
Abstract

To the Editor:
T
Autoimmune responses associated with the onset and progression of neuropsychiatric disorders such as OCD and Tourette's disorder are not limited to streptococcal infection, and in 2014, diagnostic criteria and recommendations for clinical evaluation of pediatric acute-onset neuropsychiatric syndrome (PANS) were released (Chang et al. 2014). PANS is defined as abrupt-onset OCD or severely restricted food intake with concurrent presence of neuropsychiatric symptoms after either an infectious trigger or an environmental trigger (Swedo et al. 2012). However, there are few reports on autoimmune-related OCD, including PANDAS and PANS, from regions other than North America, and there are particularly few reports from Asia. In this report, we present a 14-year-old Korean girl who presented with an abrupt onset and waxing-and-waning course of obsessive-compulsive symptoms with serological evidence for Mycoplasma pneumoniae and brain involvement, mainly basal ganglia.
Case Report
A 14-year-old girl presented to the Department of Psychiatry in January 2013 with obsessions and compulsions including the need for symmetry and orderliness, worries related to harm befalling her and her family, rituals involving herself and parents, and restricted food intake related to OCD symptoms. Emotional lability, irritability, behavioral regression, and deterioration in school performance were also present.
The patient was developmentally normal and had no premorbid neuropsychiatric symptoms before December 2009. With respect to family history, the paternal grandmother had OCD. The patient's OCD symptoms, emotional lability, and decreased school performance started in December 2009. Several months before the onset of these symptoms, the patient had had a low-grade fever, cough, and nonexudative pharyngitis with cervical lymphadenopathy. The pathogen was not identified. After 2 weeks of empirical treatment with amoxicillin/clavulanate, the patient's pharyngitis and lymphadenopathy had resolved. OCD symptoms waxed and waned despite cognitive behavioral therapy.
The patient developed binocular diplopia in January 2012. At that time, she did not have fever or any other physical or neurological symptoms except for diplopia. Brain magnetic resonance imaging (MRI) showed high-signal-intensity lesions in the right pons, both superior cerebellar peduncles, the right cerebral peduncle, and the midbrain (Fig. 1A, B). We performed herpes simplex virus type 1 and 2 polymerase chain reaction (PCR), enterovirus reverse transcription polymerase chain reaction (RT-PCR), acid fast bacilli (AFB) stain, fungal and bacterial cultures on cerebrospinal fluid (CSF), blood and throat cultures, and blood tests including complete blood cell count (CBC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), syphilis reagin test, antistreptolysin O, mycoplasma PCR and antibodies, hepatitis B and C viruses, and human immunodeficiency virus (HIV) antibody tests to rule out infection. Mycoplasma immunoglobulin IgM (3.8 S/C ratio) and IgG (81.5 AU/mL) were positive, but other tests were negative. Antinuclear antibody (ANA), anti-double stranded deoxyribonuclear acidase (anti-dsDNAase), antineutrophil cytoplasmic antibody (ANCA), rheumatoid factor (RF), anticardiolipin antibody, and lupus anticoagulant screening tests to examine a possibility of a connective tissue disease were all negative. Because lactate, pyruvate, ammonia, tandem mass spectrometry, serum amino acid, urine organic acid, indirect paraneoplastic antibody, and anti-neuromeylitis optica antibody were also negative, we could exclude the possibilities of metabolic disorders and paraneoplastic syndrome. We prescribed azithromycin for 3 days because of positive mycoplasma titers. However, azithromycin had no discernible therapeutic effect (Snider et al, 2005). The patient's diplopia was improved with steroid pulse therapy, but OCD symptoms were not improved at that time.
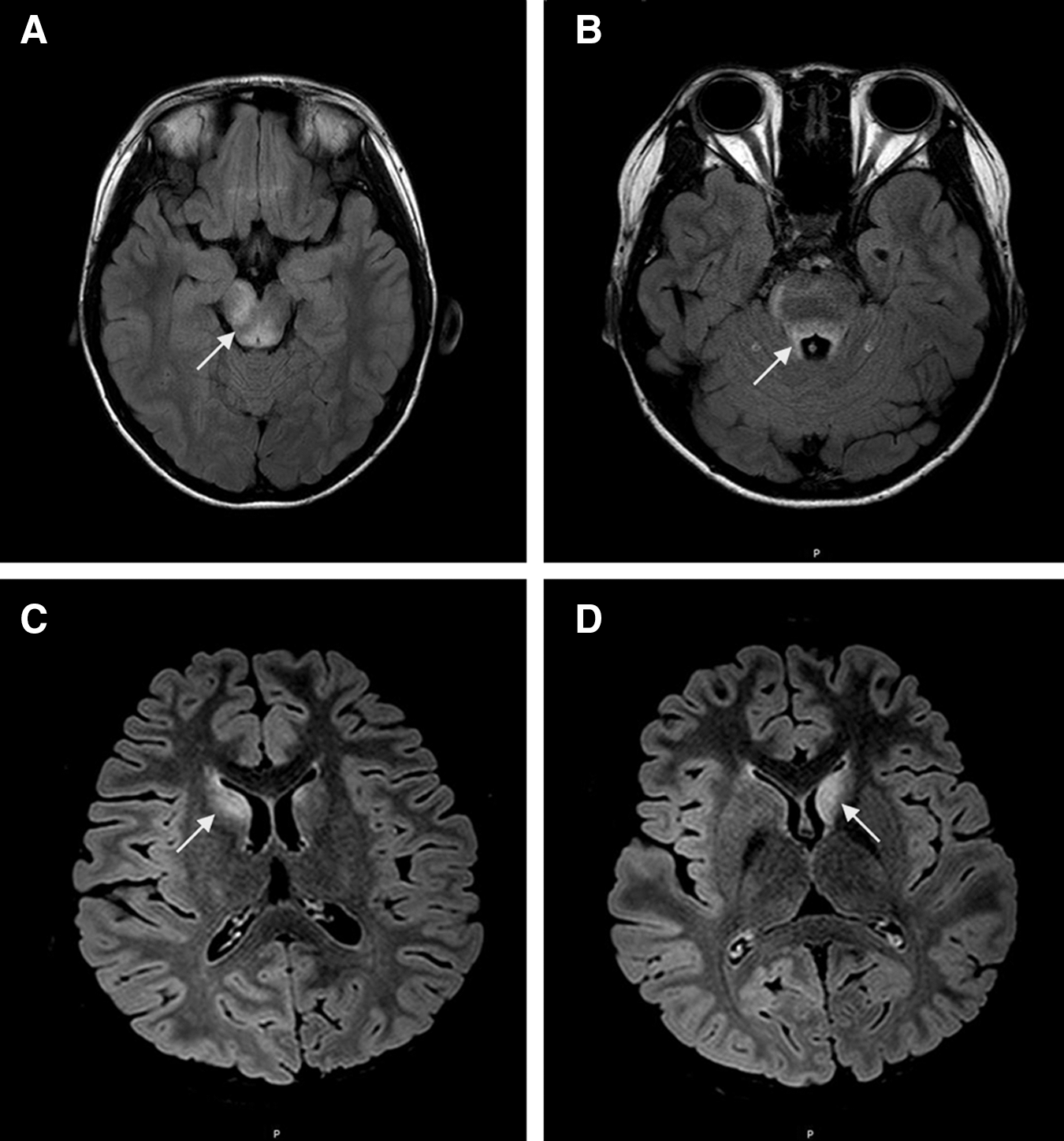
Sequential axial fluid-attenuated inversion recovery brain MR images of a 14-year-old girl with acute onset and exacerbation of obsessive-compulsive disorder (OCD) symptoms.
In January 2013, OCD symptoms became aggravated and food restriction associated with OCD symptoms developed. Truncal tremor and urinary incontinence were also present. Mycoplasma IgM antibody (3.1 S/C ratio) and IgG antibody (47.4 AU/ml) were positive, but PCR was negative. ESR (24 mm/h) was elevated and CRP level was within the normal range. Autoimmune tests of serum and CSF including ANA, anti-dsDNAse, ANCA, RF, antibodies to Hu, Yo, Ri, Ma2, collapsin response mediator protein 5 (CV2/CRMP5), amphiphysin, leucine-rich glioma inactivated 1 (LGI1), contactin-associated protein-like 2 (CASPR2), N-methyl-
Electroencephalography was normal. On brain MRI, the previously noted high-signal-intensity lesions involving mostly the right side of the brainstem had disappeared, and there were new high-signal-intensity lesions involving the left caudate nucleus head, left cerebral peduncle, left middle cerebellar peduncle, left cerebellar hemisphere, and right middle cerebellar peduncle.
The patient was treated with an antidepressant (fluoxetine up to 60 mg), antipsychotic (quetiapine up to 800 mg), and cognitive behavioral therapy, but these treatments did not have an effect. Her OCD symptoms did not respond to roxithromycin treatment or steroid pulse therapy. However, methylprednisolone (1 g/day) and intravenous immunoglobulin (IVIG) treatment (400 mg/kg/day) combination therapy effectively reduced OCD symptoms, truncal tremor, and urinary incontinence, and decreased the mycoplasma IgG titer (47.4 AU/mL) to an equivocal level (16.5 AU/mL) (Sakoulas et al, 2001). The brain lesions had decreased on follow-up MRI on April 10, 2013.
OCD symptoms relapsed in July 2013. Mycoplasma IgG antibody was again increased (92.4 AU/mL). Other laboratory findings were not significant. Brain MRI showed new strong high-signal-intensity lesions in the bilateral caudate nucleus head (Fig. 1C, D), and subtle high-signal-intensity lesions in the right middle cerebellar peduncle, pons, and midbrain. Methylprednisolone pulse therapy and IVIG were administered again, but were not as effective as the previous treatment. Plasmapheresis was tried and was effective for reducing brain lesions (Elia et al, 2005; Perlmutter et al, 1999). Since then, the OCD symptoms have gradually improved, and have been controlled with fluoxetine (60 mg), sertraline (200 mg), and olanzapine (20 mg).
Discussion
In this case, a 14-year-old girl presented with abrupt onset of OCD symptoms after pharyngitis and also had diplopia, food restriction, urinary incontinence, and behavioral regression with a wax-and-wane course. This patient had an abrupt, dramatic onset of OCD, restricted food intake, and more than two neuropsychiatric symptoms, and thus met the criteria for PANS. She also showed positive mycoplasma IgM and IgG titers and MRI findings of brain involvement, mainly basal ganglia. Moreover, mycoplasma IgG titer and the MRI finding of encephalitis were associated with the onset and progression of OCD or neurological symptoms. Frankovich and colleagues recently reported a 13-year-old girl who initially met the criteria for PANS, but finally more closely matched criteria for striatal/basal ganglia encephalitis (Frankovich et al. 2015), similar to our case.
In our case, mycoplasma IgM and IgG antibody were positive, but PCR was negative in January 2012 and in January 2013. In a recent systematic review and meta-analysis, Zhang et al. (2011) reported that PCR tests could lead to false negative results and suggested that PCR assays cannot replace serological tests for M. pneumoniae. Therefore, although the PCR assays were negative, there was a possibility of mycoplasma infection. However, serological tests could also be the result of the cross-reactive antibodies induced by mycoplasma infection or simply a marker of elevated autoimmune response. In this case, all other workups for infection had been negative, and OCD symptoms responded to immune-modulating treatment rather than antibiotic treatment for mycoplasma infection or conventional treatment for OCD. Therefore, our patient's OCD symptoms seemed to be related to an autoimmune response against the brain following mycoplasma infection.
M. pneumoniae has been associated with a number of postinfectious neurological disorders. Frankovich et al. reported a 10-year-old girl whose behavioral changes and compulsions were associated with mycoplasma infection and were improved with azithromycin (Frankovich et al. 2015). It has been also suggested that M. pneumoniae can be a stimulus triggering autoimmune process (Bae et al. 2011; Chang et al. 2014). In children with acute encephalopathy associated with mycoplasma infection, predominant symmetric basal ganglia with or without brainstem involvement has been observed on MRI (Saitoh et al. 1993; Bae et al. 2011). However, whether this basal ganglia involvement was related to direct infection or immune-mediated processes was not determined. In our case, MRI showed recurrent involvement of basal ganglia, cerebellum, and brainstem, probably related to autoimmune response triggered by mycoplasma infection. Because mycoplasma infection and mycoplasma-triggered autoimmune responses mainly target the basal ganglia, and the basal ganglia play a key role in the pathogenesis of OCD, mycoplasma infection should be considered in cases of abrupt-onset OCD (Harrison et al. 2009).
Studies of the overlap of PANS and inflammatory disease processes including infectious or autoimmune disease have only just begun. Muir et al. (2013) reported a case of abrupt-onset OCD following acute disseminated encephalomyelitis. Frankovich and colleagues (2015) studied five children and adolescents 8–18 years old at the onset of PANS, and suggested that there were different etiologies such as bacterial, autoimmune, and unknown. As these authors emphasized, it is important to find underlying infectious or inflammatory etiologies and to treat the etiologies in cases with abrupt-onset OCD or PANS. Therefore, clinicians should be alert to the possibility of PANS or underlying infectious and/or inflammatory diseases when a youth presents with psychiatric and physical symptoms that developed abruptly.
Footnotes
Disclosures
No competing financial interests exist.