
Abstract
Objective:
Perturbations in emotional conflict adaptation, an implicit regulatory process, have been observed in adult anxiety disorders. However, findings remain inconsistent and restricted to adults. The current study compares conflict adaptation in youth and adults, with and without anxiety disorders. We predicted conflict adaptation would be present in the healthy but not the anxious groups.
Methods:
In a clinic setting, 111 participants (27 healthy youth, 22 anxious youth, 41 healthy adults, and 21 anxious adults) completed emotional and nonemotional conflict tasks. Groups did not differ (all p's >0.1) on intelligence quotient (IQ), gender, and socioeconomic status; age did not differ between healthy and anxious subjects in either age cohort. Separate four way mixed-design analyses of variance were conducted to test hypotheses regarding the influence of diagnosis, age group, and task type on accuracy (percent correct) and reaction time (RT) for conflict adaptation (incongruent trials preceded by incongruent vs. congruent trials) and conflict detection (incongruent vs. congruent trials).
Results:
Measures of conflict adaptation did not interact with diagnosis or age. There was a significant main effect of conflict adaptation across the overall sample in the expected direction for accuracy, but not RT. The well-replicated conflict detection effect also did emerge across tasks, with slower RT and lower accuracy for incongruent than for congruent trials. These effects were greater for the emotional than for nonemotional tasks. Finally, there were age differences in accuracy-based conflict detection specific to the emotional task, for which the size of the effect was larger for youth than for adults.
Conclusions:
The current study of youth and adults did not replicate prior behavioral findings of failure to engage conflict adaptation in anxiety disorders. Therefore, more work is needed before widely adopting conflict adaptation paradigms as a standard neurocognitive marker for anxiety disorders.
Introduction
I
This particular task generates separate measures of conflict detection and adaptation, which represent two forms of cognitive control. In this paradigm (Etkin et al. 2006), participants must identify the emotional expression of a face while ignoring an overlaid emotion word. The face–word pairs are either semantically incongruent (e.g., fearful face superimposed with the word “happy”) or congruent (e.g., fearful face superimposed with the word “fearful”). Conflict is generated by competing response options in the incongruent condition. Because of the need to inhibit prepotent responses to the task-irrelevant words, “high-conflict” incongruent trials are associated with RT slowing compared with “low-conflict” congruent trials (Stroop 1935; MacLeod 1991; Botvinick et al. 2001). Normative developmental studies show that children, by the age when reading is established, tend to show robust RT interference generated by conflict on Stroop tasks (MacLeod 1991). The detection of conflict is proposed to activate regulatory processing, referred to as conflict adaptation, which mitigates RT interference on subsequent “high-conflict” incongruent trials (Gratton et al. 1992; Botvinick et al. 2001). Specifically, conflict detection is indexed by slower RT on incongruent relative to congruent trials, whereas conflict adaptation is indexed by reduced RT slowing on incongruent trials that follow incongruent trials, but not incongruent trials that follow congruent trials.
Using this paradigm, Etkin et al. (2010) reported that adult patients with generalized anxiety disorder (GAD) differed from healthy adults for measures of emotional conflict adaptation. Nevertheless, more work is needed, because findings using this and related emotional conflict paradigms appear inconsistent (Chechko et al. 2009; Krug and Carter 2010; Jarcho et al. 2013). In contrast to Etkin et al.'s findings with emotional conflict adaptation, behavioral performance during nonemotional conflict adaptation in other studies did not differ as a function of GAD diagnosis (Larson et al. 2013) or trait anxiety (Osinsky et al. 2010). These findings suggest that perturbations in conflict adaptation may be specific to emotional conflict. Although Egner et al. (2008) reported similar behavioral conflict adaptation across emotional and nonemotional conflict tasks in healthy adults, no study to date has directly compared emotional versus nonemotional conflict tasks in patients with anxiety disorders.
Moreover, as noted, some findings on cognitive processing in anxiety are opposite from those of Etkin and colleagues. Specifically, a psychophysiological measure, ERN, is enhanced in anxious compared with nonanxious subjects in both pediatric and adult studies, with consistent results emerging across research groups (Yeung et al. 2004; van Noordt and Segalowitz 2012; Moser et al. 2013). Although increased post-error slowing, a behavioral index of cognitive control, has been shown in anxious children (Meyer et al. 2012), the ERN is not typically associated with anxiety in behavioral differences such as error rates or post-error slowing across studies (Hajcak and Simons 2002; Ladouceur et al. 2006; Hajcak et al. 2008; Santesso et al. 2010; Carrasco et al. 2013; Lahat et al. 2014). Therefore, there is a need for more research on cognitive control in anxiety phenotypes, particularly in youth. Attempting to resolve this discrepancy of cognitive control perturbations across development may elucidate paths through which anxiety disorders in adolescence increase risk for adult disorders (Pine et al. 1998; Pine 2007).
Conflict adaptation has not yet been studied in youth anxiety disorders. To address this need, we used the same emotional and nonemotional conflict tasks as in prior studies (Etkin et al. 2006; Egner et al. 2008; Etkin et al. 2010; Etkin and Schatzberg 2011; Jarcho et al. 2013, 2014) and compared conflict detection and adaptation in youth and adults, with and without anxiety disorders. Prior studies comparing anxious and nonanxious individuals in other affective processing domains, such as threat learning and respiratory challenge, suggest shared features in pediatric and adult disorders (Pine et al. 2000; Britton et al. 2013). Therefore, we expect anxiety diagnosis to influence conflict detection and adaptation similarly in youth and adults. Specifically, we hypothesized that emotional conflict adaptation occurs in both healthy groups but in neither anxious group, whereas we predicted nonemotional conflict adaptation would not differ between the healthy and anxious groups. We predicted no age differences in conflict adaptation, given that children and adults showed similar conflict adaptation on a nonemotional task (Larson et al. 2012). We also predicted greater conflict detection effects in the anxious than in the healthy participants, based on prior studies (Chechko et al. 2009; Berggren and Derakshan 2014).
Methods
Participants
A total of 121 participants (59 youth and 62 adults) were recruited from the community via local advertisements, and completed this study in the clinic as paid volunteers. As part of an existing, larger study, participants completed a series of research visits, which were followed by a course of treatment with either cognitive behavioral therapy or medication for the youth patients only. Adult participants and parents of youth participants provided written informed consent, and youth participants provided written informed assent. All study procedures were approved by the National Institute of Mental Health Institutional Review Board.
Exclusion criteria for all groups included intelligence quotient (IQ) <70, current psychotropic medication use, or physical health problems, or siblings enrolled in the study. The age range for adults was 18–40 years. All participants underwent a comprehensive psychiatric assessment via the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (Kaufman et al. 1997) for youth, and the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) Axis I Disorders (First et al. 1995; American Psychiatric Association 2000) for adults. Anxious youth met DSM-IV-TR criteria for current primary diagnosis of GAD, social phobia, or separation anxiety disorder. Anxious patients were permitted to have additional anxiety disorders with the exception of obsessive-compulsive disorder and posttraumatic stress disorder, which were exclusionary. Inclusion criteria for the healthy volunteer groups included the absence of current Axis I disorders.
The following exclusions were applied: Five participants (four anxious youth, one healthy youth) aborted the task, three anxious youth with <60% overall accuracy on the task trials, and two participants (one healthy youth and one anxious youth) for whom there were technical issues during the task. This resulted in a final sample of 111 participants (49 youth and 62 adults). Demographic and clinical assessment information is presented in Table 1. Anxious and healthy participants did not significantly differ within each age group based on age, gender, IQ, or socioeconomic status (SES). Within each age group, the anxious groups showed significantly greater symptoms than the age-matched healthy comparison groups.
Data reported as mean (SD) unless otherwise specified.
Significant diagnosis group difference within each age group, p < 0.01.
ADHD, attention-deficit/hyperactivity disorder; BDI, Beck Depression Inventory (Beck et al. 1996); CDI, Child Depression Inventory (Kovacs 1985); GAD, generalized anxiety disorder; IQ, intelligence quotient; LSAS, Leibowitz Social Anxiety Scale (Fresco et al. 2001); ODD, oppositional defiant disorder; SAD, separation anxiety disorder; SCARED, Screen for Child Anxiety Related Emotional Disorders (Birmaher et al. 1997); SES, socioeconomic status; STAI, Spielberger State-Trait Anxiety Inventory (Spielberger 1983).
Experimental paradigms
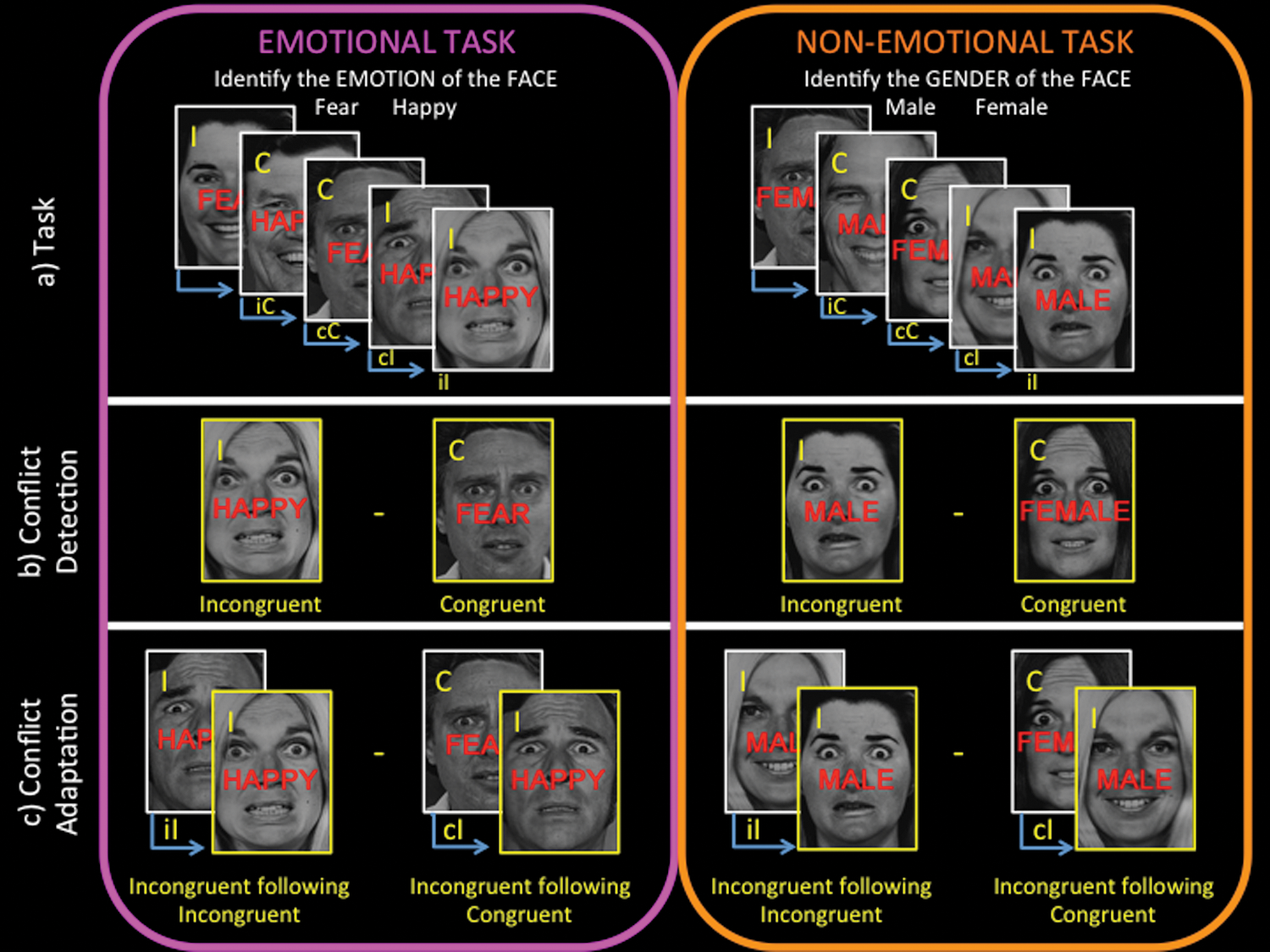
In the clinic, participants were presented with black and white photographs of males and females with happy or fearful facial expressions (Ekman and Friesen 1976) in two emotional and nonemotional conflict tasks, which have been published in prior studies (Etkin et al. 2006; Egner et al. 2008; Etkin et al. 2010; Etkin and Schatzberg 2011; Jarcho et al. 2013, 2014). The faces were overlaid with the words “FEAR” or “HAPPY” in the emotional conflict task and “MALE” or “FEMALE” in the nonemotional conflict task. Participants were instructed to ignore the words and identify the emotional expression (emotional task, fear or happy) or gender (nonemotional task, male or female) of the face via button press as quickly and accurately as possible (Fig. 1). The faces represented task-relevant stimuli and were identical across both conflict tasks. The words served as prepotent task-irrelevant stimuli that were either emotional or nonemotional, depending upon the task condition. Task-irrelevant stimuli generated conflict on semantically incongruent trials, in which the words and the faces did not match (e.g., fearful face overlaid with the word “HAPPY” on the emotional task; female face overlaid with the word “MALE” on the nonemotional task). Half of the trials for each task were incongruent and the other half were congruent (i.e., the expression/gender of the face matched the word; Fig. 1b).
Conflict adaptation task.
Participants completed practice trials (24 trials per run) of the emotional and nonemotional conflict tasks. All participants completed at least one practice run, and training stopped when proficiency (defined as 90% accuracy within a run) was demonstrated or when they completed three runs, whichever came first.
The order of the tasks was counterbalanced across participants. The stimulus presentation sequence was the same as in prior studies using the emotional and nonemotional conflict tasks (Etkin et al. 2006; Egner et al. 2008; Etkin et al. 2010; Etkin and Schatzberg 2011; Jarcho et al. 2013, 2014). The gender, identity, and emotion of the photograph and overlaid word were counterbalanced across trial type, and stimuli were shown in a pseudorandom order for 1000 ms duration, with an interstimulus interval of 3000–5000 ms (EPrime; Sharpsburg, PA). Stimuli were presented in four blocks of 37 trials (148 trials) for each task, and blocks were separated by 8 sec rest periods. To help reduce the potential confounds of negative priming or repetition priming effects (Mayr et al. 2003), there were no direct repetitions of identity (i.e., photographs of the same person) or expression–word combinations (e.g., fearful expression overlaid with the word FEAR), as in prior studies using this paradigm (Etkin et al. 2006; Egner et al. 2008; Etkin et al. 2010; Etkin and Schatzberg 2011; Jarcho et al. 2013, 2014).
Analyses (described subsequently) were conducted separately for RT and accuracy rate (percent correct). Consistent with the prior studies using these conflict tasks, RT measures excluded error trials, post-error trials, and trials with outlier values of more than 2 SDs from the mean for each trial type, within each block. After applying these exclusions, we also excluded trials with RT <200 ms from both RT and accuracy measures to remove trials that did not reflect a physiologically valid response (which occurred only for one trial for three participants and two trials for one participant).
Statistical analyses
For the conflict adaptation analyses, trials were classified based on both the current trial type (congruent [C] or incongruent [I]) and the preceding trial type (congruent [c] or incongruent [i]). Conflict adaptation was tested by comparing the incongruent trials preceded by incongruent (iI) trials versus the incongruent trials preceded by congruent (cI) trials. Conflict detection was assessed by comparing performance on the congruent versus incongruent conditions, which were classified based solely on current trial type.
Separate four way mixed-design analyses of variance (ANOVAs) were conducted to test hypotheses regarding conflict adaptation and conflict detection for each dependent measure (reaction time and accuracy), on both emotional and nonemotional tasks, resulting in a total of four ANOVAs (α = 0.05). All models included two between-subject measures (age – youth, adult; and diagnosis – healthy, anxious) and repeated measures for task (emotional task, nonemotional task) and conflict adaptation/detection. The ANOVAs testing conflict adaptation (Fig. 1c) included a repeated measure for incongruent trials as a function of preceding trial type (i.e., iI and cI conditions), whereas the ANOVAs testing conflict detection (Fig. 1b) included a repeated measure for congruency (i.e., I and C conditions). For the conflict adaptation ANOVAs, only F tests involving the conflict adaptation factor (iI vs. cI) are presented; the results for the other factors (age, diagnosis, task, and their interactions) are presented with the results from the conflict detection ANOVAs to avoid repetition because these factors were similarly included in both models. In the case of significant interactions, post-hoc pairwise comparisons were conducted using Bonferroni correction. Estimated marginal means and mean differences are reported for significant main effects and interactions, respectively. Follow-up correlational analyses of the RT and accuracy measures were conducted to assess whether there was an accuracy–speed tradeoff. Given that RT data are often not normally distributed, we conducted Kolmogorov–Smirnov normality tests on the standardized residuals for each cell from the conflict adaptation and conflict detection models, separately. To address cells showing non-normality, we performed multiple transformations (i.e., log and square root transformations), which were unsuccessful in establishing normal distribution of the residuals from the ANOVA models. We then reran the RT ANOVAs after excluding subjects who were outliers (> 2.5 SD above or below the mean) on any RT measure (n = 5; 1 healthy adult, 1 anxious youth, 3 healthy youth). This manipulation left unchanged the main study effects involving diagnosis. Based on these results and the fact that parametric analyses are frequently conducted on untransformed RT data, we report all results including the tables and figures using the original untransformed data. Finally, bivariate Pearson correlations were conducted in youth and adults separately to examine associations of dimensional anxiety symptom scores with conflict adaptation and conflict detection difference scores (see Supplementary Table 1) (see online supplementary material at
Results
All ANOVA results are presented in Table 2.
Reaction time data reported in milliseconds as mean (SD).
cC, congruent following congruent; cI, incongruent following congruent; iC, congruent following incongruent; iI, incongruent following incongruent.
Conflict adaptation
RT
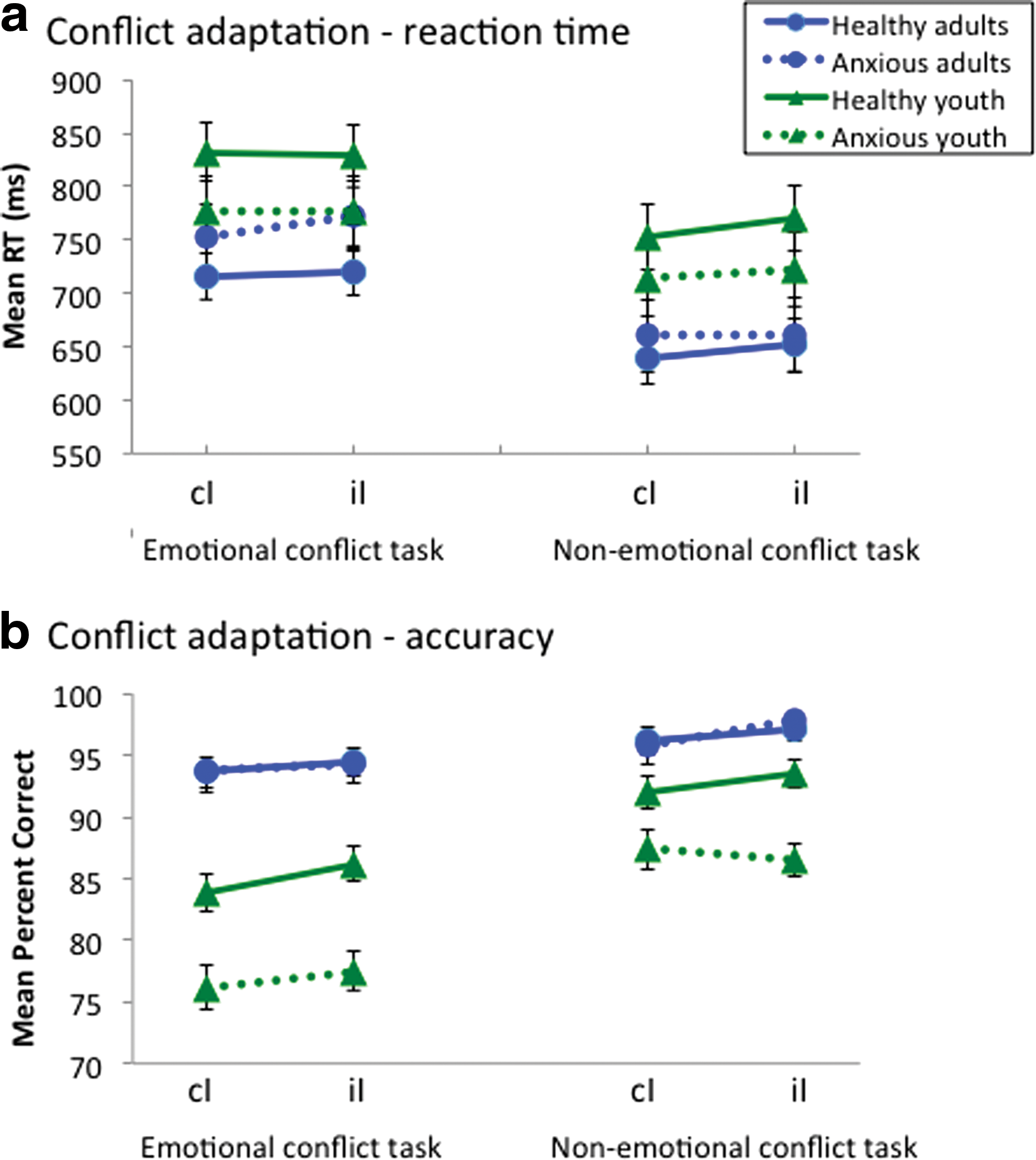
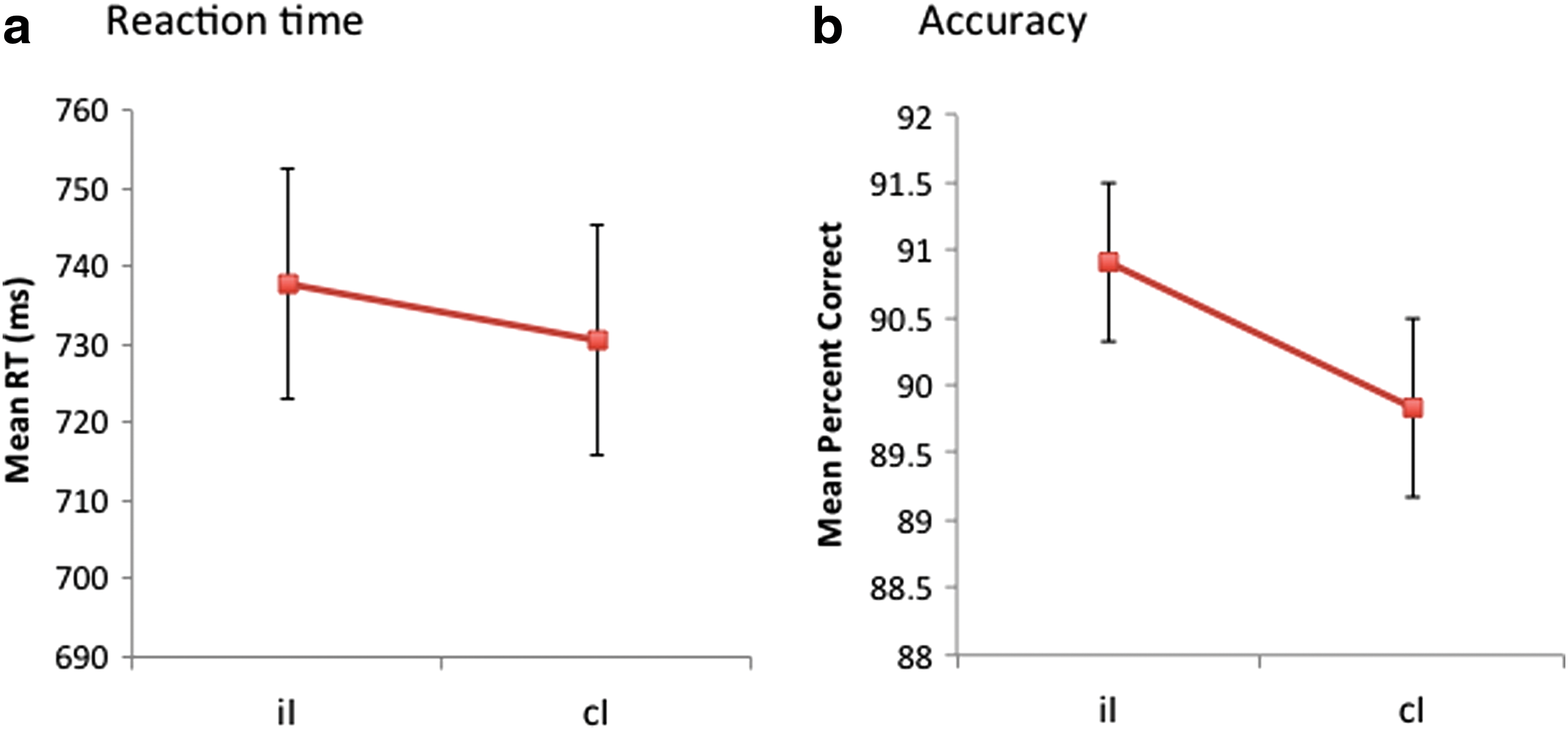
Descriptive statistics for RT by trial type, task, and group are reported in Table 2. There were no significant interactions for conflict adaptation with task, age, and/or diagnosis for reaction time, all p values >0.14 (Fig. 2a, Table 3ai). There was no significant main effect of conflict adaptation, F(1,107) = 3.22, p = 0.08 (Fig. 3a). Moreover, although nonsignificant, the iI versus cI comparison was in the unpredicted direction, with overall slower RT for iI compared with cI trials. Upon rerunning the RT ANOVAs after excluding five outlier subjects, there were still no significant associations with diagnosis (i.e., all main effects and interactions with diagnosis, all p's >0.1). The same was true for conflict detection analyses described subsequently.
Conflict adaptation by group and task.
Main effect of conflict adaptation.
C, congruent; I, incongruent; iI, incongruent following incongruent; cI, incongruent following congruent.
Accuracy
There were no significant interactions for conflict adaptation with task, age, and/or diagnosis for accuracy, all p values >0.13 (Fig. 2b, Table 3aii). The significant main effect of conflict adaptation for accuracy was in the expected direction, F(1,107) = 54.38, p < 0.001. As predicted, accuracy was higher for the iI than for the cI trials (Fig. 3b).
Speed–accuracy tradeoff
Given that the iI minus cI differences for accuracy and RT were in the opposite direction, we conducted follow-up correlational analyses to test whether there was a speed–accuracy tradeoff that might account for the observed pattern of results (i.e., slower RT associated with higher accuracy). Correlations based on the iI minus cI difference scores for RT and accuracy were nonsignificant for both tasks (emotional task: r = 0.003, p = 0.97; nonemotional task: r = 0.10, p = 0.31). However, overall mean RT and accuracy (i.e., across all trials, iI, cI, iC, cC) were negatively correlated for the emotional task (r = −0.32, p = 0.001) and the nonemotional task (r = - 0.34, p < 0.001). Regardless, these significant correlations still were not consistent with a speed–accuracy tradeoff, because they showed that faster reaction time was associated with higher accuracy for each task. A speed–accuracy tradeoff would manifest with slower reaction time for higher accuracy.
Conflict detection
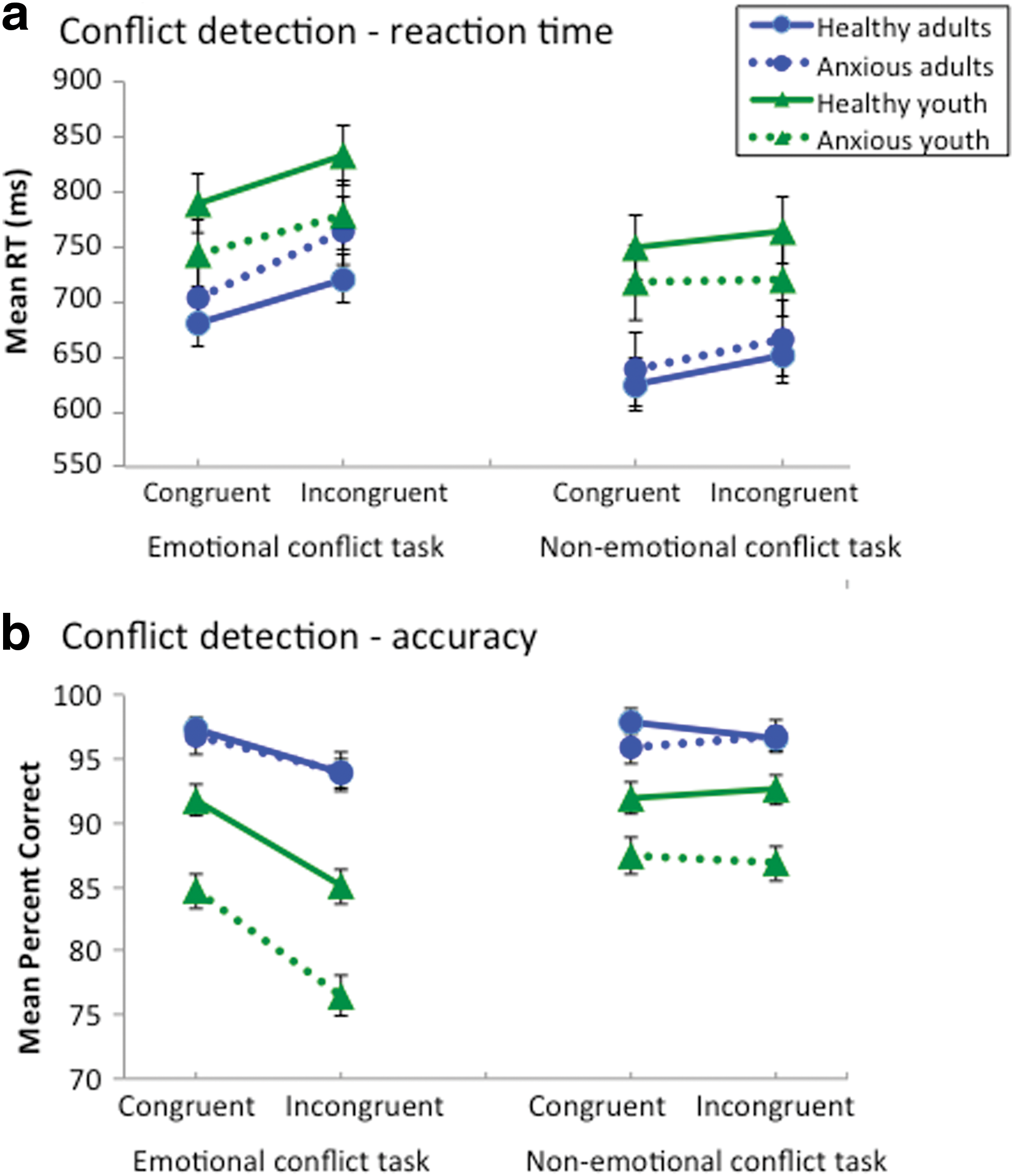
The estimated marginal means from the conflict detection ANOVAs are presented in Figure 4.
Conflict detection by group and task.
RT
There were no significant interactions involving diagnosis on RT. There was a significant interaction of congruency and task, in which there was a greater mean difference of incongruent versus congruent trials for the emotional task (mean difference = 45.21 ms, SE = 4.29, corrected p < 0.001) than for the nonemotional task (mean difference = 18.00 ms, SE = 4.16, corrected p < 0.001; Fig. 5a). There was also an interaction of congruency and age, such that the mean difference for incongruent versus congruent trials was lesser for the youth (mean difference = 24.29 ms, SE = 5.10, corrected p < 0.001) than for the adults (mean difference = 38.91 ms, SE = 4.76, corrected p < 0.001). Finally, there were significant main effects of congruency, task, and age on RT. Overall, RT was slower for incongruent (mean = 737.78 ms, SE = 14.68) versus congruent trials (mean = 706.18 ms, SE = 14.40), emotional task (mean =752.28 ms, SE = 13.96) versus nonemotional task trials (mean =691.68 ms, SE = 15.82), and youth (mean = 762.46 ms, SE = 21.10) versus adults (mean = 681.50 ms, SE = 19.71).
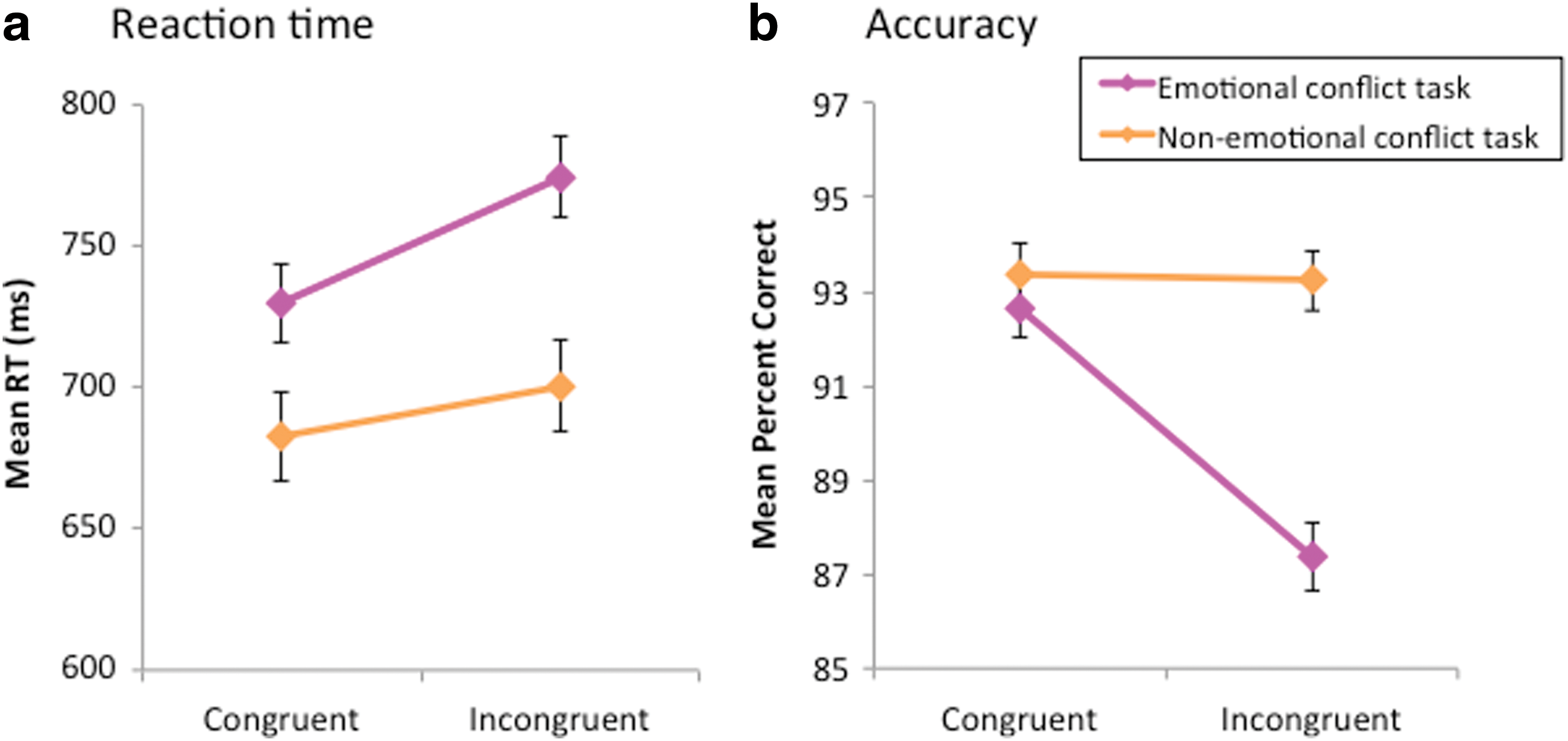
Task by conflict detection interaction.
Accuracy
There was a significant three way interaction of congruency, task, and age on accuracy (percent correct), in which the interaction of congruency and age differed by task (Fig. 4b). For the emotional task, both adults and youth showed significantly lower accuracy for incongruent compared with congruent trials, but the mean difference of incongruent versus congruent trials was larger for youth (mean difference = −7.50, SE = 0.77, corrected p < 0.001) than for adults (mean difference = −3.07, SE = 0.72, corrected p < 0.001). For the nonemotional task, both adults and youth again showed significantly lower accuracy for incongruent than for congruent trials; however, the mean differences of incongruent versus congruent trials were similar for youth (mean difference = 0.06, SE = 0.75, corrected p = 0.94) and adults (mean difference = −0.28, SE = 0.70, corrected p = 0.69).
The following two way interactions were significant and are subsumed under the three way interaction of congruency, task, and age: Congruency-by-task, congruency-by-age, and task-by-age interactions. There was also an age-by-diagnosis interaction, in which anxious youth exhibited lower accuracy than healthy youth (mean difference = −6.50, SE = 1.59, corrected p < 0.001), but there was no diagnostic group difference among adults (mean difference = −0.54, SE = 1.49, corrected p = 0.72).
Finally, all main effects were significant. Participants demonstrated overall lower accuracy for incongruent (mean = 90.30, SE = 0.59) than for congruent trials (mean = 92.99, SE = 0.56), as well as lower accuracy for the emotional task (mean = 90.00, SE = 0.62) than for the nonemotional task trials (mean = 93.29, SE = 0.60). Youth showed overall lower accuracy (mean = 87.12, SE = 0.80) than adults (mean = 96.18, SE = 0.74), and the same pattern emerged for anxious (mean = 89.89, SE = 0.85) compared with healthy groups (mean = 93.41, SE = 0.69).
Discussion
In the clinic setting, we examined behavioral conflict adaptation in adults and youth with and without anxiety disorders and observed four main results. First, conflict adaptation was not modulated by diagnosis, age, or emotional versus nonemotional tasks. We failed to replicate differences in emotional conflict adaptation between healthy and anxious individuals (Etkin et al. 2010). Second, robust conflict detection, or interference effects occurred across both emotional and nonemotional tasks; this demonstrated appropriate engagement in the paradigm by the subjects in our sample, with slower RT and lower accuracy for incongruent than for congruent trials as expected. This effect was greater for the emotional task than for the nonemotional task. Third, overall slower RT and lower accuracy were observed for the emotional than for the nonemotional conflict tasks. Finally, there were age differences in conflict detection for accuracy on the emotional task, but not the nonemotional task. Both age groups showed a significant congruency effect on the emotional task, but the size of this effect was larger for youth than for adults.
Although we used the same paradigm and analytic approach, we did not replicate anxiety-related behavioral differences reported by Etkin et al. (2010) and others (Chechko et al. 2009). Importantly, anxiety-related differences in emotional conflict adaptation were predicated on the presence of RT-based conflict adaptation in the healthy group, which we also failed to observe. We conducted a post-hoc power analysis (Faul et al. 2009) of the two key statistical tests, using effect size estimates based on findings in Etkin et al. (2010) (α = 0.05). First, the between-group difference in Etkin et al. (2010) comparing conflict adaptation (iI-cI) difference score for anxious adults versus healthy adults manifested with a large effect size (d = 0.8). Second, the within-group effect for healthy adults manifested with a medium effect size (d = 0.45). For our study, post-hoc power analysis revealed 0.83 power for observing RT-based conflict adaptation in the healthy adults and 0.88 power for a two-sample t test comparing anxious and healthy adults. Thus, power was adequate in the current study to replicate the adult findings from Etkin et al. (2010). Our failure to replicate these findings suggests the absence of large-effect-size differences in RT within the task. Moreover, using the same one-sample t test analysis for incongruent trials reported by Etkin et al. (2010), post-hoc analyses in the healthy adults (not reported) showed no conflict adaptation on RT for the emotional task, and the opposite effect of slower RT to iI versus cI trials for the nonemotional task, t(40) = 2.51, p = 0.016. Our healthy adult group was relatively large (n = 41), compared with prior studies (Etkin et al. 2006; Egner et al. 2008; Etkin et al. 2010). Similarly, post hoc two sample t tests showed no differences in emotional conflict adaptation between anxious and healthy adults for either RT, t(60) = −1.26, p = 0.21, or for accuracy, t(60) = 0.57, p = 0.57.
The current study failed to show impaired RT-based conflict adaptation in anxiety disorders. In contrast to the behavioral results by Etkin and colleagues (2010) revealing reduced cognitive control (indexed by RT-based conflict adaptation) in anxiety, studies of event-related brain potentials demonstrate enhanced ERN in anxiety. ERN is an event-related brain potential that reflects a neural response following performance errors, and is studied using well-established paradigms of cognitive control. For cognitive measures to show clinical relevance, it is important to demonstrate replicability of findings across studies and laboratories. ERN may be better suited than the emotional conflict adaptation task to clinical applications, given that findings replicate across research groups with ERN, but not this task. Although ERN, a brain-based measure, is typically increased in anxiety, such findings are generally not associated with differences in behavioral performance measures indexing cognitive control, such as post-error reaction time slowing or decreased accuracy (van Noordt and Segalowitz 2012; Moser et al. 2013). This raises issues about “brain-based” differences, which may replicate, versus only “behavior-based” differences, which fail to replicate in the current study or in Moser et al.'s (2013) meta-analysis, emphasizing the neeed to examine both brain and behavior in translational affective neuroscience studies.
The present study, which included both an emotional and a nonemotional version of the same task, allows us to address whether cognitive control impairments in anxiety disorders are specific to emotional versus nonemotional tasks. Unlike Egner and colleagues (2008), who reported RT-based conflict adaptation for both tasks in a sample of healthy adults, we did not see faster RT for iI versus cI trials in the healthy adult group, or in the overall sample, for either task. However, as in Egner et al. (2008), we showed overall slower RT for the emotional than for the nonemotional tasks, suggesting that the emotional (vs. nonemotional) coding increases the difficulty of the task. Additional research in anxious patients is needed to test whether cognitive control perturbations in anxiety vary as a function of the emotional versus nonemotional sources of conflict. Paradigms such as the face-word Stroop task (Etkin et al. 2006; Egner et al. 2008) and the Eriksen flanker task (Ochsner et al. 2009; Alguacil et al. 2013; Liu et al. 2013) have been studied using matched-task versions that compare emotional versus nonemotional forms of cognitive control, and are, therefore, well suited to test this hypothesis. Attempts to replicate anxiety-related differences in cognitive control should simultaneously examine measures of conflict adaptation, post-error slowing/accuracy, and ERN, to explore how robust the phenomena are and, whenever possible, directly compare emotional and nonemotional tasks to test for affect-based specificity.
Although the classic conflict adaptation findings have been reported on RT, here we detected conflict adaptation on accuracy. Whereas we observed overall accuracy-based conflict adaptation across groups and tasks, accuracy-based conflict adaptation was marginally significant (p = 0.096) in Etkin et al.'s (2006) initial report, and not reported in other studies (Egner et al. 2008; Etkin et al. 2010; Etkin and Schatzberg 2011; Jarcho et al. 2013). However, a recent study validating a novel face-only emotional conflict task showed conflict adaptation as better performance for iI than for cI trials based on accuracy (error rates), but not RT in healthy adults (Clayson and Larson 2013). Krug and Carter (2010) reported similar overall findings in healthy adults using a modified version of the emotional and nonemotional face–word conflict tasks, which showed significant accuracy-based adaptation for both nonemotional and emotional tasks, but no RT-based adaptation. The discrepant conflict adaptation findings across RT and accuracy raise the question of whether the regulation of conflict involves both the efficiency (RT) and effectiveness (accuracy) of performance. Importantly, impaired performance to incongruent versus congruent trials (congruency effect) was evident for both RT and accuracy measures, which suggests the need for regulatory processing across both domains. Therefore, the presence of robust congruency effects in the absence of a speed–accuracy tradeoff, combined with accuracy-based conflict adaptation, support the validity of the current study. However, accuracy-based conflict adaptation was unrelated to age or anxiety disorders in the current study. Studies examining the influence of anxiety disorders on cognitive performance of various attention or conflict tasks often show unimpaired accuracy, but a slowing of RT. For example, a recent meta-analysis of anxiety and error monitoring showed no relationship between anxiety and error rates (Moser et al. 2013). This is consistent with the Attention Control theory proposed by Eysenck and colleagues, which suggests impaired efficiency (RT) but intact effectiveness (accuracy) in anxious individuals (Eysenck et al. 2007).
It is of note that unlike prior studies in GAD, which were performed in the MRI scanner, our study was conducted in the clinic. It is possible that contextual factors may influence behavioral performance. For example, stress induced by the scanner environment may be needed to detect the presence and absence of emotional conflict adaptation in healthy and anxious individuals, respectively. In fact, experimental mood inductions influence conflict adaptation (van Steenbergen et al. 2010; Schuch and Koch 2014). Adding a stress condition during conflict tasks in the clinic may better mimic the MRI scanner environment, and allow for future clinic studies to test for RT-based conflict adaptation in healthy versus anxious individuals. Compared with healthy adults completing the same emotional conflict task in the MRI scanner (Jarcho et al. 2013), our healthy adult group in the clinic exhibited faster RT, by 144 ms and 155 ms for iI and cI trials, respectively. Although we used the same procedures as in prior studies, some factors difficult to identify might have influenced the training or administration of the conflict tasks.
Limitations
The current report failed to detect anxiety- or age-related differences in conflict adaptation. Therefore, as in any study with null findings, it is possible that these results reflect a false negative, or type II error. However, the present study had sufficient statistical power to detect true differences. All samples were equal to or larger than corresponding samples in prior studies showing emotional conflict adaptation differences between healthy adults and adults with psychopathology (Chechko et al. 2009; Etkin et al. 2010; Jarcho et al. 2013). Comorbid disorders among a subset of anxious participants could have also contributed to our discrepant findings. However, none of our anxious participants had comorbid disorders that were exclusionary in Etkin et al. (2010), nor did our anxious participants have comorbid major depressive disorder, which, unlike GAD, has been linked to intact emotional conflict adaptation (Etkin and Schatzberg 2011). Another possibility is that using a relatively liberal exclusionary criterion of <60% accuracy may have had undue influence on our results. However, post-hoc analyses (data not reported) that used a more stringent criterion of <75% accuracy on either task excluded nine additional subjects (two healthy youth, seven anxious youth), and generally replicated findings from the full sample without revealing any additional significant effects. In light of the dichotomous categorization of adults and youth, another limitation involves the heterogeneity of youth age (range 8–17 years), which fails to account for developmental heterogeneity and corresponding differences in emotion processing and cognitive control. Future research might consider testing longitudinal studies of similarly aged youth and follow them into adulthood, to more precisely investigate the developmental trajectory of emotional and nonemotional conflict adaptation. Finally, the current study did not utilize neurobiological measures (e.g., fMRI), which might have revealed diagnostic and/or age group differences that were not observable at the level of behavioral performance.
Conclusions
In summary, we report no differences in behavioral measures of conflict adaptation between youth and adults with and without anxiety disorders. This study used the exact same task as in prior studies (Etkin et al. 2006; Egner et al. 2008; Etkin et al. 2010; Jarcho et al. 2013), but failed to replicate behavioral perturbations in emotional conflict adaptation linked to anxiety disorders. Emotional conflict adaptation and error-related negativity studies have shown opposing effects for anxiety disorders, and future studies should continue to examine cognitive control via both emotional and nonemotional versions of these paradigms in adults and youth with anxiety disorders.
Clinical Significance
Although initial findings support the translational application of the emotional conflict adaptation paradigm as a promising neurocognitive marker for anxiety disorders, replication of this behavioral phenomenon is needed. The current study of youth and adults did not replicate prior behavioral findings of failure to engage emotional conflict adaptation in anxiety disorders. For translational applications of novel neurocognitive measures, it is important to replicate findings across studies and research groups. For cognitive measures to be clinically useful and relevant to treatment, they must elicit robust and reliable between-group differences. For example, anxiety-related differences on the ERN measure consistently replicate across multiple research groups (Moser et al. 2013). However, the fact that there were no reliable between-group differences in the current study indicates a problem for clinical applications of the emotional conflict adaptation task. Therefore, this null finding suggests that emotional conflict adaptation may not be a viable cognitive process to pursue for the development of novel therapeutics or the refinement of existing clinical applications in anxiety disorders.
Disclosures
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.