
Abstract
Objective:
The purpose of this study was to investigate therapy switching from methylphenidate (MPH) to atomoxetine (ATX) in a clinical sample of Danish children and adolescents with attention-deficit/hyperactivity disorder (ADHD); specifically, to determine the duration of MPH treatment before switching to ATX, and the reasons leading to a switch in therapy.
Methods:
We included 55 patients with ADHD who switched from first-line MPH to second-line ATX during January 01, 2012 and May 15, 2014. Patient and treatment characteristics along with clinical reasons for switching therapy were extracted from individual patients' records.
Results:
Mean duration of MPH treatment until switch to ATX was 11.2 months (range = 0.3–28.5 months); 36% of the patients switched within the first 6 months, 56% within the first year, and 76% within 1.5 years of initiating MPH; 24% continued MPH treatment for up to 2.5 years prior to switching. Most common reasons for switching were “adverse events” (AEs) (78%), “wish for more optimal day coverage” (24%), and “lack of efficacy” (16%). Other reasons for switching included “patient/parental request” (13%) and “noncompliance” (2%). Most common AEs leading to switch were psychiatric disorders (insomnia, aggression, tic, depression, anxiety) and decreased appetite.
Conclusions:
Our findings highlight the importance of continuous evaluation of the need for prescription switch to ATX in children and adolescents treated with MPH, taking into consideration various factors including potential AEs, non-optimal day coverage, lack of efficacy, patient/parental preferences, and noncompliance. These factors should be considered, not only at the initial stage of MPH treatment but throughout the whole treatment course.
Introduction
P
The frequency of switching has been explored in observational studies using claims data. A study by Ben Amor et al. based on prescription claims data from Quebec extracted during 2007 and 2012, found that among 9431 children and adolescents prescribed stimulant therapy, the 1 year period prevalence of switching was 18.7%. Among the most switched-to categories were other formulations of stimulants (7.8%), atypical antipsychotics (5.5%), and atomoxetine (ATX) (4.7%) (Ben Amor et al. 2014). A retrospective study by Perwien et al. used enrolment, medical, and pharmacy claims data provided between 1997 and 1999 by health maintenance organization plans located in six states throughout the United States, to investigate treatment strategies in children and adults with newly diagnosed and pharmacologically treated ADHD. Among the 735 included subjects (0–18 years of age), therapy switching was observed in 11.6%, and occurred on average 165.5 days (SD = 147.4) after initiation of ADHD pharmacotherapy (MPH 66.4%, amphetamine mixed salts 21.6%, dextroamphetamine 8.4%, pemoline 3.1%, methamphetamine 0.4%). The study did not specify to which medicines the patients were switched (Perwien et al. 2004). A study by Sanchez et al. used data from the Texas Medicaid Vendor Drug Program to investigate different adherence measures (including switching rates) in a population of 9449 patients (5–18 years of age) with ADHD starting stimulant treatment during 2001–2002. The study found that the switching rate within 6 months from initiation of index therapy was 14.2% for patients whose initial therapy was modified-release MPH, 14.8% for patients whose initial therapy was mixed amphetamine salts, and 27% for patients whose initial therapy was immediate-release MPH. The switch-to medicines were not specified (Sanchez et al. 2005). None of the abovementioned studies described the underlying reasons for switching patients from one ADHD medication to another.
In this study, we focused specifically on therapy switching from MPH to ATX. ATX, a selective norepinephrine reuptake inhibitor, received United States Food and Drug Administration (FDA) approval in 2002 as the first nonstimulant medicine used for the treatment of ADHD in children ≥6 years of age and adults. ATX has since then been marketed in a number of countries worldwide (Garnock-Jones and Keating 2009), including Denmark in 2006 (Institute for Rational Pharmacotherpy 2006). Because of its efficacy and relative limited spectrum of documented AEs, ATX is recommended for treatment of ADHD along with the stimulants MPH and dextroamphetamine in the National Institute for Health and Clinical Excellence (NICE) guideline. According to the NICE guideline, the decision regarding which medicine to use should be based on the evaluation of factors such as the presence of comorbid conditions, AEs, compliance, abuse liability, cost, and preferences of the child/adolescent and/or the parent or guardian (National Institute for Health and Care Excellence 2013).
In Denmark, licensed medicines for the treatment of ADHD in children and adolescents include MPH, ATX, dextroamphetamine and lisdexamfetamine. MPH is generally considered first-line therapy followed by ATX. ATX, however, may be considered first-line therapy in patients with comorbid tic disorder, anxiety, and/or risk of substance misuse. Dextroamphetamine and lisdexamfetamine are considered third-line medications and are generally only prescribed if neither MPH nor ATX are efficacious. The stimulant modafinil, which is not licensed for the treatment of ADHD, is considered fourth-line therapy and its use is therefore limited (Danish Child and Adolescent Phychiatric Association 2008, 2012; Danish Health and Medicines Authority 2014).
Despite a 10-fold increase in the number of Danish children and adolescents redeeming one or more prescriptions of ATX during the period from 2006 to 2013, MPH is still prescribed four times more frequently than ATX (National Institute for Health Data and Disease Control 2014). Although this is most likely an indication that prescribers are following national prescribing guidelines, we expect that a subgroup of the patients initiating MPH as first-line therapy is subsequently switched to ATX for a variety of clinical reasons. Understanding the reasons for switching children and adolescents from MPH to ATX is particularly important in light of the NICE guidelines endorsing the use of ATX for the treatment of ADHD, along with the chronic nature of the disorder and need for long-term treatment (National Institute for Health and Care Excellence 2013). Such knowledge may potentially help prescribers more effectively identify patients who would benefit from a switch to ATX.
Previously, factors associated with parent-reported discontinuation of ADHD medication have been identified including psychological side effects and inadequate medication efficacy (Toomey et al. 2012). This combined with findings from a literature-based review suggest that important reasons for switching patients from MPH to ATX include lack of efficacy, AEs including exacerbation of comorbid conditions (e.g., tic, anxiety, sleep disturbances, and somatic symptoms), and potential for substance misuse (Prasad and Steer 2008). However, to the best of our knowledge, no previous studies have specifically investigated reasons for switching patients from MPH to ATX.
Based on a manual review of records for patients attending a Danish child and adolescent psychiatric hospital with records of switching from first-line MPH to second-line ATX, this study aimed at describing: 1) Duration of MPH treatment to switch to ATX and 2) reasons leading prescribers to switch therapy.
Methods
Design
This analysis was based on patient records' data entered into the electronic patient record (EPR) system of a Danish child and adolescent psychiatric hospital during the period from January 01, 2012 to May 15, 2014. This period was chosen to ensure access to individual patients' clinical notes in electronic form, because of the hospital migrating from a paper-based to their current EPR system in January 2012. Historic prescription and diagnostic information, however, was available in electronic form from before January 2012.
The hospital is one of five regional mental hospitals in Denmark, and covers a background population of ∼1,500,000 inhabitants. Patients (0–18 years) are generally referred by their general practitioner for diagnosis and treatment of a variety of psychiatric disorders. The present analysis is based on patient records' data for a subpopulation of outpatients attending the hospital for the treatment of ADHD.
The study was approved by the Danish Data Protection Agency (Jr. no. 2014-41-2885) and was conducted in accordance with the Danish Act on Processing of Personal Data. Clearance to analyze the data without obtaining consent from individual patients' parents or guardians was obtained from the Danish Health and Medicines Authority (Jr. no. 3-3013-535/1). According to Danish legislation, no ethics or institutional review board approvals were required for this study.
Study population
The study population was selected from a clinical sample of 1,692 patients with prevalent ADHD (International Classification of Disease, 10th Revision, Diagnostic Criteria for Research [ICD-10-DCR]: F90.X Hyperkinetic disorder and F98.8C Disorder of inattention without hyperactivity) during the period from January 01, 2012 to May 15, 2014. Eligible for inclusion were patients with prescriptions of both MPH and ATX (n = 292). After scrutinizing eligible patients' prescriptions, we excluded 55 patients whose initial MPH prescription was not first-line or whose initial ATX prescription was not second-line. Thus, we excluded previous non-ADHD treatment naïve patients and patients who had been prescribed another medication for ADHD (e.g., dextroamphetamine or lisdexamfetamine) in between MPH and ATX. The remaining 237 patients had records of switching from first-line MPH to second-line ATX and, therefore, were considered as switchers. Finally, we restricted the study population to switchers initiating first-line MPH after January 01, 2012, resulting in a study population of 55 patients. A flow chart of the study sample selection is displayed in Figure 1.
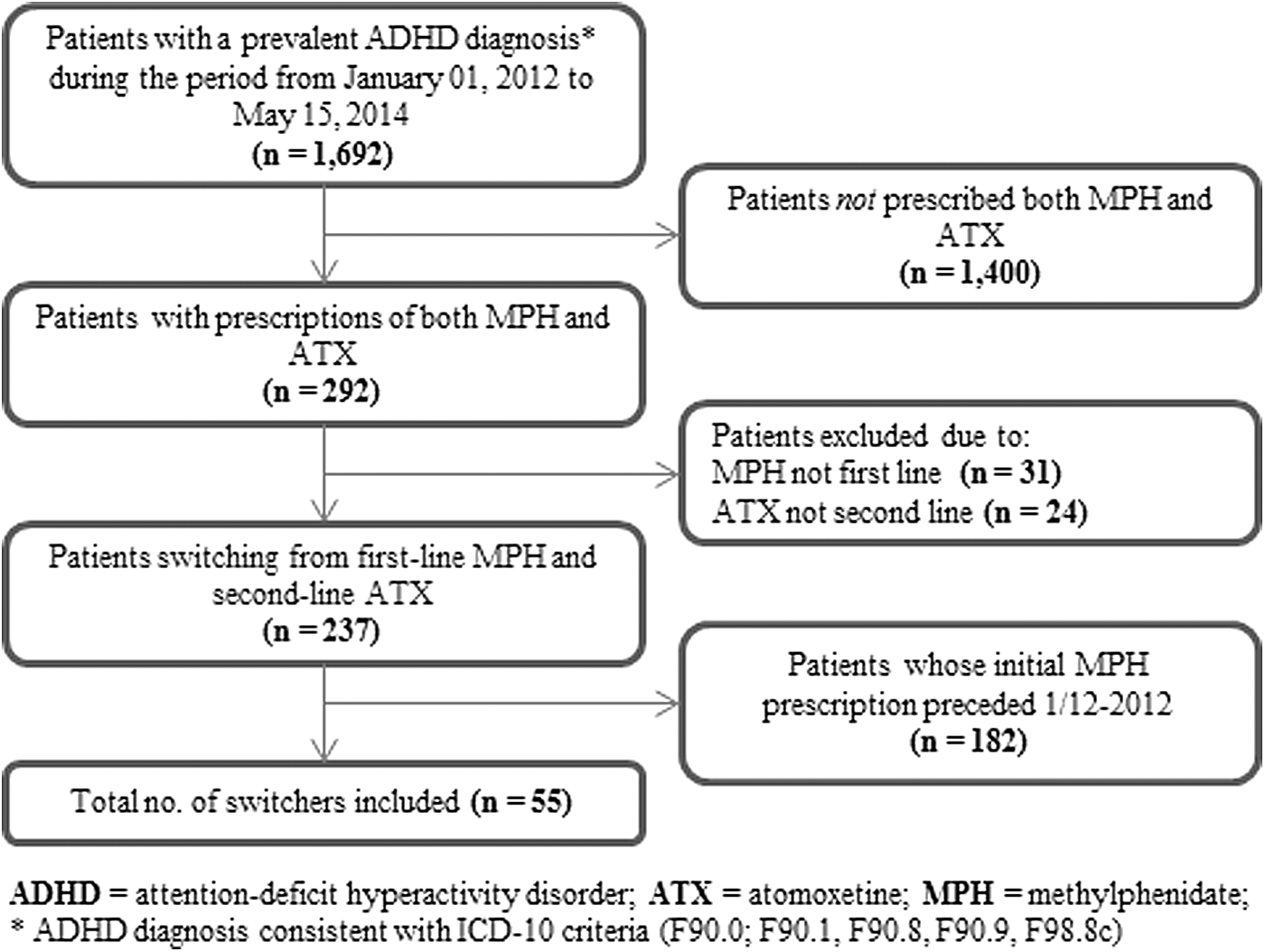
Flowchart of study sample selection (n = 55).
Outcome measures and classifications
The primary outcome measure was therapy switching, defined as switching from first-line MPH to second-line ATX. We did not consider switching between MPH formulations; for example, switching from immediate- to modified-release MPH formulations, which is considered standard practice (National Institute for Health and Care Excellence 2013), nor did we collect information about dosing regimen. It should be mentioned that patients at the hospital follow a standard treatment regimen based on dose titration; that is, initiating MPH treatment at the lowest possible dose and maximizing the dose until sufficient clinical effect is obtained or until the patient experiences intolerable AEs preventing further dose escalation. Accordingly, there is no reason to believe that the patients were undertreated or overtreated with MPH before being switched to ATX. The treatment regimen has been described in further detail in a previous study by Powell et al. (2011). Therapy switchers were required to have records of discontinuing first-line MPH and initiating second-line ATX, as switching from stimulant therapy to another ADHD therapy is sometimes done by a schedule allowing cross-tapering of treatments or with a longer washout period (Prasad and Steer 2008). No restrictions were applied as to when MPH was stopped and ATX was initiated.
Duration of MPH treatment from initiation to switch to ATX was measured as number of months between the initial MPH and initial ATX prescription. We did not consider MPH drug holidays (i.e., weekends and vacations during which patients may be off medication), as this was generally administered by the patient/and or family and, therefore, was rarely documented in individual patients' clinical notes or prescribing information.
We classified types of switching schedules into three categories inspired by previously defined approaches (Prasad and Steer 2008): 1) Immediate switching with no overlap between MPH and ATX, 2) cross tapering in which the dose of MPH was gradually reduced while the dose of ATX was gradually increased, and 3) gap switching with a treatment-free period between discontinuation of MPH and initiation of ATX. For patients switching by the cross-tapering schedule, we calculated the average number of overlapping weeks, whereas for patients switching by the gap-switching schedule, we calculated the average number of weeks between the two treatments.
Reasons identified in this study as the cause leading prescribers to switch patients from MPH to ATX were grouped into subcategories based on the information provided in individual patients' records. AEs (including exacerbation of psychiatric comorbidity) identified as the reason for switching therapy, were classified by System Organ Class (SOC) and Preferred Term (PT) level according to the Medical Dictionary for Regulatory Activities (MedDRA) (International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use 2014).
Definitions
For adverse events, we used the term AE, because no attempt was made in this study to assess whether or not a causal relationship was present between the observed event(s) and MPH. The European Union (EU) definition of an AE is “any untoward medical occurrence in a patient or clinical trial subject administered a medical product and which does not necessarily have a causal relationship with this treatment” (European Medicines Agency 2012).
Data extraction and analysis
The data were extracted and double-checked for accuracy by the first author (P.W., PhD Pharmaceutical Sciences), who also entered data into a data extraction form. Patient characteristics (gender, date of birth, ADHD subtypes, and psychiatric comorbidity), as well as details related to MPH and ATX treatment (e.g., start and stop date, initial formulation) were extracted directly from the EPR system. To identify and extract information about reasons leading prescribers to switch therapy from first-line MPH to second-line ATX, individual patients' clinical notes (in free-text form) were scrutinized from the first time a switch to ATX was mentioned until actual initiation of ATX and discontinuation of MPH.
Descriptive statistics were used to summarize overall patient and treatment characteristics (gender, age at time of MPH initiation, initial MPH formulation, and type of switching schedules), duration of MPH therapy to switch to ATX, clinical reasons leading prescribers to switch patients' therapy, and AEs observed in the study as reason for switching therapy. Differences in patient and treatment characteristics with respect to gender were tested using Fisher's Exact Test for categorical data and Mann–Whitney U test for continuous data. The α level for statistical significance was set at p < 0.05. Excel version 2010 and SAS 9.4 (SAS Institute Inc. 2013) were used to summarize and analyze data.
Results
Patient and treatment characteristics
Table 1 summarizes patient and treatment characteristics. Among the 55 switchers included in the study, 85.5% were male. Mean age at time of MPH initiation was 10.4 years (range = 7.3–17.7), with 85.5% of the patients initiating MPH treatment in the 7–12 year age range. There was a nonsignificant trend in gender patterns, with a larger share of girls than boys initiating treatment in the 7–9 year age group. Psychiatric comorbidity was frequent, with 65.5% of the patients being diagnosed with one or more comorbid psychiatric conditions; most common comorbid diagnoses were “developmental disorders” (e.g., speech and language disorders, learning disorders, autism, Aspergers syndrome, and pervasive developmental disorders not otherwise specified) (49.1%) and “behavioral and emotional disorders” (e.g., oppositional defiant disorder, conduct disorder, depression, anxiety, and tic disorder) (47.3%).
ATX, atomoxetine; MPH, methylphenidate.
More than half (60.0%) of the patients initiated MPH treatment with an immediate-release formulation, versus 40% initiating treatment with a modified-release formulation. Patients were most commonly switched to ATX by gap switching (52.7%) followed by cross-tapering (38.2%) and immediate switching (9.1%). Patients being switched by the gap switching schedule on average initiated ATX 9.3 weeks after discontinuing MPH. For patients being switched by the cross-tapering schedule, MPH and ATX on average overlapped with 14.0 weeks (data not shown). On stratification by gender, we found no significant differences between female and male patients with respect to the patient and treatment characteristics summarized in Table 1.
Duration of MPH treatment to switch to ATX
Overall, patients were switched to ATX at an average of 11.2 months (range = 0.3–28.5) after initiation of MPH treatment. Analyses stratified by gender showed no significant difference between females and males with respect to mean duration of MPH treatment prior to switch (Table 1). As shown in Figure 2, 36.4% of the patients were switched to ATX within 6 months, 56.4% within 1 year, and 76.4% within 1.5 years of initiation of MPH treatment. The remaining 23.6% continued MPH treatment for up to 2.5 years prior to being switched to ATX.

Cumulative distribution (%) of patients switching therapy, by time from initiation of methylphenidate to switch to atomoxetine (n = 55).
Reasons for therapy switching
The distribution of reasons for switching therapy from first-line MPH to second-line ATX are displayed in Figure 3. We identified a total of 74 reasons (grouped into five general categories), corresponding to an average of 1.3 reasons per patient. Overall, the single most frequently cited reason for switching therapy was “AEs” (78.2%) followed by “wish for more optimal day coverage” (23.6%), “lack of efficacy” (16.4%), and “patient/parental request” (12.7%). “Noncompliance” was identified as reason for therapy switching in only 1.8% of the patients, although many more patients (exact number not extracted) were described as noncompliant with respect to their prescribed dosing regimens.
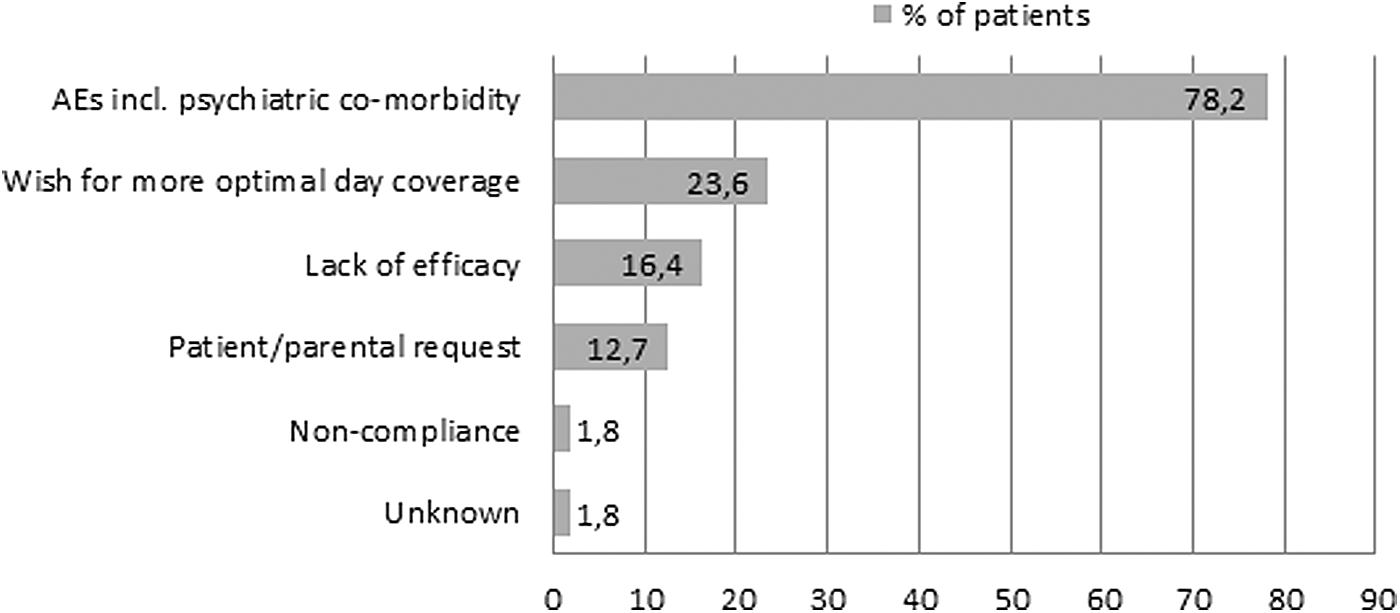
Distribution (%) of reasons for switching therapy from first-line methylphenidate to second-line atomoxetine in the study population (n = 55).
Table 2 summarizes AEs identified in the study as reason for switching therapy. Among the 55 switchers included in the study, 43 (78.2%) were switched because of AEs. We identified a total of 95 AEs, corresponding to an average of 2.2 AEs per patient. The SOC most commonly associated with AEs was “psychiatric disorders,” accounting for 64.2% of all observed AEs. Within this SOC, insomnia was the most frequent AE, corresponding to 14.8% of all AEs classified as psychiatric disorders followed by aggression (13.1%), tic (11.5%), depression (9.8%), and anxiety (8.2%). Other AEs classified as psychiatric disorders that also deserve to be highlighted, although not cited as frequently as the abovementioned AEs, include two cases of suicidal attempt and two cases of suicidal ideation. “Decreased appetite” under the SOC “metabolism and nutritional disorders,” was the most frequent single AE, accounting for 14.7% of all AEs leading to a switch in therapy.
43 patients in the study population (n = 55) switched therapy because of AEs.
Multiple responses possible.
Calculated as proportion of AEs in the group of patients switching therapy because of AEs (n = 43).
AE, adverse event; ATX, atomoxetine; MPH, methylphenidate.
Discussion
In this study, we examined switching from MPH to ATX in the pharmacological treatment of childhood and adolescent ADHD. More specifically, we determined the duration of MPH treatment prior to switch to ATX, and the underlying reasons leading prescribers to switch therapy. Our study is unique, in that it is among the first examining these topics, and it distinguishes itself by being based on systematic review of patient records throughout a predetermined time period. The main findings of the present study were a relatively long average length of time from initiation of MPH to transition to ATX, and the predominant role of AEs as reason for switching.
Of the 55 children and adolescents included in this study, 36.4% were switched to ATX within the first 6 months of initiating MPH. We note, however, that the mean duration of MPH treatment until switch to ATX was almost a year (11.2 months), which is long considering that 78.2% of the patients were switched as a direct result of AEs (including psychiatric comorbidity). Plausible explanations for this relatively long MPH mean duration obviously include the likelihood that some patients may have switched from immediate-release to modified-release MPH prior to switching to ATX, as well as the fact that more than half of the patients in this study were switched by a gap switching schedule; that is, with a treatment-free period between discontinuation of MPH and initiation of ATX. Other factors are also likely to have contributed to the long MPH mean duration. Some of the psychiatric comorbidity AEs may only have developed after a sustained period of MPH treatment. Also, decisions about switching therapy in the current study were rarely made by the patient, but rather by parents and prescribers. Although parents and prescribers may be concerned about AEs, they might be tolerant of these in favor of the perceived positive effects of MPH in reducing the symptoms of ADHD (dosReis and Myers 2008). Additionally, parents may feel pressured by schools or healthcare providers to keep their children on MPH despite occurrence of intolerable AEs (Brinkman et al. 2009). Finally, parents and prescribers may be reluctant to initiate ATX because of a number of very rare but severe AEs mentioned in the product labelling, including suicide-related behavior, sudden death in patients with preexisting structural cardiac abnormalities, and hepatic effects (Medicines and Healthcare Products Regulatory Agency 2015).
Based on information provided in individual patients' clinical notes, we found that AEs were by far the most frequently cited reason leading prescribers to switch patients' therapy followed by “wish for more optimal day coverage” and “lack of efficacy.” Less frequently cited reasons included “patient and/or parental request” and “noncompliance.” Although these findings suggest that particular attention should be given to AEs when evaluating MPH treatment outcome and need for therapy switch, it should be highlighted that the number of AEs identified in this study is likely to be biased by “exacerbation of psychiatric comorbidity” combined with a high occurrence of preexisting psychiatric comorbidity. These factors may explain the frequent occurrence of psychiatric AEs in this study (e.g., insomnia, aggression, tic, depression, and anxiety). It must be mentioned however, that psychiatric AEs are “very common” or “common” according to MPH product labelling (Medicines and Healthcare Products Regulatory Agency 2013) and have also been cited in previous studies as important factors in parents' decision to discontinue their child's ADHD medication (Toomey et al. 2012; Gajria et al. 2014). It is also important to consider that MPH may cause psychiatric AEs in patients without preexisting psychiatric comorbidity (Wigal 2009). With this is mind, the findings of our study highlight the importance of paying attention to new, as well as to exacerbation of already existing, psychiatric comorbidity when evaluating potential AEs associated with MPH treatment. Evidently, in cases of exacerbation of already existing psychiatric comorbidity (e.g., depression and anxiety), one should also consider the potential lack of efficacy of other psychotropic medication taken by the patient.
MPH is generally considered efficacious in the treatment of childhood and adolescent ADHD, with a therapeutic response rate of >75% (Wigal 2009). Nevertheless, “lack of efficacy” and “wish for more optimal day coverage” are important reasons for switching therapy in the present study. It is possible that shift from one formulation of MPH to another, such as that from an immediate-release to a prolonged-release formulation, would have rendered a shift to ATX unnecessary in some patients. However, the issue of shift in formulation of MPH was beyond the scope of the present study. “Noncompliance” was found to play a less prominent role in the decision to switch patients' therapy, which is surprising, when taking into consideration that the clinical notes reviewed revealed that many more patients were noncompliant with respect to their prescribed regimen. Although there are no obvious explanations for this, we acknowledge that noncompliance should be considered an important factor for switching patients from MPH to ATX, as noncompliance leads to reduction in the overall effectiveness of the treatment (Hack and Chow 2001). Also, unlike MPH requiring multiple doses per day, ATX can be administered as a single daily dose, thereby increasing the chances of compliance (Prasad and Steer 2008).
Although this study did not attempt to describe switching patterns after the switch to ATX (some patients switching from MPH to ATX may later be switched back to MPH or discontinue treatment all together), there is evidence that a switch from MPH to ATX may prove successful in some patients. A single-arm, open-label study by Quintana et al. evaluating the transition to ATX in 62 subjects somewhat intolerant of or partially nonresponsive to their stimulant therapy (52% MPH, 48% amphetamines), found that 53% of the patients chose to switch to ATX as a result of inadequate response, whereas 47% switched because of intolerance. Following the switch, symptoms improved significantly, with particular benefits seen early during the transition period (Quintana et al. 2007). A double-blind placebo-controlled study by Newcorn et al., comparing the effect of ATX, MPH, and placebo in 516 patients with ADHD, found that out of 70 patients who did not respond to MPH, 30 (43%) subsequently responded to ATX (Newcorn et al. 2008).
The strengths of the present analysis lie in the fact that data were derived from patient records, which, unlike data collected during controlled clinical trials, reflect “real-world” clinical practice. Further, patient records contain clinical information recorded in free-text form at the time of consultation (Warrer et al. 2012, 2015), which allowed us to extract valuable information about reasons for switching therapy. Finally, our study was based on patient records' data deriving from a clearly defined study population (i.e., children and adolescents switching from first-line MPH to second-line ATX), which increases the external validity of our findings. However, the present study is subject to a number of limitations. Firstly, we did not include a non-switcher comparator group and, therefore, were not able to make comparisons across switcher- and non-switcher groups with respect to patient and clinical characteristics (e.g., age, gender, psychiatric comorbidity). Second, because of the unavailability of data in electronic form prior to January 01, 2012, our study population was restricted to patients initiating MPH and switching to ATX within the period from January 1, 2012 to May 15, 2014, resulting in a study population of 55 patients. Finally, our calculation of MPH mean duration until switch to ATX is based on a subpopulation of therapy switchers initiating first-line MPH during the observation period. Hence, the mean MPH duration reported in this study is biased, because maximum MPH duration until switch depends upon when MPH was first prescribed. This is likely to have resulted in too short an estimate of MPH mean duration until switch.
Finally, the rather liberal definition of therapy switching employed in this study (switching from first-line MPH to second-line ATX), did not specify the length of required follow-up, possibly resulting in a biased estimation of the mean length of MPH prior to switching to ATX.
Conclusions
Assuming, in line with previous studies (Ben Amor et al. 2014; Childress and Sallee 2014; Gajria et al. 2014), that therapy switching is associated with suboptimal treatment outcome of the index therapy, we believe that our findings will lead to increased awareness about factors that may potentially help prescribers identify patients who would benefit from a switch in therapy. Additional studies, exploring larger study populations and employing different methodological approaches, are needed to replicate and confirm our findings. Ideally, future studies should also investigate the outcome of switching from MPH to ATX, to understand if a switch in therapy is successful in terms of efficacy and/or AE resolution.
Clinical Significance
The findings of this study highlight the importance of continuous evaluation of the treatment outcome and need for therapy switch to ATX in children and adolescents treated with MPH. Factors to take into consideration include intolerable AEs (in particular psychiatric AEs), nonoptimal day coverage, lack of efficacy, patient/parental preferences, and noncompliance. Importantly, these factors should be considered not only at the initial stages of MPH treatment but also throughout the whole MPH treatment course. Our findings may potentially help prescribers identify patients, who would benefit from a switch from MPH to ATX, more efficiently.
Disclosures
No competing financial interests exist.