results also showed no treatment group differences in other safety assessments, such as vital signs and body weight change.
OROS, osmotic-release oral system.
Discussion
To our best knowledge, this is the first large head-to-head, randomized, long-term (24-week) study to prospectively compare response to OROS-methylphenidate and atomoxetine in drug-naïve children and adolescents with ADHD. Our findings show that both OROS-methylphenidate and atomoxetine treatments are associated with clinically meaningful improvements in ADHD symptoms, including inattention and hyperactivity/impulsivity. Symptom severity decreased to “mildly-to-moderately ill” for both treatment groups, suggesting that both OROS-methylphenidate and atomoxetine are efficacious in reducing the severity of ADHD symptoms. In addition, no significant differences were noted between the two treatment groups with respect to the ratings of investigators, parents, teachers, and subjects. Our findings provide further comparative information for the similar efficacy of OROS-methylphenidate and atomoxetine in reducing ADHD symptoms in children and adolescents (Kratochvil et al. 2002; Sangal et al. 2006).
Although some of earlier comparator trials show that methylphenidate is superior to atomoxetine in reducing ADHD symptoms (Kemner et al. 2005), several design features may influence the observed results. First, subjects who previously had either poor response or intolerable adverse events in an adequate trial of methylphenidate were excluded (Kemner et al. 2005). Such study design could create a critical bias in favor of methylphenidate by excluding those with increased risk for poor response or tolerability with methylphenidate. Consistent with our findings, effect sizes for atomoxetine in treatment-naïve cohorts are similar to those for methylphenidate (Bushe and Savill 2014), implying the clinical value of using treatment-naïve populations as a baseline comparator in ADHD (Montoya et al. 2009; Svanborg et al. 2009). Second, the short duration of treatment is inadequate for accurate assessment of response to atomoxetine because the effectiveness of OROS-methylphenidate may increase at a faster rate than that of atomoxetine during the first few weeks after treatment initiation (Kemner et al. 2005). Reductions in core ADHD symptoms are gradual with atomoxetine and may extend beyond 12 weeks (Dickson et al. 2011). In our present study, although improvements on the primary efficacy measure were observed in both treatment groups as early as 2 weeks after randomization, the ADHD-RS-IV Inattention score of the OROS-methylphenidate group was significantly lower than that of the atomoxetine group (Cohen's d, 0.46; p=0.004) at week 2 (visit 2). However, the responses to these two medications were not significantly different from week 4 through week 24 (visits 3–7). Our findings demonstrate that long-term studies are needed to evaluate changes in the relative efficacy of OROS-methylphenidate and atomoxetine.
Given no direct reports from teachers in most of previous studies (Kemner et al. 2005; Newcorn et al. 2008), our present study is one of the few head-to-head trials employing teacher ratings to assess ADHD symptom severity (Yildiz et al. 2011). Several studies have demonstrated that teacher ratings are important not only when the diagnosis of ADHD is being established (Wolraich et al. 2004), but also during a year-long medication trial (Lavigne et al. 2012). Failure to obtain teacher ratings is one reason why medication management of ADHD is thought to be suboptimal (Miller 1999).
A meta-analysis finds that the standardized mean difference in ADHD scores between atomoxetine and methylphenidate using parent ratings is relatively small, and that the difference is much higher if studies use teacher ratings, suggesting that the advantage of methylphenidate over atomoxetine appears larger in school than at home (Hanwella et al. 2011). However, only one study with a small sample size (n=30) included in that meta-analysis used teacher ratings (Yildiz et al. 2011). Our present study with a larger sample size shows that the magnitude of symptom reduction based on the teacher ratings is similar to that based on the parent ratings, implying the comparable effectiveness of OROS-methylphenidate and atomoxetine in improving ADHD symptoms across situations.
Changes in self-rated SNAP-IV scores also show significant improvement over baseline for both drugs. Previous studies demonstrate that children are valuable informants about their own behavior (Sturgess et al. 2002; Klimkeit et al. 2006). The improvement in subjects' self-reported measures in the present study suggests that self-reports may be useful for assessing treatment outcomes for ADHD. Further research is needed to investigate the basis on which children and adolescents with ADHD make their self-ratings: Whether they are reporting behaviors that they have heard others feed back to them or whether they themselves have observed these behaviors in themselves.
A recent review of published prospective clinical trials shows that most adverse events are mild for methylphenidate and atomoxetine used for ADHD in children and adolescents (Clavenna and Bonati 2014). In our present study, both OROS-methylphenidate and atomoxetine were safe and well tolerated, with only modest differences in tolerability between the two drugs. Neither drug was associated with treatment-emergent serious events, although concerns about the potential for increased serious outcomes (Vitiello 2008) related to medications used to treat ADHD have been raised. The number of patients recruited in the present study was based primarily on detecting differences in efficacy, not safety; therefore, it is possible that infrequently occurring events could have been missed.
Limitations
Several limitations of this study should be considered when interpreting our findings. First, OROS-methylphenidate is a controlled drug in Taiwan, which prevents us from conducting a double-blinded, placebo-controlled trial as an investigator-initiated clinical trial. Because there is no assignment to placebo, we cannot determine whether patients assigned to placebo would also show an improvement over the 24 week duration of treatment. Second, the sample size may not have enough power to detect the differences in efficacy between the two drugs. Third, open-label studies are subject to potential expectation bias. However, our data are consistent with rating score improvements reported in placebo-controlled studies with OROS-methylphenidate (Wolraich et al. 2001) and atomoxetine (Gau et al. 2007). In addition, the bias derived by an open trial design has been minimized by our approach strategies as follows: Study subjects, their parents, and teachers did not know the hypothesis of this study, and parents were instructed regarding symptoms and asked to rate their children's symptoms objectively without taking into account what treatment their children received. In Taiwan, neither a school nurse nor a teacher distributed medication to students; therefore, the teachers would not know which medication their students took. Fourth, the stimulant comparator in the present study was OROS-methylphenidate; therefore, our findings may not generalize to other formulations of methylphenidate or to amphetamine. Fifth, allowing investigators to adjust doses without using a systematic titration schedule could have led to underdosing in one group or the other; however, doses in the current study are consistent with those in the package information. Sixth, generalizability of this present study is questionable because of participants being from one medical center in Taipei, and because of the small number of females. Lastly, the present study excluded patients with other psychiatric disorders, such as depression or anxiety. Further studies to compare the treatment response of OROS-methylphenidate and atomoxetine in patients with the comorbid conditions of ADHD are needed.
Conclusions
The present study suggests that both OROS-methylphenidate and atomoxetine are well tolerated and effective in the improvement of ADHD core symptoms in drug-naïve children and adolescents after 24 weeks of chronic treatment. These results are consistent across settings (home and school), raters (investigators, parents, teachers, and subjects) and measures (ADHD-RS-IV, CGI, and SNAP-IV).
Clinical Significance
Our findings based on drug-naïve children and adolescents with ADHD challenge previously held beliefs that methylphenidate has a significantly greater effect size than atomoxetine, and suggest that pharmacological treatment with either OROS-methylphenidate or atomoxetine is promisingly effective in drug-naïve children and adolescents with ADHD.
Footnotes
Acknowledgments
The authors thank to Ming-Fang Chen for assistance in data analysis, and for making the tables, and also thank all the participants and their parents for their contributions.
Disclosures
C.Y.S., S.S.G., Y.L.P., H.Y.L., and L.W.H. were investigators. Data were analyzed by S.S.G. The manuscript was drafted by C.Y.S. and critically reviewed by S.S.G. All the authors approved the final version of the manuscript for submission. S.S.G., C.Y.S., and H.Y.L. were on the speakers' bureau for Janssen-Cilag and Eli Lilly & Co., Taiwan. Y.L.P. and L.W.H. have no conflict of interest to be disclosed.