
Abstract
Background:
An abnormality in long chain-polyunsaturated fatty acid (LC-PUFA) levels has been implicated in attention-deficit/hyperactivity disorder (ADHD). Studies evaluating LC-PUFA supplementation for therapeutic efficacy in ADHD have shown mixed and, therefore, inconclusive results.
Methods:
Seventy-six male adolescents (age 12–16 years, mean = 13.7) with ADHD were assessed for the effects of 12 weeks omega-3 and omega-6 supplements on biochemical and psychological outcomes in a randomized, placebo-controlled, clinical trial. The primary outcome measure was change in the Conners' Teacher Rating Scales (CTRS) following 12 weeks of supplementation of LC-PUFA or placebo. At baseline, the placebo and treatment groups had comparable levels of LC-PUFA as measured by red blood cell phosphatidylcholine. In the treatment group, supplementation enhanced eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and total omega-3 fatty acid levels.
Results:
No superiority of LC-PUFAs to placebo was observed on the primary outcome. Further, there were no reliable treatment effects on aggression, impulsivity, depression, and anxiety.
Conclusions:
Future studies should use larger sample sizes and longer supplementation period to detect small-modest effects for clinical recommendations in ADHD.
Introduction
A
Research spanning the last 3 decades has supported the role of long-chain polyunsaturated fatty acids (LC-PUFAs) in neurodevelopment (Marszalek and Lodish 2005). Eicosapentaenoic acid (EPA, omega-3), docosahexaenoic acid (DHA, omega-3), γ-linoleic acid (GLA, omega-6), and arachidonic acid (AA, omega-6), docosapentaenoic acid (DPA, omega-6), are members of the omega-3 and omega-6 fatty acids family. Their parent compounds are α-linoleic acid (ALA) and linoleic acid, respectively.
DHA is especially concentrated in synaptic regions of the brain, and constitutes ∼30% of the ethanolamine and serine phosphoglycerides of brain tissue (Crawford et al. 2009). Within brain tissues, DHA preferentially accumulates in growth cones, astrocytes, synaptosomes, myelin, and microsomal and mitochondrial membranes (Bourre et al. 1992). The perinatal increase in cortical DHA concentrations coincides with active periods of neurogenesis, axonal myelination, and synaptogenesis (Green et al. 1999; Cao et al. 2009; Yavin et al. 2009). Animal studies have provided robust evidence that changes in retinal and brain DHA can alter neuronal structure and function (Zimmer et al. 2000a,b). Diets deficient in ALA lead to a lower accumulation of DHA in brain phospholipids, and structural changes in membranes in the central nervous system are in turn related to behavior (Sinclair and Crawford 1972; Fienners and Sinclair 1973; Reisbick et al. 1994). Depriving rats of omega-3 fatty acids results in behavior abnormalities, but repletion of DHA reverses the effect (Moriguchi et al. 2000; Levant et al. 2004; Chalon 2006; Fedorova and Salem 2006).
EPA is important in its role in the production of eicosanoids that have anti-inflammatory, antithrombotic, and vasodilatory properties. EPA inhibits the manufacture of several inflammatory cytokines such as interleukins 1 β and 6 and tumor necrosis factor α, which are implicated in depression (Salem et al. 2001a,b; Song et al. 2008).
ADHD has frequently been associated with abnormal erythrocyte and plasma levels of omega-3/6 fatty acids (Stevens et al. 1995, 1996; Chen et al. 2004; Antalis et al. 2006). Improvement of symptoms following supplementation has been reported in a range of related disorders including depression (Peet and Horrobin 2002; Nemets et al. 2006), risk from suicide (Sublette et al. 2006), and aggression/anti-social behavior (Corrigan et al. 1994; Gesch et al 2002; Zaalberg et al. 2010); and poor developmental outcomes have been reported if the maternal consumption of seafood (high omega-3) is <340 g per week (Hibbeln et al. 2007).
Several randomized, placebo-controlled, double-blind trials with omega-3/6 fatty acids in children/adolescents with symptoms of either ADHD, literacy/reading and writing difficulties (e.g., dyslexia), or developmental coordination disorder have reported statistically significant improvements in learning and/or behavior (Richardson and Puri 2002; Richardson and Montgomery 2005; Sinn and Bryan 2007; Richardson et al. 2012), whereas others have reported little (Johnson et al. 2009) or no effect (Voigt et al. 2001; Hamazaki and Hirayama 2004). Supplementation trials using fatty acid fortified foods have thus far appeared to be the least successful (Hamazaki and Hirayama 2004).
Bloch and Qawasmi (2011) conducted a recent meta-analysis of 10 well-designed trials involving 699 children. They reported that omega-3 supplementation had a small but statistically and clinically significant effect size in reducing symptoms of ADHD (effect size standardized mean difference [SMD] = 0.31, 95% confidence interval [CI] 0.16–0.47, z = 4.04, p = < 0.001). When the different omega-3 fatty acids were considered separately, higher doses of EPA (which collectively ranged from 80 to 750 mg daily) were significantly but modestly correlated with efficacy (β = 0.36, 95% CI: 0.01–0.72, t = 2.30, p = 0.04, R2 = 0.37). Doses of other omega-3 LC-PUFAs such as DHA and ALA were not significantly related to efficacy. A Cochrane review authored by Gilles and colleagues (2012) included 13 studies. They reported a somewhat higher improvement in the omega-3/6 fatty acid intervention group (relative risk [RR]: 2.19, 95% CI: 1.04–4.62); however, there were no statistically significant differences in parent-rated or teacher-rated ADHD symptoms when all participants receiving LC-PUFA supplements were compared with those receiving placebo. Further research was considered necessary. Sonuga-Barke and colleagues (2013) provided the most recent meta-analysis. Eleven omega-3 and/or omega-6 supplementation trials met their inclusion criteria. Five involved omega-3 supplements, two involved omega-6 supplements, and the remainder used both omega-3 and omega-6 supplements. The overall result was a small, but there was statistically significant preference for supplementation over placebo (SMD = 0.21).
Bloch and Qawasmi (2011) highlighted the valid point that available studies have small sample sizes and individually lack the statistical power to demonstrate a substantive effect. Other potential reasons for the lack of consistent findings in the clinical trial literature are the large variation in methodological design, differences in dose, duration of supplementation (e.g., 8, 12, 16, or 34 weeks), and choice of formula of fatty acids used (e.g., EPA-rich versus DHA-rich). Biochemical results are mostly not reported; therefore, it may be unclear whether supplementation had its intended effect. ADHD diagnosis is often neglected. Parents are usually both the deliverers of the treatment and the raters of its effect, with the possibilities arising that concealment of allocation may be compromised, or that responses will be magnified subjectively because of the effort that has been expended.
Methods
In consideration of the research to date, the primary aim of the present study was to investigate whether LC-PUFA supplementation was a safe and effective treatment in the context of a 12 week, randomized, placebo-controlled, double-blind clinical trial named “The Maudsley Adolescent ADHD Fatty Acid (MAAFA) trial.” This was a collaborative research trial with London Metropolitan University. The key objective of the trial was to assess whether LC-PUFA supplementation would improve symptoms of ADHD at 12 weeks postrandomization as measured by Conners' Teacher Rating Scales (CTRS-L), which assessed each of 59 items of child behavior on a four point scale (Conners et al 1998). The secondary objective tested whether blood levels of fatty acids increased postsupplementation and whether other beneficial effects on problems associated with ADHD could be detected.
Participants
A total of seventy-six male adolescents were recruited for this study (Fig. 1). At the time the study was designed, the meta-analyses of effect sizes described were not available, and the sample size was, therefore, calculated using an expected effect size of 0.7, in order to be comparable with the effect sizes of established therapies such as parenting classes or stimulant medication. This resulted in a total of 38 patients (which included an additional 10% dropout rate) in each intervention arm. Subjects who met eligibility criteria were randomized by the Mental Health and Neuroscience Clinical Trials Unit based at the Institute of Psychiatry, King's College London. Allocation was stratified by whether the adolescent attended a day or boarding school, and by age group (12–14 years and 15–17 years) using minimization randomization. Participants were drawn from various special educational settings (e.g., boarding schools, mainstream schools with provision for students with emotional and behavioral difficulties) in England. Subjects who were taking concomitant medication underwent a 48 hour washout period for stimulant medication, prior to their assessment visit.
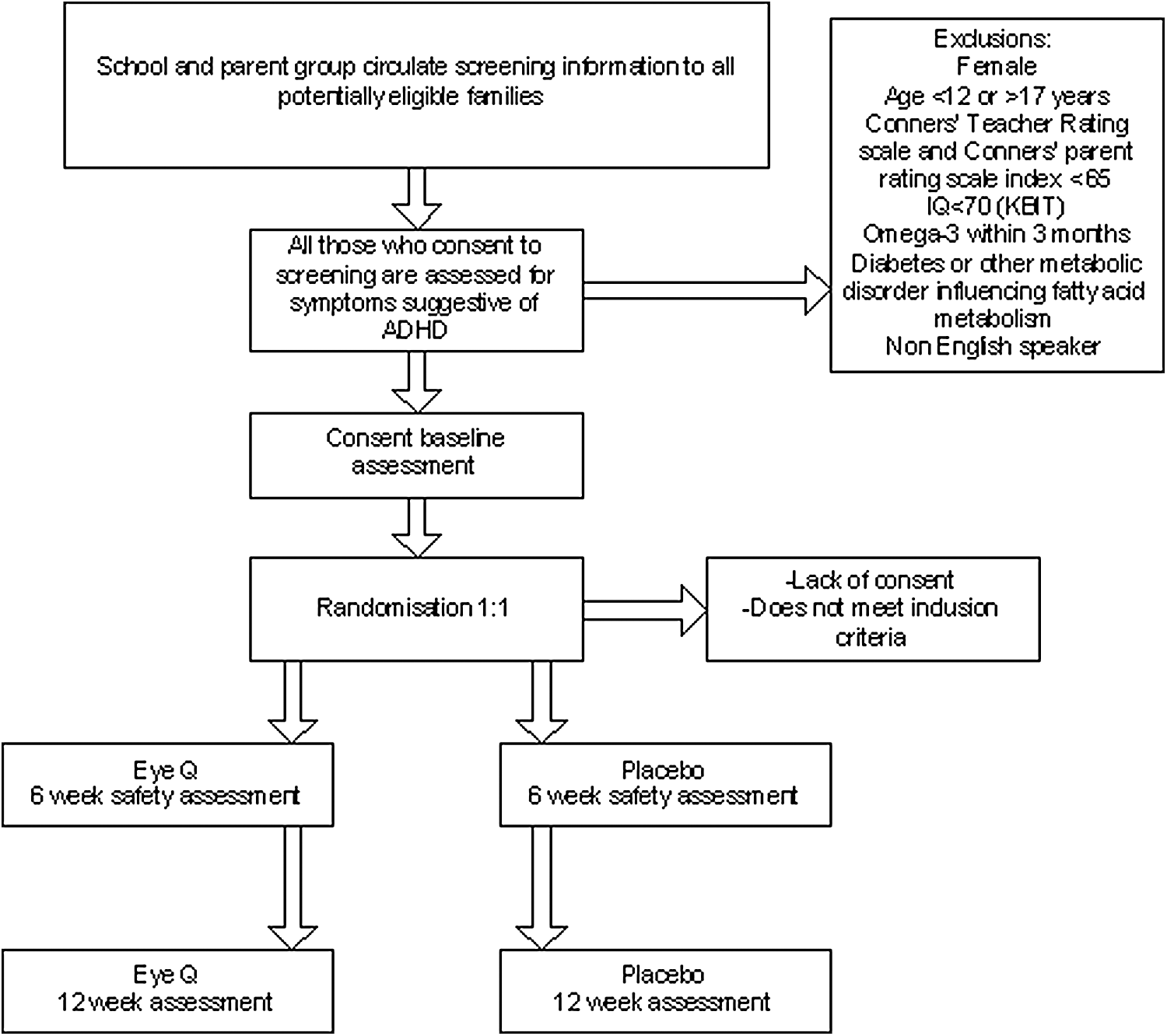
Flow chart of participants.
Criteria for inclusion were based on a mean standardized score >65 (>95th percentile) on both CTRS-L and the Conners' Parent Rating Scales (Conners et al. 1998), and being between 12 and 17 years old. Intelligence quotient (IQ) had to be >70, and was assessed using the Kaufman Brief Intelligence Test, Second Edition (KBIT-2) (Kaufman 2004). A diagnosis of ADHD was confirmed through a semistructured interview based on Diagnostic and Statistical Manual of Mental Disorders, 4th ed (DSM-IV) criteria (Children's Interview for Psychiatric Syndromes [ChIPS]) (American Psychiatric Association 1994; Rooney and Weller 1999). The Barratt Impulsivity Scale was also performed to describe characteristics of the participants (Patton et al. 1995).
Subgroup analysis of ADHD
The ADHD group was assessed into subgroups by the ChIPS, and 65.8% were found to have the combined type, 23.7% were found to have the inattentive type, and 10.5% were found to have the hyperactive/impulsive type.
Ethics
This study was approved by the Research Ethics Committee in the UK (MREC: 06/Q0702/19). It was conducted as a formal “clinical trial using medication,” and obtained an International Standard Randomized Controlled Trial Number (ISRCTN27741572).
Informed consent/assent was obtained from participants and their parents, according to the National Health and Medical Research Council (UK) guidelines. Adolescents, parents, and teachers gave signed consent to take part, and were fully briefed on the ethical considerations of the study. They were also advised they could withdraw at any point with no obligation.
Procedure and materials
Each subject was accompanied by a caregiver to The Institute of Psychiatry at The Maudsley Hospital, where ∼15 mL of fasting blood was taken followed by the baseline assessments that included electroencephalography/event-related potential and neuropsychological assessments (not reported in this article). The blood was taken by a qualified phlebotomist and stored at −80°C.
Total red blood cell lipid analysis
Total lipids were extracted from 1 mL of red blood according to the Folch method (Folch et al. 1957). The red cells were homogenized in chloroform and methanol (2:1 v/v) containing 0.01% butylated hydroxytoluene as an antioxidant, under nitrogen. Fatty acid methyl esters (FAMEs) were prepared by heating the extracted total lipid in 4 mL of 15% acetyl chloride in methanol for 3 hours at 70°C, under nitrogen in a sealed vial. FAMEs were separated by a gas-lipid chromatograph (HRGC MEGA 2 series, Fisons Instruments, Italy) fitted with a capillary column (30 × 0.32 mm inner diameter, 0.25 μm film, BP20). Hydrogen was used as a carrier gas, and the injector, oven, and detector temperatures were 235°C, 250°C, and 178°C, respectively. FAMEs were identified by comparison with relative retention times of authentic standards and calculation of equivalent chain length values. Peak areas were quantified by a computer chromatography data system (EZChrom Chromatography Data System, Scientific Software Inc., San Ramon, CA). Results are expressed in ng/mL.
Interventions
The investigative medicinal product or active treatment was LC-PUFA capsules, Equazen Eye Q. The daily dose of six capsules provided a combination of omega-3 fatty acids (EPA 558 mg and DHA 174 mg), omega-6 fatty acid γ-linoleic acid 60 mg, and vitamin E 9.6 mg (in the natural form, α-tocopherol). This, or indistinguishable placebo (medium chain triglycerides) as a placebo, was given for a 12 week period. These were provided in four identical bottles labeled with an identifying code and in compliance with good manufacturing process. Bottles were collected at the end of the study and assessed for compliance. At 6 weeks, parents and teachers were contacted by telephone or e-mail to monitor adverse effects and compliance. All primary and secondary measures were evaluated at baseline and following 12 weeks of intervention.
Outcomes
Primary analysis
The primary analysis performed on the intention to treat (ITT) complete case sample was statistically analyzed by applying a linear regression of ADHD index adjusted for baseline CTRS ADHD index, school type (day, boarding), age (≤14, ≥15) and an indicator variable for treatment (LC-PUFA, placebo). The ADHD index t. value was used to test the null hypothesis that the treatment coefficient in the model is zero. Rejection of the null hypothesis at the two sided 5% significance level was considered to be a successful demonstration of efficacy.
Secondary analysis
The model used to complete each secondary analysis was a linear regression outcome on the ITT complete case sample adjusted for corresponding baseline score, school type (day, boarding), age (≤ 14, ≥ 15) and an indicator variable for treatment (LC-PUFA, placebo). ADHD index t value was used to test the null hypothesis that the treatment coefficient in the model is zero. Rejection of H0 at the two sided 0.0083% significance level was considered to be a successful demonstration of efficacy.
Safety analysis
Summaries of incidence rates (frequencies and percentages), severity, and relationship to drug of adverse events and reactions classified by body system were prepared. A participant may have been counted more than once within each body system. Summaries were presented for each treatment group for those participants in the safety sample. Only events starting after randomization were included. Fisher's exact test was performed at the 5% significance level to test the association between adverse events and reactions by body system and event type.
Patients
The patient disposition across the different data sets analyzed was well balanced between the safety data set and the ITT data set. The per protocol analysis had four (15%) more patients in the placebo intervention than in the LC-PUFA intervention. Treatment groups were homogenous with respect to demographics.
Results
Demographics
One hundred and thirty-eight patients were screened for eligibility (Table 1). Of those, 76 male adolescents were randomized. Six randomized patients did not receive either intervention before withdrawing from the study, and 86% of participants randomized (65) were day students in school. The age range was between 12 and 16 with a mean age of 13. 7 years. The mean composite IQ score was 96.1 (SD = 12.8), which did not differ significantly between active and placebo groups at baseline. A total of 15 subjects were taking concomitant medications as confirmed by interview, of which 7 were randomized into the placebo group and 8 were randomized into the treatment group.
IQ, intelligence quotient; K-BIT2, Kaufman Brief Intelligence Test, 2nd ed., ADHD, attention-deficit/hyperactivity disorder; ChIPS, Children's Interview for Psychiatric Syndromes; CTRS, Connors' Teacher Rating Scale; CPRS, Connors' Parent Rating Scale.
Primary outcome
Linear regression of the CTRS ADHD index adjusted by treatment, baseline ADHD index score, school type (day, boarding), and age (<15 years, ≥15 years) failed to show a significant difference between treatment at 12 weeks (p = 0.671) (Fig. 2). This analysis was performed on the ITT complete case sample consisting of 69 patients (placebo = 36, LC-PUFA = 33). Sensitivity analysis on the ITT complete case sample was conducted by adjusting by the treatment and baseline ADHD index score only. This analysis failed to show a significant result between treatment at 12 weeks (p = 0.617). Per protocol, complete case analysis was performed on 50 participants (placebo = 27, LC-PUFA = 23) using the same method as the ITT complete case sample. The analysis failed to show a significant difference between treatment at 12 weeks (p = 0.164). Removing points of influence also failed to show a significant outcome at the 5% level.
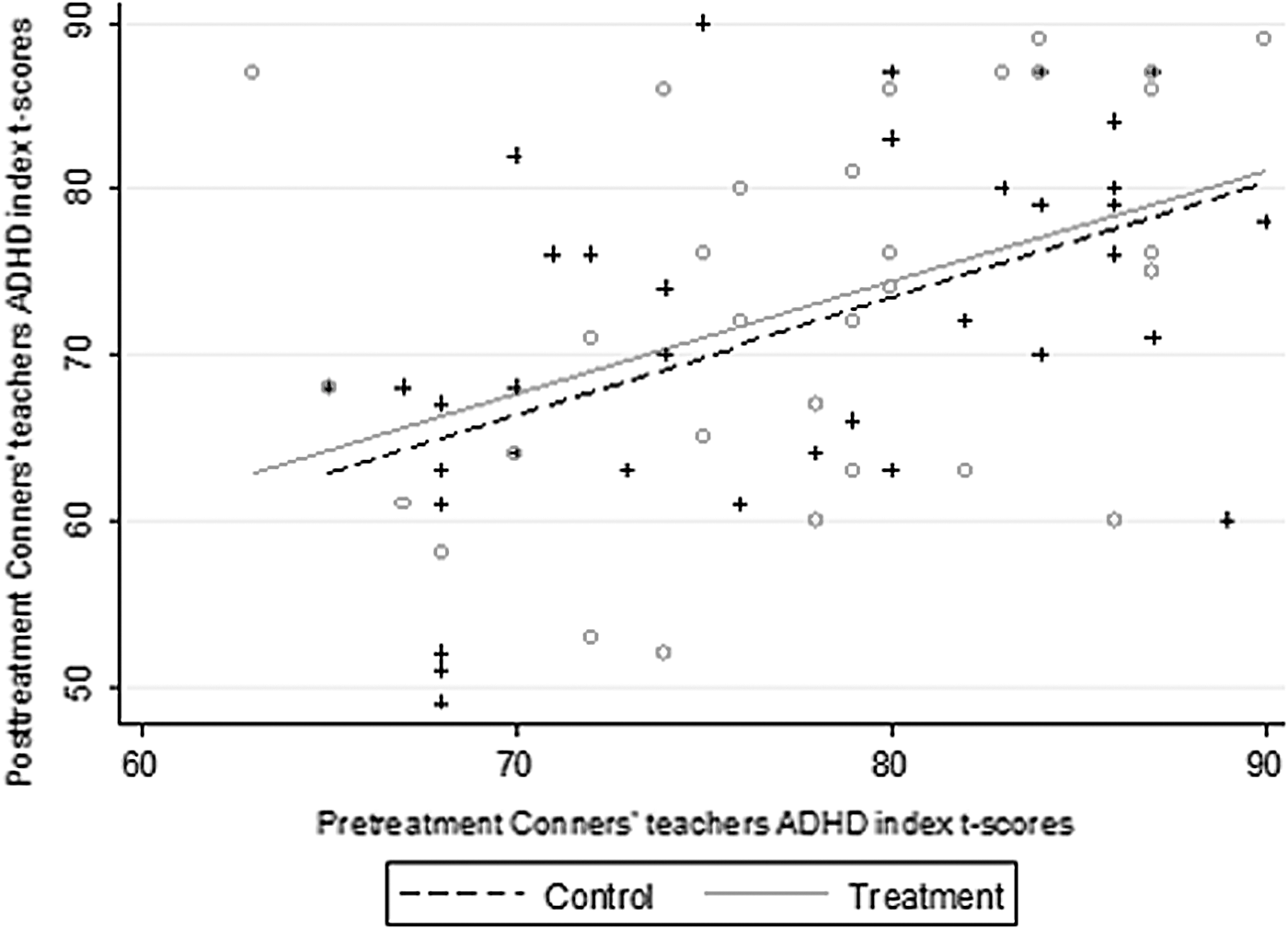
Pretreatment and posttreatment scores by treatment of the Conners' Rating Scale Teacher Attention-Deficit/Hyperactivity Disorder (ADHD) Index t scores. Pretreatment and posttreatment scores in each group showing fitted lines. The difference between the two groups is shown by the vertical distance between the two lines.
Pretreatment and posttreatment scores in each group showing fitted lines. The difference between the two groups is shown by the vertical distance between the two lines.
Secondary outcomes: Biochemical results
There were changes in the expected direction on red blood cell phosphatidylcholine measures (Table 2). Total omega-3 levels rose from a mean of 2.57 (SD 0.75) to 2.73 (SD 0.73) in the control group; and from 2.60 (SD 1.16) to 3.62 (SD 1.21) in the group receiving supplementation; p < 0.001. Both EPA and DHA levels rose significantly from the baseline to the end of the trial in the group receiving supplementation, but not in the controls. On the other hand, DPA, which shares the same enzyme for conversion with DHA, was decreased after intervention in the active group. GLA level did not increase significantly.
Mean ± SD (%).
No difference between control and active group before intervention.
No difference before and after intervention in control group.
Compare means before and after intervention in active treatment group: * p < 0.05, ** p < 0.01.
DPA, docosapentaenoic acid; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid.
Secondary outcomes: Impulsiveness
To account for multiplicity, an unadjusted p value = 0.0083 needed to be achieved to declare a significant outcome. The total impulsivity score of the Barratt impulsivity scale showed some indication of an increase in the LC-PUFA group after supplementation (Table 3). The observed results were not free from bias, as there was selection of participants who did not return the baseline and/or 12 week questionnaires.
Mean ± SD.
p = 0.014 ** p = 0.024.
The numbers for a complete case analysis were only 27, as only a subset of participants completed the baseline and week 12 outcomes for this measure. Per protocol, complete case analysis indicated a 3.1 point increase in the LC-PUFA group (95% CI [0.4, 5.9] p = 0.028).
No significant changes were noted for the Conners' Parent Rating Scale.
Safety results
A total of five 5 patients, 7%, of the safety sample (70 patients) had an adverse event (placebo = 2, LC-PUFA = 3). Out of these five patients, four had more than 1 adverse event, as 12 adverse events were reported in total (placebo = 7 adverse events, LC-PUFA = 5 adverse events). Ten of the adverse events were reported as mild in severity. One was classed as moderate, a bone fracture that occurred on the LC-PUFA intervention, but was thought to have no relation to the drug. Three patients withdrew from treatment because of adverse events reported. Fisher's exact test failed to show a significant difference between the adverse events and treatment reported at the 5% level (p = 1.000).
One patient, who had withdrawn from the trial early, returned 127 days after initial randomization and requested that the fatty acids should be resumed. This was agreed to (but not as part of the trial); but on the 2nd day he had a seizure. This serious adverse event subsequent to the trial was deemed to be remotely related to the LC-PUFA intervention, and the event was moderate in severity.
Discussion
This intervention study demonstrated that the primary outcome failed to show a significant difference between active and placebo intervention at 12 weeks. The fatty acid supplementation used in this study, which contained a higher ratio of EPA (6 capsules = 558 mg) compared with DHA (174 mg per 6 capsules) and some GLA (60 mg per 6 capsules), did not improve teacher-rated ADHD symptoms at 12 weeks follow-up. Similar results were reported for the teacher scores by Sinn and Bryan (2007).
The likely reasons for the negative outcome may include the lack of statistical power, dropping out (19 participants), and/or dose of the supplement. Our results do not exclude a small effect of the size suggested by the recent meta-analyses. In this study, male adolescents were invited to the study because the symptoms can be evaluated more clearly than at a younger age, and ADHD is more common in males than in females. A different study population and a larger sample size may have shown the significant effect of LU-PUFA supplementation.
The results of blood analysis showed a significant increase of DHA levels whereas the level of GLA did not change after intervention in the active treatment group. This suggests that the dose of the supplement for intervention might not have been high enough to affect the results. A recent meta-analysis by Bloch and Qawasmi (2011) involving 10 trials and 699 children indicated that higher doses of one omega-3 fatty acid were significantly, although modestly, correlated with supplement efficacy in the treatment of ADHD.
The relative efficacy of omega-3 fatty acid supplementation appears to be modest in contrast to currently available pharmacologic interventions; for example, psychostimulant medication for ADHD. However, taking into consideration its relatively mild side effect profile and evidence of modest efficacy, it may be rational to use omega-3 fatty acids to supplement traditional pharmacologic interventions, or for subjects who resist or are resistant to psychopharmacologic options. Other studies also lend support to the potential beneficial effects of EPA in alleviating symptoms of low mood and depression (Peet and Horrobin 2002; Freeman et al. 2006; Bloch and Qawasmi 2011), in keeping with the notion that EPA and DHA have separate roles in the brain (Young and Conquer 2005).
Taking into consideration the significant effects of LC-PUFA supplementation reported elsewhere over a 6 month period (Richardson and Montgomery 2005; Sinn and Bryan 2007) the length of the present intervention may have been too short to have a measurable impact on behavior, especially if correcting a deficiency. Because the red blood cell survives ∼120 days in the body, 12 weeks (84 days) of supplementation might not be long enough to change the LC-PUFAs compositions.
Another possibility is that there could be a need to provide AA rather than GLA (Antalis et al 2006). Further, the combined effects of methylphenidate (MPH) and omega-3/6 fatty acids are not well reported. A recent study by Barragán et al. (2014) reported that omega-3/6 fatty acids had similar effects to MPH, whereas the MPH plus omega combination appeared to have some tolerability benefits over MPH. Almost 20% of our sample (15 subjects) were taking psychostimulant medication, and the medication remained stable during the intervention trial. This could have affected their follow-up scores by both teachers and parents.
It is possible that the outcome measures (i.e., the CTRS) were not sensitive enough to detect small improvements in behavior. Teacher rating scales are often problematic, and raise multiple questions concerning reliability (Sinn and Bryan 2007). In our study, we experienced the occasional problem of a changeover of teachers during the intervention period. Several teachers were on sick leave and/or left the school prior to the collection of final scores. It is likely that any change in teacher scoring would have affected the overall scores. Arguably, new teachers will know a student less well than teachers who have worked consistently with that student for a considerable length of time.
The results of the secondary analyses are less reliable then hoped, because of large levels of missing data both at baseline and at week 12. This reflected difficulties in compliance for parents in this school-based setting, and should be reckoned with in future such studies. In some cases, the model's fit may be questioned. A rule of thumb is that there should be 10 participants for each covariate fitted in the model (in our case, baseline outcome score, age, and school type). Covariates were not removed from the model, as they were prespecified a priori; however, in the majority of analyses, the covariates age and school were not found to be significant, and may not be needed in the model if a larger trial is performed. Other covariates might have explained more variation.
The study did not have sufficient power to detect an effect size <0.7 SD. We initially chose this size of effect to be comparable with other interventions for ADHD; but considering the ready availability and acceptability of the intervention, a smaller effect size and larger numbers should be considered for future work.
Conclusions
In this study, UK adolescent males with ADHD did not show the hypothesized level of benefit from 3 month LC-PUFA supplementation. It is still unknown whether other specific populations, types of LC-PUFA supplement, and alternative intervention periods can show more effects of LC-PUFA treatment. However, many parents of ADHD children still prefer to use LC-PUFA supplements, particularly when their children do not respond to psychostimulant medication and/or experience side effects. The negative evidence reported here is not strong enough to assert the ineffectiveness of LC-PUFA supplementation for ADHD. It may be too early to disappoint people's expectations of LC-PUFAs, and further research with the methodological improvements suggested here is strongly advised.
Footnotes
Clinical Significance
LC-PUFA use can still be considered as an alternative treatment for ADHD in children, but further research is needed.
Disclosures
No competing financial interests exist.