
Abstract
Objective:
The goal of the University of Hawaii (UH) child and adolescent psychiatry telemental health (TMH) program is to train child and adolescent psychiatry fellows to provide behavioral health services for the children of Hawaii and the Pacific Islands in the cultural context of their rural communities using interactive videoteleconferencing (IVTC). The training experience balances learning objectives with community service. Learning objectives include: Understanding mental health disparities in rural communities, leveraging community resources in ongoing treatment, providing culturally effective care, and improving health care access and delivery through TMH service research and evaluation.
Methods:
We describe the UH experience. Several UH faculty are experienced with IVTC technology. They are triple-board trained, are recognized for their research in program evaluation and mental health disparities, and are committed to serving Hawaii's rural communities. We demonstrate the role of TMH in linking children and their families living in rural communities with multiple mental health treatment providers. The service-learning curriculum and a unique collaboration with Mayo Clinic provide the opportunity to examine the role of TMH in global service, and training, education, and research.
Results:
TMH provides direct services to patients and consultation on Hawaii Island and Maui County. The collaboration with the Mayo Clinic brings further consultation in complex diagnostics, pharmacogenomics, and cross-cultural psychiatry. A curriculum provides trainees experience with IVTC with the goal of potential recruitment to underserved rural communities. The TMH program at UH is unique in its team building and workforce development by joining multiple entities through IVTC and translating expertise from the Mayo Clinic to rural communities, and strengthening collaboration with local child and adolescent psychiatrists, and primary care and other mental health providers.
Conclusions:
The UH psychiatry program is a model program to develop an expert mental health workforce in cultural context for children living in rural communities.
Introduction
T
Clearly, there is a critical need to develop a workforce of child and adolescent mental health and primary care providers who are committed to serving Hawaii's children, particularly in rural and underserved areas, and who are proficient with the use of creative technologies in meeting these healthcare needs (Helm et al. 2010; Chung-Do et al. 2012). To meet this need, we developed a telemental health (TMH) training curriculum for child and adolescent psychiatry (CAP) fellows and a collaboration with the Mayo Clinic that examines the role of TMH in global service and workforce development, education, training, and cross-cultural psychiatry.
Methods for Development of a TMH Service
The TMH program at the University of Hawaii (UH) has five core components: 1) A TMH service-learning curriculum, 2) cultural context: the Hawaii experience, 3) a collaboration for workforce development, 4) a primary care initiative, and 5) technology.
Development of the TMH service-learning curriculum
In 2008, a collaboration was formed between UH at Manoa, Department of Psychiatry (DOP) and the Department of Health, Child and Adolescent Mental Health Division (CAMHD) with the goal of developing a TMH training curriculum for CAP fellows. The curriculum adheres closely to the clinical guidelines and practice parameters described by the American Academy of Child and Adolescent Psychiatry (Myers et al. 2008) and the American Telemedicine Association (Yellowlees et al. 2010).
The service-learning curriculum integrates the Accreditation Council for Graduate Medical Education (ACGME) clinical competencies as described in the Psychiatry Milestone Project to train residents to become competent psychiatrists and educate medical students to the discipline (Accreditation Council for Graduate Medical Education 2013). The residents achieve clinical skills and training goals by participating in clinical services that are part of the Hawaii community-based system of care administered by CAMHD (Chorpita and Donkervoet 2005; Hodges et al. 2006; Daleiden et al. 2006). The TMH training objectives include understanding mental health disparities in rural Hawaii communities, creatively leveraging community resources in ongoing treatment, providing culturally effective care, achieving proficiency with the technology to resolve issues of distance and time in serving rural areas, and improving health care access and delivery through TMH service research and evaluation.
Because of the critical need for child and adolescent psychiatric services to rural communities, the TMH clinics were initially developed at the CAMHD Family Guidance Centers (FGC) on Hawaii Island, in the communities of Waimea, Kona and Hilo, and Maui County (includes the islands of Maui, Molokai and Lanai). As the clinical needs continue to grow, the TMH program will expand to the communities of Leeward Oahu and Kauai. All these communities are federally designated as Health Professional Shortage Areas and Medically Underserved Populations/Areas (Hawaii Primary Care Association 2006). Partnerships were developed with the FGC clinical directors, who also serve as DOP clinical faculty and regularly participate in the fellowship curriculum didactics and the on-site clinical supervision of the trainees. The DOP and CAMHD clinical leadership and support staff developed the TMH clinical protocols that include staff training, scheduling, billing, communication and maintaining interactive videoteleconferencing (IVTC) connection integrity, pharmacy support, electronic health record and clinical documentation, and emergency and after-hour coverage, and that meet the Health Insurance Portability and Accountability Act (HIPAA) requirements (Myers et al. 2008; Yellowlees et al. 2010).
Youth are often referred for support for emotional and behavioral development (SEBD) services with CAMHD from a number of community sources, including acute hospitalization, the Departments of Education and Human Services, Hawaii State Judiciary (Family and Drug Courts), juvenile justice, primary care, and directly by the family. The youth and their families participate in a series of mental health evaluations, and the CAMHD clinical director determines the range of comprehensive services available to the family and whether the TMH program would be helpful in achieving the treatment goals. Once the services begin, the CAMHD clinical director and staff coordinate all mental health and educational services provided by multiple community-based contracting agencies and the Department of Education (DOE). We are fortunate that an increasing number of community- and hospital-based programs have IVTC capacity and can link the youth with their family during periods of residential treatment or incarceration. Figure 1 shows the service array available through CAMHD (State of Hawaii, Department of Health 2012). IVTC technology is required, at a minimum, to connect at any point in the range of services and to link the youth, family, and mental health providers with single- and multiple-point connections that meet clinical standards and HIPAA requirements. Multiple-point IVTC connections are often required to connect with youth in a hospital- or community-based residential treatment program on Oahu, their family, and treatment team on Hawaii Island or Molokai and with the DOP TMH team on Oahu.
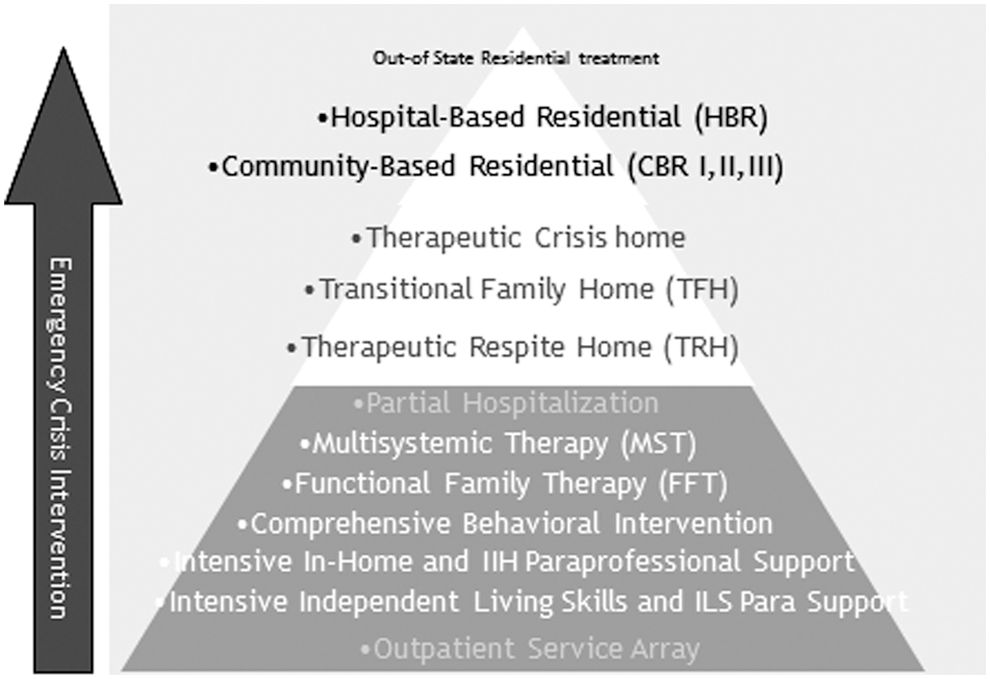
Services available through Child and Adolescent Mental Health Division (CAMHD): Evidenced-based services are organized as outpatient in-home and out-of-home, ranging from less to more intensive levels of care (State of Hawaii, Department of Health 2012).
Cultural context: The Hawaii experience
Several authors have recommended approaches to integrate culturally appropriate care into TMH practice (Shore et al. 2006; Savin et al. 2011; Brooks et al. 2013; Yellowlees et al. 2013). We discuss these recommendations from the perspective of a collaborative academic and state TMH program committed to building a team of expert child and adolescent psychiatrists that provide culturally appropriate care to youth and their families in their own community.
In 1993, the state was involved in a class action lawsuit concerning inadequate educational and related mental health services provided to children with disabilities. In 1994, the lawsuit was settled resulting in a system of care reform with the agreement that children identified as needing mental health services in order to benefit from their public education would receive evaluation and intervention within an evidenced-based system of care (Chorpita and Donkervoet 2005; Daleiden et al. 2006; Hodges et al. 2006; see Fig. 1). Prior to the lawsuit, rural communities experienced multiple practitioners, who often were unfamiliar with the local community and culture and provided fragmented and time-limited care that continued until funding resources were no longer available or when debt obligations were fulfilled. The practitioners often left the community or abruptly stopped providing services. It was common that families were without follow-up care or realistic strategies for the appropriate transition of care. The communities often experienced protracted periods of time when practitioners were not available and families were without psychiatric care. Consequently, families were hesitant to engage with any services or care, when their sustainability was uncertain.
In response to the class action lawsuit, the DOP and CAMHD developed a collaborative rural community training rotation for CAP fellows in 1997. An objective for the training experience was to appreciate the role of culture in the psychiatric formulation and in the provision of timely evidence-based mental health services for Hawaii's children living in rural and ethnoculturally diverse communities (Andrade et al. 2006; Accreditation Council for Graduate Medical Education 2013; Guerrero et al. 2014). Therefore, critical lessons learned because of the class action lawsuit were the importance of building the future workforce of child and adolescent psychiatrists who were trained in culturally appropriate care practices, and who understood the culture and community that they served (Brooks et al. 2013).
Beginning in 1997, the DOP fellows have travelled to one or several neighbor island communities each week for a period of 6 months to provide on-site psychiatric services at the CAMHD FGC. Supervision was shared by the CAMHD clinical director and the UH faculty who accompanied the fellow. Ron Snead, MD, the department's first supervising faculty for the rural rotation, strongly encouraged his trainees to, “show up consistently, and let the community guide you as how best to care for its families.” In 2008, the UH TMH program was developed by DOP faculty who were the first to train with Dr. Snead and CAMHD clinical directors who graduated from DOP's CAP program. These child and adolescent psychiatrists were strongly influenced by the rural community rotation and were committed to serve those communities where they had trained. The success of this training program has been facilitated by the consistent communication and interactions among the CAMHD clinical directors and UH faculty with the clinical and administrative staff, contracting agencies providing clinical services, and the institutions that commonly interact with families, including schools, primary care, social welfare, and the juvenile justice agencies (Savin et al. 2011). To ensure that the quality of care, treatment goals, and outcome objective benchmarks are met, all treatment team members review clinical and administrative issues regularly. This level of oversight by the CAMHD clinical director and UH faculty allows for immediate adjustments in treatment planning. The evidence-based system of care treatment model and its effective integration of culturally appropriate child and adolescent mental health services provided from a diverse group of practitioners and community agencies is the foundation for the collaborative TMH program.
Currently there are eight weekly TMH clinics to the FGC on Hawaii Island, Maui County, and Leeward Oahu, with plans to expand to the FGC on Kauai. During their TMH clinic rotation, each fellow is paired with a supervising faculty for a period of 6–12 months, during which they make on-site visits to their communities every 8–12 weeks. CAMHD and UH clinical and administrative staff arrange and schedule each site visit to provide the opportunity for the fellow to meet with families and treatment team members, including pharmacists, pediatricians, probation officers, and educators, in their own community. The frequency of the community visits helps the fellows to understand the community's values and needs, reinforces the program's credibility, and demonstrates commitment to developing cultural rapport.
A priority for each TMH encounter with youth and their family is to include all available members of the treatment team, which is frequently achieved with single- or multiple-point IVTC connections and telephone conferencing. The success of a cohesive integration of an evidence-based system of care from a diverse group of service providers is dependent upon the strong alliance with the local CAMHD clinical leadership and administrative staff (Savin et al. 2011; Brooks et al. 2013). The care coordinator is the assigned social work specialist who interacts frequently and directly with the family and coordinates all mental health services. They are the primary contact with the family to address schedules and urgent and after-hour care, procure on-site translation services, and introduce and train families in the use of the IVTC technology. They attend every TMH clinic, treatment team and school meeting, and court hearing, and often provide frequent home visits when transportation and other psychosocial challenges are an issue. The care coordinator is the primary resource for providing the cultural and community context for the fellows. An important goal during a site visit is for the trainee to directly experience and appreciate the constellation of community-intensive work provided by the care coordinator.
Many youth in the TMH program receive special education services, and the teachers are integral and proactive members of the treatment team. The TMH program consults to teachers and school-based mental health therapists and provides direct services to youth at school. School staff join case conferences and participate in treatment team planning for youth transitioning from hospital- and community-based treatment programs through the DOE's Teleschool program, which provides a secure and enclosed network at district offices and school campuses statewide using high definition connectivity. These IVTC resources provide enormous flexibility in linking multiple treatment team members separated by significant distances especially in rural communities where the most practical meeting site is at the school.
TMH workforce development: Collaboration with the Mayo Clinic
In 2008, Dr. Naleen Andrade, professor and then chair of the DOP, and the late Dr. David Mrazek, then Professor and Chair of the Department of Psychiatry and Psychology at Mayo Clinic (Rochester, MN) shared the common goal of evaluating the role of TMH in training, education, and research; workforce development; and global service. The DOP has a unique history of sustaining relationship-building and mentoring with similar education and training goals in collaboration with colleagues at the University of Indonesia Child and Adolescent Psychiatry Program (Guerrero et al. 2014).
The CAP Fellowship
The Mayo Clinic and DOP CAP programs developed a collaboration to use IVTC technology to support a joint monthly clinical case conference and consultation. The shared training experience provides specialized expertise for the evaluation of complex diagnostic issues, pharmacogenomics, the cross-cultural aspects of CAP, and the translation of this expertise to the multiethnic communities in rural Hawaii. The DOP has been able to consult with our Mayo Clinic colleagues on a number of cases involving Native Hawaiian and Pacific Islander youth who responded poorly to appropriate dosing strategies of psychotropic medication. Pharmacogenomic evaluation identified the phenotypes of the youth as either being poor or ultrarapid metabolizers for the respective medications, resulting in effective and timely adjustments in treatment. The DOP is now able to access convenient and routine pharmacogenomic evaluation for children living in rural communities. The DOP's TMH program provides our Mayo Clinic colleagues the opportunity to appreciate cultural context in psychiatric formulation and treatment planning for youth with mental health conditions, as >70% of Hawaii's residents are of Asian and/or Native Hawaiian and other Pacific Islander ancestry or of mixed ethnicities (United States Census Bureau 2012). Through TMH, they engage with the youth, families, and treatment team members, often connecting from different neighbor islands requiring multiple-point IVTC connections. For example, a conference may include the live patient interview with the youth at the Hawaii Youth Correctional Facility (Oahu) and mental health providers (social worker, therapist, and probation officer) located on a different island. This is just one example of TMH bridging families, mental health partners, and consultants across significant distances and with rich and varied cross-cultural backgrounds (Savin et al. 2011).
Recently, our colleagues at the Tripler Army Medical Center (Oahu), CAP program, joined the clinical case conferences by IVTC. This shared educational experience has heightened the participants' appreciation of the critical challenges of providing culturally appropriate child and adolescent mental health care to the Iraq and Afghanistan war veterans and their families returning to their home communities in rural Hawaii (Brooks et al. 2012; Doarn et al. 2012).
The DOP CAP program is well poised to serve and develop the workforce for rural and neighbor island communities. A growing number of faculty is experienced with the use of IVTC technology. They are triple-board trained, collaborate with primary care physicians, are recognized for their research in program evaluation and addressing mental health disparities, and are committed to serving Hawaii's rural communities (Helm et al. 2010). Since 2008, nearly 70% of the DOP child fellows completing their training have joined the DOP faculty or CAMHD, and continue to provide TMH services to youth and their families in rural Hawaii (Chung-Do et al. 2012).
Medical Student Training
Hawaii faces significant healthcare challenges including an increasing shortage of physicians on all islands including Oahu (Withy et al. 2012). Native Hawaiians, Asian Americans, and Pacific Islanders are overrepresented in the increasing rates of diabetes, obesity, and other chronic illnesses. In 2012, 90% of the entering first year medical student class were residents of Hawaii, and many lived in the neighbor islands (John A. Burns School of Medicine 2013).
The UH John A. Burns School of Medicine (JABSOM) provides a longitudinal clinical training experience for its 3rd year medical students. Approximately one third of the class will choose the opportunity to train in ambulatory clinics in rural communities statewide for a period of 6 months. Students are supervised by UH residents and clinical faculty at the community sites. However, with the increasing physician shortage affecting all of Hawaii, student supervision by on-site clinical faculty is harder to achieve. The goals for the DOP TMH program are to increase the exposure and opportunities for medical students to participate in child psychiatry programs, and introduce the student to rural community integrated behavioral healthcare during their psychiatry clerkship rotation. Pullen et al. (2013) reported that interest in CAP among undergraduate medical students increased after participating in an interactive psychiatry curriculum provided by the Mayo Clinic CAP program using IVTC technology.
For the past 2 years, JABSOM students rotating in the rural Hawaii Island community of Waimea have participated in a half-day TMH clinic each week. They work directly with families and community-based mental health and DOE providers. Both the on-site CAMHD clinical director and remote DOP psychiatry fellow and faculty share the responsibility for supervision and evaluation of the students. Students reported that the experiences have given them the opportunity to envision the integration of IVTC technology in their own professional development as physicians and future clinical work in Hawaii's rural communities.
Primary care initiative
Collaborating with the Department of Health and local Community Health Centers, the DOP created the Primary Care Initiative to investigate novel methods to integrate behavioral health into the pediatric medical home. Initial assessment of community needs and resources revealed a shortage in child behavioral health providers accepting patients with Medicaid coverage and further difficulties in accessing care, especially within rural areas with large Native Hawaiian/Pacific Islander populations. Families and community providers also expressed a desire for culturally relevant mental healthcare delivered in their community.
Utilizing TMH, the DOP is able to reach underserved rural and neighbor island populations, and collaborate with primary care colleagues to deliver quality, culturally sensitive mental healthcare in the community. Building on the successful TMH clinics, child psychiatry trainees have been involved in all phases of the Primary Care Initiative project to provide experiences working with primary care providers, and to promote sustainability of integration efforts. The Primary Care Initiative provides education sessions and telephone consultation, and plans to begin case conferences and direct patient evaluations at the local Community Health Centers using IVTC.
Although current TMH technology provides instant connections to remote areas, the quality of equipment and familiarity with TMH varies greatly among sites. Addressing these TMH utilization challenges was essential for effective collaboration with families and healthcare partners. Problems with network quality and encryption capability of older equipment were identified in the course of the project, which were addressed with use of hardwire connections and HIPAA-compliant cloud video conferencing, respectively. Subsequently, community health centers that initially were hesitant to use TMH technology quickly acclimated to its use with increasing exposure and technical support. Although the flexibility of TMH was invaluable, intermittent face-to-face visits provided further opportunities for community engagement and strengthened the relationships that are the foundation of successful integration endeavors.
IVTC technology and future directions
Hardware-based, or “legacy” video teleconferencing systems, have traditionally been difficult to implement because of their high upfront costs, relative immobility, the technical expertise needed to manage them, and their low-latency high-speed Internet requirements. The DOP's TMH program deployed legacy IVTC units in clinics that had adequate technical support, infrastructure, and funding; however, such systems are not feasible for rural clinics without adequate infrastructure and supports.
In order to overcome many of the barriers of the legacy systems, the TMH program is moving to different technology and is examining HIPAA-compliant cloud videoconferencing for future deployments. With cloud videoconferencing services, stakeholders can connect with each other through various devices, such as their existing computer, smart phone, or tablet, equipped with a microphone and webcam. Users simply download an application or link to a web site to join a video session. Most of these video software programs are designed to be firewall friendly, precluding concerns about complicated network configurations. Sophisticated algorithms that monitor the network connection are incorporated into the software and automatically adjust the call quality based on the available bandwidth, ensuring adequate connectivity under various network conditions (e.g. Wi-Fi, 3G, and 4G). With hosted videoconferencing, the service provider manages all of the back-end technology infrastructure. Smaller sites then have reduced need for on-site technical support.
Conclusions
The DOP's TMH program is an ideal model demonstrating how academic and state programs can build a virtual team of expert mental healthcare providers that develops and extends the CAP workforce, collaborates with primary care and other community partners, and telecommutes expertise from other national leaders so as to provide state-of-the-art pharmacotherapy and culturally appropriate care to youth and their families in their own community.
Clinical Significance
The DOP's TMH program is more than the sum of its parts in the provision of timely evidence-based mental health services for children and their families living in ethnoculturally diverse communities in rural Hawaii. Our TMH program integrates new technology in a successful evidence-based system of care treatment model, and broadens the access to psychiatric services for Hawaii's youth. The TMH program will continue to address the growing challenges of rectifying mental healthcare disparities for children of Hawaii and the Pacific Islands, to creatively leverage community resources in ongoing treatment, to support primary care providers, and to examine the cultural influences associated with family engagement and treatment outcomes provided by TMH.
This is only one of many TMH models that emphasize the concerted and converging efforts of legislative, academic, state, and community stakeholder commitment and initiative to provide evidence-based and culturally appropriate care to a growing population living in rural communities. The skill set of the TMH champions will continue to be refined, as developing IVTC technology and evidence-base therapies are integrated into the new landscape of healthcare reform.
Footnotes
Disclosures
No competing financial interests exist.