
Abstract
Objective:
Catatonia as a result of autoimmune conditions offers new therapeutic opportunities for patients that child and adolescent psychiatrists should consider. However, the diagnosis is sometimes challenging when an autoimmune signature is not identified.
Methods:
In this study, we aim to summarize seven cases from a 20-year series of 84 youths with catatonia, including three cases that represented a diagnostic challenge because of the absence of positive autoimmune testing.
Results:
Immunosuppressive/modulatory treatment improved catatonic and psychotic features in all cases.
Conclusion:
To facilitate treatment decision-making, we propose a causality assessment score and a treatment algorithm, which may help clinicians consider whether an autoimmune condition is associated with catatonia.
Introduction
C
In addition, up to 20% of pediatric catatonias are secondary to a medical condition such as neurometabolic disorders (Wilson disease…) and genetic conditions (Huntington disease…) (Lahutte et al. 2008). This final point has crucial therapeutic implications (Consoli et al. 2012). Among medical conditions, autoimmune disorders can be treated with immunosuppressive treatments. Pediatric cases with catatonia have been successfully treated in systemic lupus erythematosus (SLE) (Lanham et al. 1985; Perisse et al. 2003; Marra et al. 2008), pediatric autoimmune neuropsychiatric disorders associated with streptococcus infections (PANDAS) (Elia et al. 2005; Kovacevic et al. 2015; Latimer et al. 2015), and anti-NMDA-receptor encephalitis (Florance et al. 2009; Schimmel et al. 2009), including malignant catatonia (Consoli et al. 2011; Wilson et al. 2013). In a recent study of 500 patients diagnosed with anti-NMDA-receptor encephalitis, 180 patients were younger than 18 years of age (Titulaer et al. 2012).
The presentation of anti-NMDAR encephalitis in children can be different from adults with a predominance of psychiatric symptoms, including psychosis and catatonia (Dalmau et al. 2008; Armangue et al. 2013). In addition, Honnorat et al. (2013) described an aggressive form of dysimmune nonparaneoplastic limbic encephalitis in children associated with anti-Hu antibodies. Other antibodies, such as anti-VGKC-complex (LGI1, CASPR2, and contactin-2), GlyR, D1R, D2R, AMPAR, GABA(B)R, anti-thyroperoxidase (TPO), anti-thyroglobulin (TG), and glutamic acid decarboxylase antibodies, are known for their pathologic roles in the development of encephalitis (Hacohen et al. 2013; Cox et al. 2015).
In this study, we aim to summarize all cases (N = 7) of autoimmune catatonia from a 20-year series of young individuals with catatonia (N = 84 to date) that we prospectively treated, including three cases that represented a diagnostic challenge because of the absence of positive autoimmune testing. Immunosuppressive/modulatory treatment dramatically improved all cases. To facilitate treatment decisions, we introduced a causality assessment score (CAUS) that may help clinicians determine whether an autoimmune condition is associated with catatonia.
Materials and Methods
We examined seven children and adolescents who presented catatonia with or without direct evidence of an underlying autoimmune condition and were admitted to the Department of Child and Adolescent Psychiatry at University Hospital La Pitié-Salpêtrière between 1993 and 2013. The details regarding this prospective study are available in Consoli et al. (2012), specifically regarding the systematic identification of organic conditions in the context of pediatric catatonia. To assess whether a suspected organic condition may be considered a causal medical risk factor associated with catatonia, we calculated a CAUS, which follows the principals of adverse medical effect assessment with standardized methods (Naranjo et al. 1981; Begaud et al. 1985).
For each patient, we systematically searched for and scored the following five causality-support criteria on a three-point scale (0 = absent; 1 = moderate; 2 = high): (1) the existence of similar cases in the literature; (2) the presence of clinical symptoms; (3) the presence of biological symptoms; (4) the presence of other paraclinical symptoms; and (5) the response to a specific treatment related to the suspected medical condition (e.g., improvement of catatonia after antiepileptic medication in the case of seizures). The details of how to rate this score are described in Table 1. Three raters independently scored the cases. Interrater reliability (3 raters, 20 cases) was excellent (Intraclass correlation coefficient = 0.95 [95% confidence interval: 0.86–0.99]). In Consoli et al. (2012), it appeared that scores ≥6 were likely associated with a medical condition.
CAUS, causality assessment score; CT, computed tomography; EEG, electroencephalogram; MRI, magnetic resonance imaging; PET, positron emission tomography.
Results
The mean age at admission of the seven patients (two boys, five girls) was 12.1 years (range: 6–17). All patients had an acute onset. The psychiatric diagnoses associated with catatonia were major depressive episode with psychotic features (N = 3), manic episode (N = 1), and childhood disintegrative disorder (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition [DSM-IV]) or ASD (DSM-5), with psychotic features (N = 3). The mean CAUS was 8.3 (range: 6–10). The mean Catatonia Rating Scale (CRS) score (Bush et al. 1996) was 25 (range: 16–33). The underlying autoimmune conditions associated with catatonia are summarized in Table 2.
CAUS, causality assessment score; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; EEG, electroencephalogram; IgG, immunoglobulin type G; MRI, magnetic resonance imaging; PET, positron emission tomography; SLE, systemic lupus erythematosus; TG, thyroglobulin; TPO, thyroperoxidase.
Three patients presented SLE, and one patient had anti-NMDA-receptor encephalitis. Two patients had no definitive evidence of autoimmune encephalitis, but did respond to plasma exchange (PE) and immunosuppressive treatment. One patient was finally classified as SLE because of positive antinuclear antibodies during follow-up. We decided to describe the last three cases as they were complex in their presentation and brought up the challenging question of what to do when there is no obvious proof of an autoimmune condition and no efficacy of the traditional therapeutics for catatonia.
Patient 1
A 7-year-old boy without a medical history and with a normal development presented with an acute onset of psychotic symptoms (persecutory delusions and visual/auditory/tactile hallucinations) and catatonia (mutism, schizophasia, social withdrawal, echolalia, and psychomotor agitation). He was first hospitalized in a neuropediatric unit where risperidone (0.75 mg/day) was first used and then increased at 1.5 mg/day 1 month later. Risperidone had a positive effect on sleep disorders and anxiety, but did not improve psychotic symptoms. It was stopped after 2 months due to lack of efficacy and weight gain.
A cerebral [18F] fluorodésoxyglucose (FDG) positron emission tomography (PET) image indicated a severe hypometabolism that affected the bilateral intern temporal cortex and a mild hypometabolism in the bilateral intern prefrontal cortex, which was compatible with acute encephalitis. Intravenous immunoglobulin (2 g/kg for 48 hours) was first administered, followed by a pulse of methylprednisolone (30 mg/kg/day) for 48 hours, 1 month after because of a lack of efficacy. A transient clinical improvement was observed, and he was subsequently treated with dexamethasone (18 mg/day) in conjunction with psychotropic treatment. At that time, different antipsychotics were administered. Aripiprazole (5 mg/day) was used during 2 months with no improvement on delusion and hallucinations. It was switched to haloperidol (5 mg/day then 10 mg/day) during 1 month, without efficacy and with several side effects (dyskinesia and akathisia).
At some point, the question of using clozapine was raised, but aborted due to the unusual psychiatric presentation. Two months after the first PET scan, a control [18F] FDG PET scan indicated a normalization of most hypometabolisms with exceptions in the frontomesial regions (Fig. 2). He was then in a day care psychiatric hospital. Psychotic signs and agitation mildly improved; however, he exhibited dramatic cognitive regression during the subsequent 4 months.
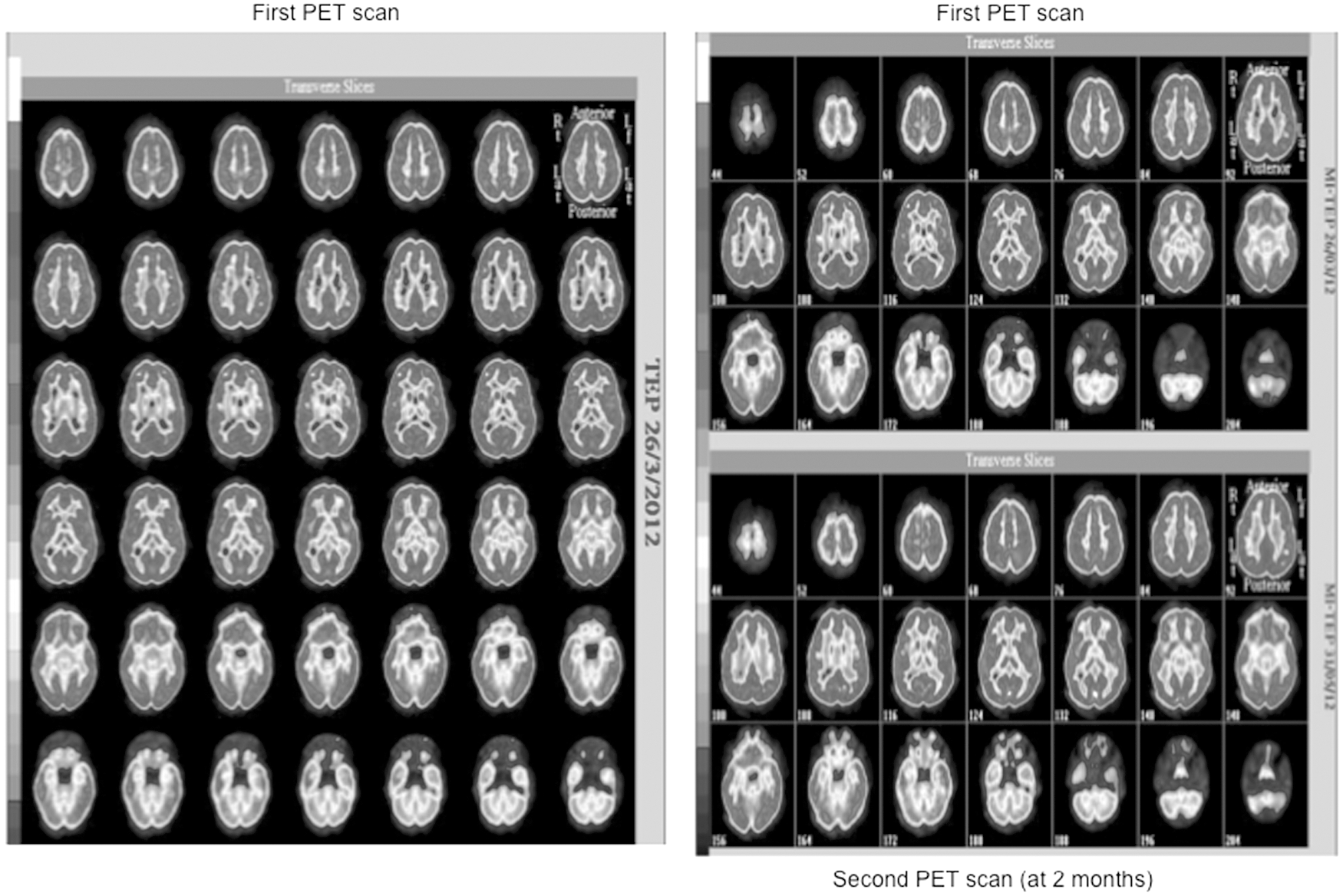
[18F]FDG positron emission tomography (PET) scan course in patient 1. The first PET scan (left) indicated a severe hypometabolism that affected the bilateral intern temporal cortex and a mild hypometabolism in the bilateral intern prefrontal cortex. The second PET scan (2 months later) indicated a normalization of the hypometabolism in the prefrontal cortex, an improvement of the metabolism in the temporal cortex, a significant improvement in the bilateral anterior medial temporal metabolism, and a moderate worsening of the discrete hypometabolism previously described in the frontomesial regions, which also affected the bilateral orbital regions. FDG, fluorodesoxyglucose.
He was then transferred to our department (week 0, Fig. 1a) to manage the behavioral disorders and continue the etiological explorations. All other explorations were negative, including standard blood tests, immunological blood tests (Antibodies: ANCA, anti-TPO, anti-TG, anti-DNA, anti-NMO, anti-endomysium, anti-transglutamase; Accessory salivary glands biopsy), metabolic explorations (neurometabolic and lysosomal disorders), genetic explorations (karyotype, Fluorescence in situ hybridization (FISH): 15q11-q13, 22q11, 22q13, 17p11.2), electroencephalogram (EEG), video-EEG, and brain imaging, including head computed tomography (CT) and magnetic resonance imaging (MRI; Supplementary Data; Supplementary Data are available online at

Course of the patients' catatonia and global functioning scores according to treatment. GAF, Global Assessment Functioning; ABC, Aberrant Behavior Checklist. “…” after a treatment indicates that it was continued.
A full body PET scan did not identify suspicious tumor process or other abnormalities. From week 1, he received high doses of benzodiazepines (lorazepam 4 mg/day). At admission, he scored 21 on the CRS, 122 on the Aberrant Behavior Checklist (ABC), 7 on the Clinical Global Impression scale (CGI), and 15 on the Global Assessment Functioning (GAF). The cognitive regression was impressive. The Kaufman Assessment Battery for Children scores indicated a developmental age range from 3 years and 6 months in the assembly of geometric figures to a maximum of 5 years and 10 months in story completion. At this time, it was not possible to use the Wechsler scale.
The dramatic cognitive regression, the persistence of psychotic features, the lack of response to a high dose of lorazepam, the PET scan abnormalities, and the early transient improvement with corticosteroids (started at week 2) suggested autoimmune conditions. Therefore, eight PEs were performed (four PEs at week 13 and four PEs at week 22). Drastic improvements in psychosis and catatonia were observed as shown in Figure 1a. Antipsychotic drugs were terminated and only benzodiazepines (lorazepam 2.5 mg/day) were continued. A monthly pulse of cyclophosphamide (for 6 months) followed by mycophenolate mofetil was initiated (at week 20).
At the last follow-up (at 1 year), clinical improvement was still observed: no aberrant behaviors and psychotic or catatonic symptoms were apparent. However the mild cognitive improvement obtained after the use of immunosuppressive treatment needed to be maintained with speech therapy, special education, and occupational therapy. The Cognitive and language assessments indicated severe phonological deficits and syntactic impairments, as well as mild intellectual disability (Wechsler scale: Verbal Comprehension Index = 53; Perceptual Reasoning index = 54; and Processing Speed Index = 62).
Patient 2
Patient 2 was a 6-year-old boy. He was the product of a 37-week pregnancy that was complicated by gestational diabetes. He presented a language delay (first words at ∼3 years old). He initiated a neuropediatric follow-up because of the language delay and gestational history and was referred to outpatient psychiatric consultations for anxiety, attention and academic difficulties at the age of 4. Language and psychomotor rehabilitation were initiated.
At the age of 6, the patient was admitted to our child psychiatric unit for an acute childhood disintegrative disorder with psychotic (visual and auditory hallucinations) and catatonic (negativism, catalepsy, social withdrawal, stereotypes, echolalia, verbigeration, and psychomotor excitement) features. He scored 33 on the CRS. The cognitive impairment was severe with a psychoeducational profile score that indicated a developmental age of 3 years and 3 months in fine motor skills, 2 years and 10 months in gross motor skills, 1 year and 10 months in receptive language, 1 year and 8 months in expressive language, and 3 years and 3 months in verbal cognition. The CGI score was 6 and the GAF score was 25. There was no vertical supranuclear ophthalmoplegia. Standard blood tests were negative.
The CSF explorations identified the presence of oligoclonal bands of IgG, but no specific antibodies (anti-NMDA, anti-Hu, anti-Yo) were identified. Extensive immunological (Antibodies: ANCA, anti-DNA, anti-TPO, anti-TG, anti-NMO, anti-endomysium, anti-transglutamase), genetic (karyotype, FISH: 15q11-q13, 22q11, 22q13, 17p11.2), and metabolic (neurometabolic and lysosomal disorders) explorations were performed and were normal, as well as EEG, video-EEG, and brain MRI (Supplementary Data). The treatment comprised benzodiazepines (Lorazepam 3 mg/day) and immunosuppressive drugs with corticosteroids and pulse methylprednisolone followed by oral prednisolone. No antipsychotic was used. Catatonic symptoms, behavior, and psychotic features dramatically improved with this regimen (Fig. 1b).
Regarding cognitive impairment, the improvement was not significant as the second PEP score (after 3 months) was the same in three fields and exhibited an increase in developmental age in the last two fields (a gross motor skills increase of 4 months and a receptive language increase of 3 months). After 2 months, his clinical presentation regarding catatonia and psychotic features was stable, although the cognitive improvement remained mild, and the IgG in the CSF continued to decrease.
Patient 3
Patient 3 is a 9-year-old girl with a normal development and in her usual state of good health, before being admitted to the pediatric emergency department for an acute onset of psychotic symptoms (mystic/persecutory delusions and visual hallucinations) and catatonia (mutism, negativism, refusal to eat, echolalia, social withdrawal, and echopraxy). She scored 26 on the CRS and 60 on the ABC. A mild cognitive impairment was observed, which was predominately in language and memory.
She was transferred to a pediatric unit, where the standard blood tests, the first immunological blood tests (Antibodies: ANF, anti-TPO, anti-TG, anti-DNA, anti-Ro, anti-La, anti-Sm, anti-nRNP, anti-Scl-70, anti-dsDNA, anti-histone, antibodies to nuclear pore complexes, anti-centromere, anti-sp100, anti-NMO, anti-endomysium, and anti-transglutamase), CSF explorations (protein = 0.17 g/L; Antibodies: anti-NMDA, anti-Hu, anti-Yo, anti-mGlur5, anti-NMO, anti-TPO, anti-TG; search for neurotropic viruses through PCR: Varicella-Zoster Virus, Cytomegalovirus, Epstein-Barr Virus, HHV6, Parvovirus B 19, Enterovirus, Adenovirus, TPHA, VDRL), and EEG were negative (Supplementary Data).
As a result of behavioral issues, she was transferred to a child and adolescent psychiatric intensive care unit. Originally, the cerebral MRI was considered normal; however, a second reading 1 month later identified multiple nonspecific signal abnormalities (Fig. 3). The metabolic (neurometabolic and lysosomal disorders) and genetic (karyotype, FISH: 15q11-q13, 22q11, 22q13, 17p11.2) explorations were also normal. The immunologic tests indicated positive anti-TPO, anti-TG antibodies, and anti-nuclear antibodies 1 month later on a second test; however, the remaining variables were negative (Supplementary Data).
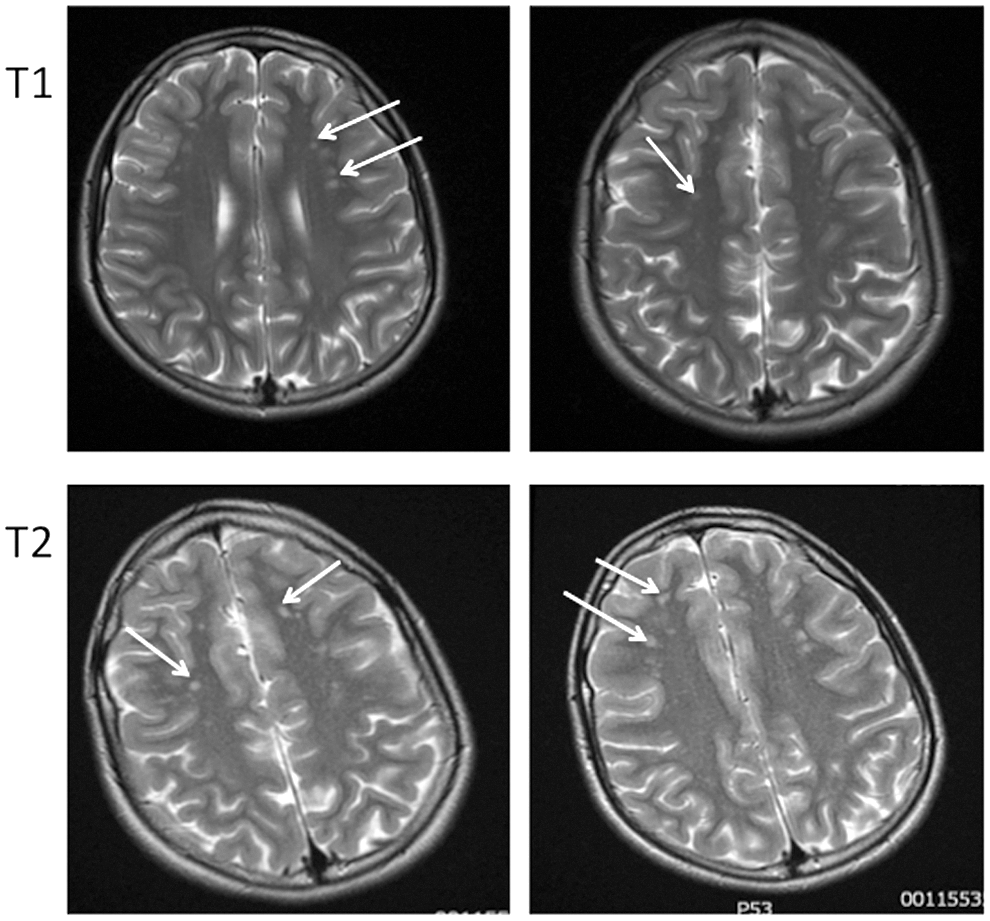
Magnetic resonance imaging in patient 3. Multiple nonspecific signal abnormalities were identified, including bilateral frontoparietal hyposignals of the white matter in the T1- and T2-weighted sequences (blue arrow).
At first, the treatment comprised an antipsychotic (risperidone 1.5 mg/day, increased to 2.5 mg/day over 1 month) and benzodiazepines (lorazepam 3.5 mg/day). As the catatonia worsened, the antipsychotic drug was terminated, and lorazepam was maintained and increased at 4.5 mg/day, which enabled an improvement of the catatonic symptoms (Fig. 1c). Although there was insufficient clinical evidence to confirm a diagnosis of an SLE, the multidisciplinary staff thought it was legitimate to consider an autoimmune condition and therefore to initiate aggressive immunosuppressive treatments; this decision was based on this atypical psychiatric presentation, its severity, the cognitive impairment, the prognosis, and the recent increasing titer of anti-TPO, antinuclear, and anti-TG antibodies.
The patient received five PEs during 1 week under general anesthesia, followed by monthly pulses of cyclophosphamide. The PE improved both the ABC and CRS scores, which continued to decrease after the first pulse of cyclophosphamide. Hence, these treatments showed and provided major improvements on catatonic and psychotic symptoms (Fig. 1c). We identified a slight relapse at the end of the first month, which triggered an earlier initiation of the second pulse. To date, the patient is stable regarding catatonia and psychotic and behavioral symptoms. She is waiting for her third pulse of cyclophosphamide and benzodiazepines (4.5 mg/day) to be continued. Thus far, there have been no relapses or tolerance issues. Regarding the cognitive impairment, she showed partial improvement: her language and lack of words have improved; however, she continues to exhibit a lack of short-term memory.
Discussion
Current evidence has reduced the controversies regarding the high rates of medical conditions associated with childhood and adolescent catatonia (Lahutte et al. 2008). Of all causal medical conditions, autoimmune encephalitis has a legitimate role as a therapeutic option exists that is dramatically different and can offer patients amazing opportunities (Schimmel et al. 2009; Consoli et al. 2011, 2012). In these cases, catatonia appears to have an acute onset (sometimes following a brief period of nonspecific symptoms) and a stuporous type with a potential switch with the excited subtype (Consoli et al. 2012). Catatonia is also likely associated with striking psychiatric features that suggest encephalitis, including delirium, severe and invasive hallucination phenomena (visual, auditory, tactile), and cognitive impairment and regression. Neurological signs should be assessed (e.g., seizures, abnormal movements), but may be absent.
In our three cases, we observed major improvements on catatonic and psychotic features, quickly after the initiation of aggressive immunosuppressive treatments (corticoids, PE…). However the cognitive signs were severe, and even after several months of treatment, the patients continued to exhibit cognitive impairment, mainly in memory and language fields (Finke et al. 2012) because of the neurological sequelae of encephalitis. Therefore, cognitive profiles must be monitored and checked often throughout the follow-up.
The three cases detailed in this study represent a real therapeutic challenge. From recent studies (see Introduction section), it appears genuine and important to identify autoimmune dysfunction by screening the CSF for antibodies, such as anti-NMDA-R, anti-Yo, and anti-Hu, through lumbar puncture because the levels of antibodies in the CSF appear to correlate better with symptom outcome compared with the serum (Dalmau et al. 2011; Gresa-Arribas et al. 2014; Chang et al. 2015). However, antibodies can be identified in the CSF months later (Dalmau et al. 2008) or can remain negative (Hacohen et al. 2013).
We developed the CAUS score to provide evidence that medical conditions could be causal in cases with catatonic syndrome. Among the five criteria, the response to cause-targeted therapy is crucial. In cases of an absence of biological evidence for an underlying autoimmune condition, such as in patients 1 and 3, we propose to consider whether a presumptive immunosuppressive treatment would be efficient before considering electroconvulsive therapy (ECT) in very young patients (Consoli et al. 2010).
When the serum is negative for the antibody tests that are currently available, the suspicion of an immune-mediated central nervous system disorder can be based on the clinical characteristics that previously described the negative results for other catatonia causal conditions and the resistance to high doses of benzodiazepines. The secondary effects of antipsychotics (e.g., malignant catatonia) (Cohen et al. 2005; Consoli et al. 2012) are also another argument for the treatment of these patients with immunosuppressive drugs.
The CAUS score appears to be an interesting tool to evaluate the probability of an underlying condition for clinicians who deal with these tricky situations and question the risk of a treatment delay. The CAUS score is not validated yet due to the low number of patients with catatonia to perform proper statistics. As the current case series is small, we are gathering new cases within a multisite consortium interested in rare diseases to validate this diagnosis tool. It will be the subject of a future collaborative study in which we will group together cases of catatonia associated or not with medical condition and use receiver operating characteristic (ROC) analysis to assess which threshold produces the best area under the curve when classifying catatonia associated with medical conditions versus catatonia without medical condition.
In the current cases, although the literature remains limited, clinical improvement regarding catatonia and psychotic symptoms appeared to be strongly time related to immunotherapy. This finding suggests that a reduction in circulating antibodies can be an effective intervention even in patients with a long history (e.g., Agrawal et al. 2010); however, the long-term cognitive prognosis likely depends on how early and aggressive the treatment is initiated (Finke et al. 2012). This may explain the frequent cognitive sequels found in our series.
Immunosuppressive treatments were defined after multidisciplinary meetings of psychiatrists and internists specialized in lupus and autoimmune disease management. Schematically, first-line therapy was based on high-dose steroids (mainly prednisone 1 mg/kg) often initiated with three intravenous pulses of methylprednisolone to get an earlier onset of response (patients 1, 2, and 3). Because these “first-line” treatments fail in 30%–40% of the patients (Armangue et al. 2012) and there is an increasing number of reports showing that rituximab is effective, this drug is increasingly being used in combination with intravenous immunoglobulin and steroids, or after first-line immunotherapies (Ishiura et al. 2008; Luca et al. 2011; Frankovich et al. 2015).
Therefore treatments like rituximab and cyclophosphamide represent a second line of treatment. Rituximab and cyclophosphamide, alone or combined, are often effective in adults; however, because of the potential adverse effects of cyclophosphamide (infections, malignancies, infertility, and premature gonadal failure), most pediatricians only use cyclophosphamide when the first-line treatments fail (Kashyape et al. 2012; Titulaer et al. 2013). However, on the other hand, the cognitive prognosis is known to be uncertain and time related to the initiation of the immunosuppressive treatment. For example, early treatment of NMDA encephalitis in children results in a better general outcome (Byrne et al. 2015).
Hence in case of failure or aggressive disease, immunosuppressive drugs, mainly intravenous cyclophosphamide, were added (patients 1 and 3) (Ishiura et al. 2008). In catatonic presentation, we have shown the effectiveness of plasmatic exchanges (Marra et al. 2008). In case of severe catatonia, PE can be immediately initiated with corticosteroids even at a very young age. Intravenous immunoglobulins have been proposed in cases of neurological damage due to lupus (patient 1). The use of intravenous immunoglobulins does not present a risk of triggering immunosuppression, therefore it is safer than other aggressive treatments, but the efficacy has not been proved yet.
Figure 4 represents the diagnostic and therapeutic protocol we used for these cases (including the ones without clear autoimmune evidence). This algorithm is a preliminary proposal that should help physicians who encounter children and adolescents with catatonia arguing for the autoimmune condition. Its limit is due to the limited number of cases described so far. However, it seems interesting to share this multidisciplinary protocol, which resulted in positive outcomes in our patients.
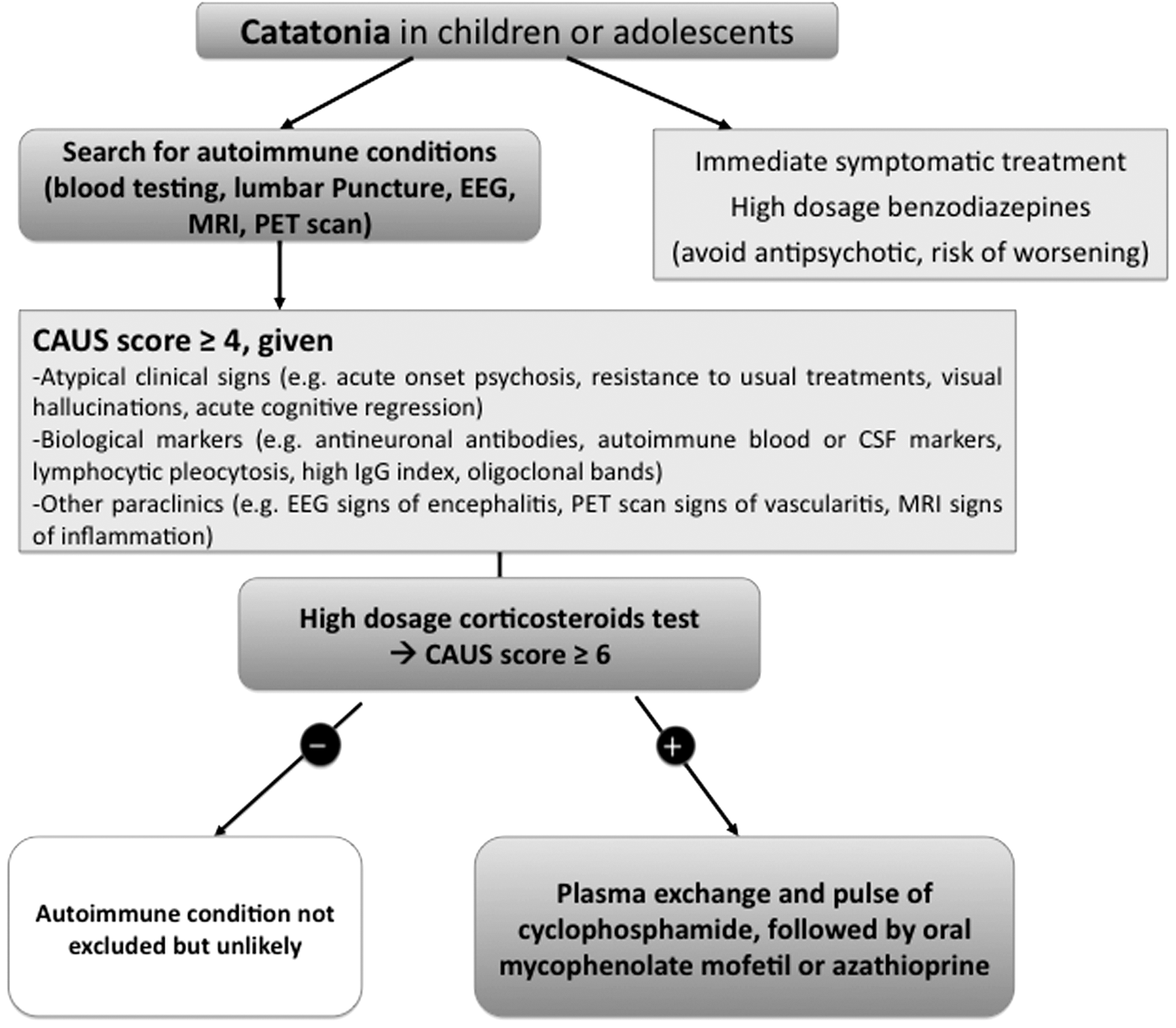
Diagnostic and therapeutic algorithm for children and adolescents with catatonia. All treatment decisions are made through a multidisciplinary staff: neuropediatricians, internal medicine specialists, radiologists, child and adolescents psychiatrists.
Conclusion
Catatonia in children and adolescents is characterized by a high frequency of organic conditions. Autoimmune conditions represent a diagnostic and therapeutic challenge because treatments are drastically efficient on catatonic and other acute psychiatric symptoms and the timing of treatment initiation can limit neurological and cognitive sequels. We emphasize the importance and need to ensure an early diagnosis of the underlying autoimmune condition by the identification of antibodies in CSF. In cases similar to these presented in this study, in which no evidence of an autoimmune disorder is identified, the early and aggressive use of immunosuppressive or immunomodulatory treatment, including PE, is worth considering as a therapeutic option.
Footnotes
Acknowledgment
The authors thank all the patients and their families for participating.
Author Contributions
Study concept and design: V.F., M.R., D.C., A.C. Acquisition of data: V.F., M.R., K.D., X.S.C., A.L., M.S., J.H., Z.A., P.G., A.C. Interpretation of data: V.F., M.R., K.D., X.S.C., A.L., M.S., J.H., Z.A., P.G., D.C., A.C. Drafting the article: V.F., M.R., D.C., A.C. Critical revision of the article for important intellectual content: Z.A., D.C., A.C. Final draft: All authors.
Disclosures
Dr. David Cohen reported past consultation for or the receipt of honoraria from Schering-Plough, Bristol-Myers-Squibb, Otsuka, Shire, Lundbeck, Janssen, Sanofi-Aventis, and IntegraGen. Dr. Angèle Consoli reported receiving travel support from BMS. Dr. Julien Haroche received honoraria from Glaxo Smith Kline for counseling on targeted treatments of patients with histiocytosis. No other authors reported financial disclosure or conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.