
Abstract
Objective:
Treatment of early-onset schizophrenia spectrum psychosis (EOS) is hampered by limited data on clinical presentation and illness course. We aimed to systematically review the clinical characteristics, diagnostic trajectories, and predictors of illness severity and outcomes of EOS.
Methods:
We conducted a systematic PubMed, PsycINFO, and Embase literature review including studies published from January 1, 1990 to August 8, 2014 of EOS patients with 1) ≥50% nonaffective psychosis cases; 2) mean age of subjects <19 years; 3) clinical samples recruited through mental health services; 4) cross-sectional or prospective design; 5) ≥20 participants at baseline; 6) standardized/validated diagnostic instruments; and 7) quantitative psychotic symptom frequency or severity data. Exploratory analyses assessed associations among relevant clinical variables.
Results:
Across 35 studies covering 28 independent samples (n = 1506, age = 15.6 years, age at illness onset = 14.5 years, males = 62.3%, schizophrenia-spectrum disorders = 89.0%), the most frequent psychotic symptoms were auditory hallucinations (81.9%), delusions (77.5%; mainly persecutory [48.5%], referential [35.1%], and grandiose [25.5%]), thought disorder (65.5%), bizarre/disorganized behavior (52.8%), and flat or blunted affect/negative symptoms (52.3%/50.4%). Mean baseline Positive and Negative Syndrome Scale (PANSS)-total, positive, and negative symptom scores were 84.5 ± 10.9, 19.3 ± 4.4 and 20.8 ± 2.9. Mean baseline Clinical Global Impressions-Severity and Children's Global Assessment Scale/Global Assessment of Functioning (CGAS/GAF) scores were 5.0 ± 0.7 and 35.5 ± 9.1. Comorbidity was frequent, particularly posttraumatic stress disorder (34.3%), attention-deficit/hyperactivity and/or disruptive behavior disorders (33.5%), and substance abuse/dependence (32.0%). Longer duration of untreated psychosis (DUP) predicted less CGAS/GAF improvement (p < 0.0001), and poor premorbid adjustment and a diagnosis of schizophrenia predicted less PANSS negative symptom improvement (p = 0.0048) at follow-up. Five studies directly comparing early-onset with adult-onset psychosis found longer DUP in EOP samples (18.7 ± 6.2 vs. 5.4 ± 3.1 months, p = 0.0027).
Conclusions:
EOS patients suffer substantial impairment from significant levels of positive and negative symptoms. Although symptoms and functioning improve significantly over time, pre-/and comorbid conditions are frequent, and longer DUP and poorer premorbid adjustment is associated with poorer illness outcome.
Introduction
E
Since the appearance of Diagnostic and Statistical Manual of Mental Disorders, 3rd ed. (DSM-III) and International Statistical Classification of Diseases and Related Health Problems, 9th revision (ICD-9), schizophrenia patients with an early onset are diagnosed using the same criteria as for adults (American Psychiatric Association 1980). Schizophrenia-spectrum disorders have shown sufficient diagnostic stability from childhood throughout adolescence and adulthood (Masi et al. 2006; Remschmidt and Theisen 2012) to justify the use of age-independent diagnostic criteria; however, more data about diagnostic trajectories can help determine sources of early misclassification in youth with EOS.
The evidence base is limited regarding developmentally sensitive descriptions of the symptomatology, clinical characteristics, and outcome of EOS. Textbooks and reviews often refer to a small number of studies, in which EOS, in contrast to adult-onset schizophrenia (AOS), is characterized by an even larger preponderance of males, more insidious onset (especially in prepubertal schizophrenia), less complex or elaborated delusions, hallucinations affecting several sensory modalities, more negative symptoms, disorganization and formal thought disorders, a higher frequency of premorbid neurodevelopmental abnormalities, a stronger biological disposition, and a poorer prognosis; probably caused by a more severe and early disruption of brain development (Werry 1992; Asarnow et al. 1994; Remschmidt et al. 1994; Masi et al. 2006; Remschmidt and Theisen 2012). The prognosis of EOS is debated, however, as recent studies from early intervention services suggest that early-onset patients might have an equally good or even better outcome than adult-onset patients (Schimmelmann et al. 2007; Amminger et al. 2011), at least in settings with comprehensive early recognition and outreach efforts (Schimmelmann et al. 2013).
There seems to be considerable overlap in phenomenology between schizophrenia and affective symptomatology in children and adolescents with psychosis, and the clinical picture in youth may become clear only with time, making the differential diagnosis between schizophrenia and affective disorders with psychotic symptoms difficult, and the treatment strategy complicated (McClellan et al. 1993; Werry et al. 1994). The most common mistake seems to primarily involve a misclassification of mood disorder as schizophrenia (Werry 1992; Masi et al. 2006). Schizophrenia and bipolar disorders share both some clinical features and risk factors, and evidence suggests that the neurodevelopmental trajectories differ on a quantitative rather than a qualitative level (Arango et al. 2014).
The diagnostic challenge of psychosis in childhood and adolescence extends to the differentiation of schizophrenia from pervasive developmental disorder, severe personality disorders/traits, posttraumatic stress disorder, generalized anxiety disorder, and obsessive-compulsive disorder (OCD) without insight (Driver et al. 2013; McClellan and Stock 2013). Further, on the other end of the psychosis continuum, an estimated median of 10–17% of the general population of children and adolescents report nonclinically relevant psychotic symptoms, such as hallucinations and delusions (Kelleher et al. 2012; Jeppesen et al. 2015).
In recent years, there has been considerable interest in early identification of psychosis in children and adolescents (NICE Clinical Guideline 155, 2013; Schimmelmann et al. 2013). Early identification after onset of psychosis aims to reduce the duration of untreated psychosis (DUP); that is, the time from onset of psychotic symptoms to initiation of adequate treatment. The early detection and treatment of people at risk for – or in the earliest phases of – psychotic disorders is currently regarded as the most promising strategy to improve treatment outcome and long-term prognosis, and thus reduce the consequences of full-blown psychotic disorder in this population (Marshall et al. 2005; Melle et al. 2008). Longer DUPs have been found among early-onset psychosis (EOP) patients compared with adult-onset psychosis (AOP) patients (Schimmelmann et al. 2013), and for this reason, a focus on reducing DUP might be even more important in EOP than in AOP patients.
An increased evidence base concerning the clinical presentation and course of psychosis in childhood and adolescence is the first step toward identifying improved strategies for early detection and development of more operational treatment guidelines. Currently, the commonly cited facts are based on a small number of studies of limited quality because of small sample sizes, retrospectively defined samples, lack of standardized assessments for diagnostic evaluation, and the mixing of data from first and multi-episode patients.
In order to provide comprehensive evidence and compare this against the currently held notions, we systematically reviewed the literature on the clinical characteristics and outcome of EOS-spectrum psychosis in children and adolescents, published since 1990. We chose 1990 as the starting point to include only studies using either ICD-9/ICD-10 or Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria for schizophrenia (American Psychiatric Association 1994). The specific aims of the current study of predominantly schizophrenia-spectrum psychosis in children and adolescents were to: 1) Describe the clinical characteristics of EOS patients; 2) determine the illness trajectories, including diagnostic trajectories, and symptomatic and functional outcomes; 3) explore predictors of severity and outcome of illness in the first years after treatment initiation; and 4) compare data from AOP and EOP patients, when the included studies directly compared these two patient groups.
Methods
Search
We searched the databases PubMed, PsycINFO, and Embase and hand-searched reference lists of eligible papers and pertinent reviews for studies published since January 1, 1990 reporting nonretrospective data in children or adolescents with a diagnosis of predominantly nonaffective psychosis using a comprehensive set of search terms (Table 1). The literature search was performed by Drs. Stentebjerg-Olesen and Jeppesen with the assistance of an information specialist. The literature search was completed on August 7, 2014.
Inclusion and exclusion criteria
To be included, the studies had to fulfill the following criteria.
1. At least 50% of the participants had nonaffective psychosis (first or multi-episode)
2. Mean age of participants was <19 years at baseline
3. Clinical samples recruited through mental health services
4. Cross-sectional or prospective design
5. Data for at least 20 participants at baseline
6. Standardized, validated instruments used for diagnostic evaluation and psychopathological examination
7. Studies reported count data, proportions, or scores of psychotic symptoms (e.g., hallucinations, delusions, thought disorder, bizarre behavior, catatonia) or continuous data on psychopathology
8. No study restriction for inclusion based on a threshold for psychopathology scores
9. Published in the English language
Studies were excluded according to the following criteria.
1. Patients with psychotic disorders clearly related to substance abuse or physical conditions
2. Retrospective design
3. Review articles
As indicated, we decided to include only studies with a prospective or cross-sectional design and of clinical cohorts with research assessments using standardized psychometric instruments. This was done to minimize ascertainment biases and imprecisions of recording in retrospective evaluations of diagnoses and psychopathology as well as selection biases from unmeasured attrition during follow-up.
Extracted variables
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Moher et al. 2010) guidelines. The risk of selection and information biases in individual studies was addressed by including only those studies reporting data on at least 20 participants and using reliable and validated psychometric assessments.
From each study, we extracted detailed data on study population (first episode psychosis or mixed first episode and multi-episode patients); sampling years; number of patients at baseline and follow-up; mean age at baseline; mean age at onset of psychosis; follow-up time; percent of males; psychiatric family history; diagnostic instrument used; primary and comorbid diagnoses; trajectories of diagnoses; treatment characteristics; psychometric instruments used; measures of total, positive and negative psychotic symptoms; symptoms of disorganization; affective symptoms and general/other psychopathology; instruments for measuring social, premorbid function/developmental delay and global function plus their respective results; DUP; duration of untreated illness (DUI); and intelligence quotient (IQ).
Statistical analyses
We used descriptive statistics to summarize the study, patient and illness characteristics of the included studies, reporting weighted means ± standard deviations (SD) and weighted proportions. In longitudinal studies, we compared baseline psychopathology scores with end-point ratings, using paired t tests to assess if changes were significant over time. The following variables with at least three studies contributing data were examined: Positive and Negative Syndrome Scale (PANSS) (Kay et al. 1987) total score, and positive and negative symptom subscores; Clinical Global Impressions-Severity (CGI-S) scale (Guy 1976) scores; Children's Global Assessment Scale (CGAS) (Shaffer et al. 1983); and Global Assessment of Functioning (GAF) (Endicott et al. 1976) scores.
Further, we conducted exploratory correlational analyses testing the associations between each of the following baseline variables, using the reported means and proportions per study as the unit of analysis: First episode versus multi-episode or mixed samples; percent males; age; age at illness onset; IQ; DUP; percent with presence of any psychiatric family history; percent with primary diagnosis of schizophrenia, schizoaffective disorder, psychotic disorder not otherwise specified (psychosis-NOS), schizophrenia spectrum disorders, bipolar disorder, or depressive disorder, as well as baseline scores in PANSS total score; and positive, negative, and general psychopathology symptom subscores, CGI-S scores, and GAF/CGAS scores. In exploratory analyses of factors influencing the change in psychopathology scores, all baseline variables were examined as potential moderators, and study duration and attrition were examined as potential mediating factors. Because most variables were non-normally distributed, we used nonparametric tests; that is, Kruskall–Wallis test for comparison of measurement variables between two categorical groups (i.e., first episode vs. mixed samples), and Spearman's ρ for all other analyses testing correlations between two measurements variables. R2 reflects the percent variance explained by the specific moderating or mediating variable. All analyses were conducted in JMP 5.0.1, SAS Institute, Inc, 1989–2003, Cary, NC, using two sided tests with α set at 0.05.
Results
Study characteristics
The literature search resulted in 1186 hits after duplicates were removed (Fig. 1). An additional 17 publications were identified through successively conducted hand searches of reference lists of eligible articles; therefore, a total of 1203 records were screened. Of these, 399 records were excluded based on title, 609 were excluded based on abstract, and the remaining 195 full text articles were assessed for eligibility. Altogether, 160 of these full text articles were excluded because of the mean age of participants being >19 years (n = 90), they were review articles (n = 24), had a retrospective design (n = 23), had <20 participants (n = 7), <50% with nonaffective psychosis in the study (n = 6), there were no psychopathology scores (n = 4), sample at risk of psychosis (n = 4), or sample selected for severe illness (n = 2). Therefore, 35 studies were included in this review.
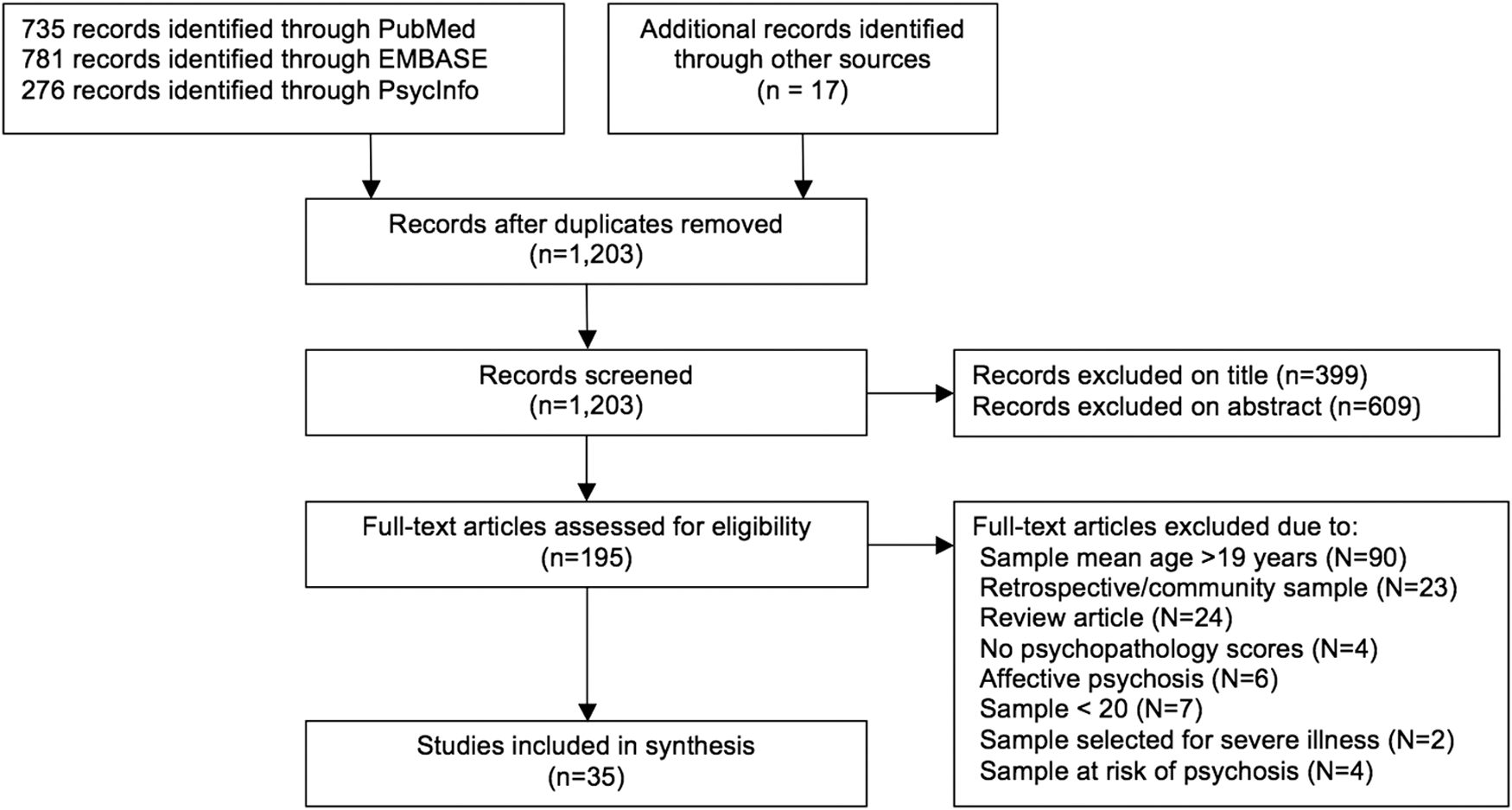
Flowchart of records.
Study, patient, and treatment characteristics
The 35 included studies represented 28 independent samples, of which 22 were prospective and 6 were cross-sectional, with a total of 1506 patients at baseline and 773 patients at follow-up (after a mean of 2.2 ± 1.7 years). The studies used a range of psychometric and diagnostic instruments (Table 2).
AffPS, affective psychosis; BD, bipolar disorder; BDI, Beck Depression Inventory; BPRS, Brief Psychiatric Rating Scale; CAFEPS, Child and Adolescent First-Episode Psychosis Study; CBCL, Child Behavior Checklist, CBI, Children's Behavioral Inventory; CBS, Child Behavior Scale; CDS, Children's Depression Scale; CDSS, Calgary Depression Rating Scale for Schizophrenia; CGAS, Childrens Global Assessment Scale; CGI(-I; -S), Clinical Global Impressions Scale (-Improvement; -Severity); DD, depressive disorder; DES, Dissociative Experiences Scale; DSM, Diagnostic and Statistical Manual of Mental Disorders; FE, first-episode; GAF, Global Assessment of Functioning; GDS, General Developmental Scale; HDRS, Hamilton Depression Rating Scale; ICD, International Classification of Diseases; K-SADS-PL, Kiddie Schedule for Affective Disorders And Schizophrenia – Present And Lifetime Version; ME, multi-episode; PANSS, Positive And Negative Syndrome Scale; PAS, Premorbid Adjustment Scale; PSE, Present State Examination; PsyNOS, psychosis not otherwise specified; SA, schizoaffective disorder; SANS, Schedule for Negative Symptoms; SAPS, Schedule for Positive Symptoms; SASS, Social Adaptation Self-evaluation Scale; SCID, Structured Clinical Interview for DSM Disorders; SCFS, Strauss-Carpenter Level of Functioning Scale; SCOS, Strauss-Carpenter Outcomes Scale; SCS, Strauss Carpenter Prognostic Scale; SOFAS, Social and Occupational Functioning Assessment Scale; SZ, schizophrenia; WAIS, Wechsler Adult Intelligence Scale; WHO-DAS = World Health Organization-Disability Assessment Schedule; WISC, Wechsler Intelligence Scale for Children; YMRS, Young Mania Rating Scale.
Seventeen samples included only first episode patients (n = 872) and 11 samples included a mixture of first and multi-episode/chronic patients (n = 634) (Table 2).
The mean age of patients was 15.6 ± 1.9 years at baseline (range of means: 9.6–18.4 years) and the mean age at onset of psychosis was 14.5 ± 2.4 years (range of means: 7.7–16.4 years) (Table 3). The mean DUP was 17.2 ± 12.8 months (range of means 2–45 months). The mean percentage of males was 62.3 ± 10.8%.
Means and proportions are weighted by the total number of patients in each study who contributed with a score.
ADHD, attention-deficit/hyperactivity disorder; CD, conduct disorder; IQ, intelligence quotient; NOS, not otherwise specified; ODD, oppositional defiant disorder; PDD, pervasive developmental disorder; PTSD, posttraumatic stress disorder.
At baseline, 89.0% of the patients had a diagnosis of a schizophrenia spectrum psychosis (Table 3). Comorbid psychiatric disorders were common. These primarily included posttraumatic stress disorder (PTSD) (34.3%), attention-deficit/hyperactivity disorder (ADHD) and disruptive behavior disorders (oppositional defiant disorder [ODD] and conduct disorder [CD]) (externalizing disorders together: 33.5%), substance abuse disorders (32.0%), and pervasive developmental disorder (PDD) (12.5%) (Table 3).
More than 90% of the patients were treated with antipsychotic medications at baseline (Table 3). Comedications, primarily antidepressants and mood stabilizers, were common.
Symptom dimensions at baseline
The most frequently recorded symptoms were auditory hallucinations (81.9%), any hallucinations (70.3%), and other hallucinations (54.8%), followed by delusions (any: 77.5%, persecutory: 48.5%, referential: 35.1%, and grandiose: 25.5%) (Table 4).
Studies reporting on one symptom are not necessarily the same as those reporting on another symptom
Thought disorder was common (65.5%), and 52.8% of patients were reported to display bizarre behavior. A total of 50.4% had negative symptoms, and 52.3% had flat/blunted affect. Data on affective symptoms were limited.
Diagnostic trajectories
Nine studies reported both baseline and follow-up diagnoses. In these studies, 88% of the patients at baseline and 75% at follow-up had a diagnosis of a schizophrenia spectrum disorder, whereas the proportion of patients with affective disorders increased from baseline to follow-up (from 12.2% to 24.5%) (Table 5). Overall, the proportion of patients with fully developed syndromes of schizophrenia (from 31.9% to 40.2%), bipolar disorder (from 8.9% to 14.3%), and depressive disorder (from 1.9% to 4.1%) increased, and the proportions of patients with psychosis NOS (from 15.8% to 12.0%) and, especially, schizophreniform disorder (from 21.3% to 1.1%) decreased; however, the diagnostic shifts were not statistically significant.
Psychopathology and function scores at baseline and over time
Mean PANSS total, positive, and negative symptom scores at baseline were 84.3 ± 10.9, 19.3 ± 4.4, and 20.8 ± 2.9, respectively, at baseline. Mean baseline CGI-S score was 5.0 ± 0.7 and CGAS/GAF scores were 35.5 ± 9.1 (Table 6).
Bolded values indicate p < 0.
One study did not report the overall n.
BPRS, Brief Psychiatric Rating Scale; CGAS, Children's Global Assessment Scale; CGI, Clinical Global Impressions Scale; GAF, Global Assessment of Function Scale; PANSS, Positive and Negative Syndrome Scale.
In prospective studies with both baseline and follow-up data, all mean psychopathology ratings improved significantly from baseline to follow-up. In these studies, mean PANSS total, positive, and negative symptom scores were 84.5 ± 10.8, 19.4 ± 4.4, and 20.2 ± 2.9, respectively at baseline, and 60.8 ± 6.1 (p = 0.0006, n = 7), 12.4 ± 2.0 (p = 0.0004, n = 10), and 16.6 ± 2.4 (p = 0.0003, n = 10) at follow-up. Mean CGI-S scores were reduced from 5.5 ± 0.1 at baseline to 3.2 ± 0.2 at follow-up (p = 0.012, n = 4), and mean CGAS/GAF scores increased from 38.4 ± 10.1 to 63.8 ± 9.0 (p = 0.0046, n = 6).
Direct, post-hoc comparison between youth and adult samples within included studies
Six studies, representing five youth samples, directly compared the phenomenology of EOP and AOP. The mean age at baseline was 17.6 ± 0.7 years in EOP patients and 23.9 ± 4.1 years in AOP patients. The mean age at onset of psychosis was 16.2 ± 0.3 and 23.5 ± 1.7 years, respectively. The percentage of males was roughly similar in EOP compared with AOP patients (63.1 ± 9.9% vs. 69.2 ± 6.4%, p = 0.28), and baseline mean CGAS/GAF scores were also similar in both groups (28.9 ± 5.2 vs. 29.6 ± 5.3, p = 0.88). However, more EOP patients had schizophrenia spectrum disorders (90.0 ± 5.9 % vs. 85.0 ± 10.5%, p = 0.036), and the mean DUP was almost 3.5 times longer in EOP than in AOP patients (18.7 ± 6.2 months vs. 5.4 ± 3.1 months, p = 0.0027) (Table 7).
Taken from Amminger et al. 2011, Langeveld et al. 2012, Schimmelmann et al. 2007, Pencer et al. 2005, and Ballageer et al. 2005.
DUP, duration of untreated psychosis; GAF, Global Assessment of Functioning; NOS, not otherwise specified.
Baseline predictors of outcomes
Table 8 summarizes the baseline predictors of outcomes after 1–4 years of follow-up as reported by individual studies. More positive and negative symptoms at baseline significantly predicted a worse illness severity at follow-up. Fewer negative symptoms at baseline significantly predicted remission and a better social functioning at follow-up, and fewer positive symptoms at baseline significantly predicted a better quality of life after 1–4 years.
Higher scores reflect better functioning.
Quality of life at follow-up also inversely associated with positive and negative symptoms at follow-up (Pencer et al. 2005).
CGAS, Childrens Global Assessment Scale; CGI-S, Clinical Global Impressions Scale-Severity, GAF, Global Assessment of Functioning; SASS, Social Adaptation Self-evaluation Scale; SCS, Strauss Carpenter Prognostic Scale.
A better premorbid adjustment significantly predicted remission, and more favorable outcomes on global function, social function, and quality of life at follow-up, whereas worse premorbid adjustment significantly predicted more negative symptoms and worse illness severity at follow-up.
Exploratory correlational analyses of associations among diagnosis, age at onset of illness, severity, and the change in psychopathology and global functioning
Age at illness onset and age at study baseline
First episode versus mixed first /multi-episode samples had a higher mean age at onset (n = 10, 15.2 ± 0.9 years vs. n = 7, 11.5 ± 2.4 years, r2 = 0.54, p = 0.0013) and a higher mean age at baseline (n = 15, 16.0 ± 2.0 years vs. n = 10, 14.7 ± 1.6 years, r2 = 0.11, p = 0.026). A higher baseline PANSS total score was associated with higher age at illness onset (ρ = 1.0, p < 0.0001). Psychosis NOS and affective disorders diagnosed at entry were associated with a lower mean age at onset (both ρ = −1.0, p < 0.0001), as well as a lower mean age at baseline (psychosis NOS: ρ = −0.86, p = 0.0065; affective psychosis: ρ = −1.0, p < 0.0001). By contrast, a diagnosis of schizoaffective disorder (ρ = 0.54, p = 0.0472) or schizophreniform disorder (ρ = 0.68, p = 0.0103) were associated with a higher age at illness onset.
DUP
There was a trend association of first episode versus mixed samples with a shorter mean DUP (n = 9, 10.9 ± 8.4 months vs. n = 3, 32.1 ± 13.8 months, r2 = 0.52, p = 0.052).
Baseline psychopathology
A higher baseline PANSS total subscore was associated with a higher baseline PANSS positive (ρ = 1.0, p < 0.0001) and PANSS general (ρ = 0.9, p = 0.0374), but not PANSS negative subscore (ρ = 0.48, p = 0.233). There was a trend of male sex (n = 27) associated with higher baseline PANSS total (p = 0.072) and PANSS positive symptom scores (p = 0.057). A diagnosis of affective psychosis was associated with a higher GAF/CGAS score at baseline (ρ = 1.0, p < 0.0001).
Change in psychopathology and functioning
A greater PANSS total score improvement (decrease) was associated with higher baseline PANSS total score (ρ = −0.86, p = 0.0137) and PANSS positive subscore (ρ = −0.86, p = 0.0137) as well as with a greater PANSS positive subscore reduction (ρ = 0.96, p = 0.0005).
Greater PANSS positive subscore improvement (decrease) was associated with higher baseline PANSS total scores (ρ = −0.93, p = 0.0025) and all baseline PANSS subscores (PANSS positive: ρ = −0.93, p < 0.0001; PANSS negative: ρ = −0.69, p = 0.0289; and PANSS general: ρ = −0.83, p = 0.0416). Greater PANSS negative subscore improvement (decrease) was correlated with a higher baseline PANSS negative subscore (ρ = −0.72, p = 0.0186) and greater PANSS positive subscore reduction (ρ = 0.70, p = 0.0251). Moreover, a diagnosis of schizophrenia was significantly associated with less PANSS negative subscore reduction (ρ = 0.94, p = 0.0048).
Greater CGI-S score improvement was associated with a higher baseline CGI-S score (ρ = −1.0, p < 0.0001). Greater improvements in global functioning (CGAS/GAF) scores were associated with shorter DUP (ρ = 1.0, p < 0.0001) and a greater improvement (decrease) in PANSS positive (ρ = −1.0, p < 0.0001) and PANSS negative subscores (ρ = −1.0, p < 0.0001).
Discussion
In the current review that included 35 articles representing 28 samples of youth with early onset, predominantly schizophrenia-spectrum psychosis (89.0%), the analyzed samples had a mean age of 15.6 years at baseline and a mean age at illness onset of 14.5 years, 62.3% were males, and most of the patients were treated with antipsychotics at study baseline. The main findings of this systematic review include: 1) Youth were moderately to markedly ill, with similar levels of positive and negative symptoms at baseline. 2) Hallucinations (70.3%), predominantly auditory (81.9%), and delusions (77.5%) were very common, followed by thought disorders (65.5%), bizarre/disorganized behavior (52.8%), and flat or blunted affect/negative symptoms (52.3%/50.4%). 3) The rate of comorbidity was high, including high rates of PTSD, ADHD and/or disruptive behavior disorders, and substance abuse/dependence. 4) The proportion of patients with fully developed syndromes of schizophrenia, bipolar disorder, or depressive disorder increased over time, whereas psychosis NOS and, especially, schizophreniform disorder decreased; but diagnostic shifts were not significant, likely because of the small samples. 5) All mean psychopathology and global functioning scores improved significantly during a mean follow-up of 2.2 years. 6) Schizophrenia was associated with less improvement in negative symptoms. 7) PANSS positive and negative symptoms scores and changes were intercorrelated, and PANSS total score and change were correlated with PANSS positive and general, but not with negative subscale scores. 8) DUP was longer in EOP than in AOP samples studied in the same context (same study methodology), and longer DUP predicted less improvement in global functioning; better premorbid adjustment predicted remission, and more favorable outcomes regarding global function, social function, and quality of life, whereas worse premorbid adjustment predicted more negative symptoms and higher illness severity at follow-up.
Clinical characteristics of EOS patients
The preponderance of males (62%) is in accordance with a large Australian study of first episode psychosis, 1997–2000 (Early Psychosis Prevention and Intervention Centre [EPPIC]) (Amminger et al. 2006), and meta-analytic evidence of a rate ratio for males:females of 1.4:1 for lifetime incidence of schizophrenia (McGrath et al. 2008). A register-based study of the incidence of EOP in Denmark (Okkels et al. 2013), reported a comparable male percentage of 65% in the earlier time period 1971–1993, but an equal gender distribution in the later period 1994–2010, indicating a possible historical shift toward a more equal male:female ratio among EOS patients that was not replicated in our study of samples published from 1990 to 2014. The mean age at baseline in our sample (15.6 years) is similar to the one found by Okkels et al. (15.8 years at first diagnosis).
The EOP patients were moderately to markedly ill at baseline and had serious problems in global functioning. The mean CGI-S score was 5.0, “markedly ill,” and the mean PANSS total score was 84 (corresponding to “moderately” to “markedly ill” on the CGI-S scale according to Leucht and colleagues (2005). The mean GAF/CGAS score at baseline was a low 34, reflecting that these patients were seriously functionally impaired.
Our pooled data on specific psychotic symptoms confirm the general understanding that hallucinations in EOP patients are mostly auditory. Hallucinations of any kind were reported in 70% of the patients, whereas a subset of studies found auditory hallucinations in 82%, and delusions (primarily persecutory) in 77%. The frequencies of hallucinations are largely comparable with that reported in a study by Biederman et al. (2004), who found 85% of youth with broadly defined psychosis to experience hallucinations. However, our findings suggest slightly lower frequencies of specific hallucinations than in older studies of more narrowly defined early-onset schizophrenia (Kolvin et al. 1971; Russell et al. 1989; Green et al. 1992). The frequency of delusions identified in our review was higher than in older EOP studies, which reported delusions in 54–63% of youth (Kolvin et al. 1971; Russell et al. 1989; Green et al. 1992; Biederman et al. 2004). We found a predominance of delusions of persecution and reference, similar to the finding in a study of adults with first episode schizophrenic psychosis (Ellersgaard et al. 2014). Patients with EOP are thought to have more disorganization and more formal thought disorder than AOP patients (Hafner and Nowotny 1995). On average, 65% of patients with EOP had formal thought disorder and 36% had disorganized/pressured speech. The frequency of formal thought disorder was close to the frequency reported by older studies on EOS (Kolvin et al. 1971; Russell et al. 1989).
Negative symptoms were present in half of the patients, and the level of negative symptoms was moderate at baseline. The prevalence of clinically relevant negative symptoms in adults is estimated at ∼15% in first episode patients and higher in chronic schizophrenia (Foussias and Remington 2010). Baseline data from the large Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study showed prominent negative symptoms in 40% of participants with chronic schizophrenia (Rabinowitz et al. 2013). One half of this subgroup showed prominent negative symptoms without prominent positive symptoms, and the other half showed prominent negative symptoms plus prominent positive symptoms. Compared with these percentages in AOP patients, we found higher proportions of EOP patients with negative symptoms (50–52%), indicating a possible reason for EOS patients to have the potential for poorer outcomes, especially as negative symptom levels tended to remain high at follow-up, and because higher negative symptoms have been found to predict greater overall psychopathology in adults (Fusar-Poli et al. 2015). The rate of comorbidity was high, and a total of 32% of patients had a substance abuse disorder. In the studies comparing first episode EOP and AOP patients, comorbid substance abuse was reported in almost 50% of EOP and 60% of AOP patients (Ballageer et al. 2005; Pencer et al. 2005; Schimmelmann et al. 2007; Amminger et al. 2011; Langeveld et al. 2012). The overall percentage of patients with substance abuse (32%) is similar to that in the Spanish Child and Adolescent First-Episode Psychosis Study (CAFEPS) of youth with a first episode psychotic episode, where 33.6% of the patients used substances at baseline (Baeza et al. 2009). Substance use may influence the onset and course of psychosis. Cannabis use might exert adverse effects on brain maturation triggering an earlier age at onset of psychosis (Large et al. 2011; Schimmelmann et al. 2011; Stefanis et al. 2013), and ongoing substance use may be associated with negative outcomes (Baeza et al. 2009; Bertelsen et al. 2009; Sara et al. 2014).
An overall high rate of comorbid psychiatric disorders was also reported in other studies of children and adolescents with schizophrenia (Ross et al. 2006; Driver et al. 2013). A total of 99% of childhood-onset patients in the study by Ross et al. (2006) had at least one lifetime nonpsychotic DSM-IV-axis 1 disorder, most often ADHD (84%), whereas PTSD was rare. Although we found a lower proportion with ADHD and/or disruptive behavior disorder diagnoses (33.5%), the high level of PTSD diagnoses (34%) in the pooled samples supports the notion that trauma plays a role in the pathogenesis of EOS as well as in individuals with psychotic symptoms (Harley et al. 2010; Varese et al. 2012; Dvir et al. 2013; Aas et al. 2014; Daglas et al. 2014; Li et al. 2014). The documentation of high rates of PTSD in EOS patients has important clinical implications, especially in the light of new evidence that standard protocols for PTSD treatment are effective, safe, and feasible in patients with psychotic disorders (van den Berg et al. 2015). However, although OCD has been recognized as a relevant comorbidity in people with schizophrenia (Bottas et al. 2005; Cunill et al. 2009), only two studies provided data on comorbid OCD, highlighting that more detailed information should be collected and reported in future phenomenological studies.
Diagnostic trajectories and symptomatic and functional outcomes in EOS
All mean psychopathology and global functioning ratings improved significantly over time. Recent studies from early intervention services suggest that early-onset patients might have an equally good or even better outcome than adult-onset patients (Schimmelmann et al. 2007; Amminger et al. 2011), at least in settings with comprehensive early recognition and outreach efforts (Schimmelmann et al. 2013). However, these services and studies did not include children, but only adolescents ≥15. Therefore, the generalization to EOP samples with prepubertal patients in whom psychosis interrupts maturation and developmental processes very early is unclear. Regarding the associations among diagnoses, age, and age of onset of illness, our results were somewhat surprising, because the less well-defined diagnoses might be expected to be more common in the younger patients, as these diagnoses are the least stable (Chang et al. 2009; Salvatore et al. 2009). These results most likely reflect differences in the selection of samples with different diagnoses for different age groups. However, the early age of onset of affective psychosis could indicate that the co-occurrence of psychotic and affective symptoms facilitated the early recognition of psychosis. In our study, the diagnostic trajectories did show a pattern of change from nonspecific to more specific diagnoses and a decline in the proportion of patients with schizophrenia spectrum diagnoses, whereas the proportion of patients with diagnoses of affective disorders increased. These findings are in line with a review reporting common misclassification of affective or atypical psychotic disorders as schizophrenia in childhood (Driver et al. 2013). Regarding diagnostic shifts during follow-up in studies of first episode adult patients, some reported a predominant shift from nonaffective psychosis to affective psychosis (Salvatore et al. 2009), whereas others reported a shift in the opposite direction (Chang et al. 2009). In both cases, the data illustrate the diagnostic challenges in clinical care as well as early intervention services for youth patients. Professionals are usually trained to diagnose fully developed syndromes, such as schizophrenia and bipolar disorder; however, the early stages of these conditions are often difficult to categorize without view of a longer-term trajectory of symptomatology.
Predictors of severity and outcome of illness in the first years after treatment initiation
We did not find significant effects of age, age at onset of illness, and gender on course and outcome of EOS. Perhaps the prognostic effects of age and gender were diluted by unadjusted effects of premorbid/comorbid problems and disorders. A recent systematic review of prospective and retrospective longitudinal observational studies (as opposed to intervention studies) of EOS found no predictive effects of gender and age at onset of illness on outcome in multivariate models (Diaz-Caneja et al. 2015), which is in line with the literature showing inconsistent findings in this area.
For our pooled samples, we found that the severity of positive symptoms at baseline, the severity and the persistence of negative symptoms, longer DUP, and poorer premorbid adjustment each predicted a worse outcome of illness measured at one or several domains of outcome (symptom severity, remission, global function, social function and/or quality of life). These findings are consistent with results from adult studies (Fenton and McGlashan 1991; Foussias and Remington 2010; Moller et al. 2010; Carbon and Correll 2014), and with the results from a recent review showing that premorbid difficulties, greater symptom severity (especially negative symptoms) at baseline, a diagnosis of schizophrenia, and a longer DUP predicted worse outcomes in all or several important areas (clinical, functional, cognitive, neuroimaging) in EOS patients (Diaz-Caneja et al. 2015).
The findings that DUP was longer in EOP than in AOP, and that longer DUP as well as poorer premorbid adjustment predicted a less favorable outcome emphasize the importance of early intervention strategies in order to improve long-term outcome of EOS (Correll et al. 2010; Chang et al. 2012; Hill et al. 2012). The severe delay in recognition of psychosis in youth patients may be explained by the relative lack of specificity in the very early stages of psychosis; insidious onset; presence of comorbid, nonpsychotic disorders; and lack of clinical training in – or focus on – the identification of psychotic disorders in the services for youth patients (Schimmelmann et al. 2013). Although a review of 28 studies of adult patients with first episode psychosis reported a much higher mean DUP of 14.2 months (Boonstra et al. 2012), even longer DUPs of up to 7 years have been reported in studies of EOP patients (Russell et al. 1989; Alaghband-Rad et al. 1995; Hafner and Nowotny 1995; Maziade et al. 1996; Eggers and Bunk 1997). A reduction of DUP may be of particular importance in youth, because untreated psychosis obviously interferes with the normative developmental processes in this age group.
We did not study the effects of various treatments on outcome of illness, but clearly, various treatments received during follow-up, and adherence or nonadherence to such treatments will be relevant mediators of outcome. For example, a review of clinical predictors of therapeutic response and remission, focusing on adults with first episode schizophrenia spectrum disorder, found reduced odds for response and remission to be associated with poor premorbid adjustment, longer DUP and illness duration, lower functional status, substance abuse, antipsychotic treatment nonadherence, lack of an early response to antipsychotic medication, and early side effects at therapeutic doses (Carbon and Correll 2014).
The results from this systematic review have to be interpreted within its limitations. Most importantly, the included studies were heterogeneous in design, sampling, assessments, duration of follow-up, and the reporting of specific data. Moreover, both the number of studies and the corresponding number of patients contributing data for individual outcomes were quite limited in most cases and often did not provide sufficient data for inferential statistics. Overall, the generalizability of the results and the ability to identify reliable clinical correlates were reduced. Further, these limitations make the exploratory analyses vulnerable to selection biases and unadjusted confounding. Additionally, despite neurobiological overlap between affective and nonaffective psychotic disorders, we chose to only include only studies with >50% nonaffective psychosis in this systematic review. This decision was made because we aimed at reviewing symptoms and the prognosis of youth with nonaffective psychosis attempting to avoid biasing results toward potentially more positive outcomes by including a majority of patients diagnosed with bipolar or major depressive disorder with psychotic features during the first episode, who may not have a predominantly psychotic disorder subsequently. Finally, outcomes are influenced by heterogeneous types of treatment that was received in naturalistic settings in the included studies. Therefore, controlled longitudinal studies and naturalistic studies collecting detailed information about specific types of treatment and their relationship to outcome are required to further inform the field. The present review highlights the need for research of larger samples of young people with early-onset schizophrenia spectrum disorders with a more detailed and comprehensive measurement of outcomes, using the reviewed outcomes as an example and minimum requirement.
Conclusions
This comprehensive review of clinical studies published from 1990 to 2014, presenting data on the clinical characteristics, clinical correlates and outcome of first-episode nonaffective psychosis in children and adolescents largely confirmed currently held notions based on more limited sample sizes. EOS patients are characterized by substantial impairment from significant levels of positive and negative symptoms; disorganized behaviour; pre- and comorbid conditions, including PTSD, ADHD, and/or disruptive behavior disorders and substance abuse disorders; long DUP; and poor premorbid adjustment. Both longer DUP and poorer premorbid adjustment were associated with poorer illness outcome, suggesting areas for early intervention to improve outcomes in EOP youth.
Clinical Significance
The high prevalence of negative and disorganized symptomatology in EOS patients in the context of co-occurring nonpsychotic mental disorders may mask the emergence of psychosis and thereby explain the higher risk of delayed identification and treatment of EOS. These findings emphasize the need for early detection and treatment of psychosis in youth. The comorbid conditions of ADHD/disruptive behavior disorders, substance abuse, and PTSD are treatable conditions, which may be helpful to target, especially in youth with signs of emerging psychosis. More prospective studies and longer-term studies are needed in order to identify the best early identification and treatment strategies to improve outcome and functioning in youth with EOS.
Footnotes
Disclosures
Drs. Stentebjerg-Olesen, Pagsberg, and Jeppesen have no conflicts of interest to report. Dr. Fink-Jensen has received grant support from Novo Nordisk A/S. Dr. Correll has been a consultant and/or advisor to or has received honoraria from: Bristol-Myers Squibb (BMS), Eli Lilly, Genentech, Gerson Lehrman Group, IntraCellular Therapies, Janssen/J&J, Lundbeck, MedAvante, Medscape, Otsuka, Pfizer, ProPhase, Roche, Sunovion, Supernus, and Takeda. He has received grant support from the American Academy of Child and Adolescent Psychiatry BMS, Janssen/J&J, National Institute of Mental Health (NIMH), Novo Nordisk A/S, Otsuka, Takeda, and the Thrasher Foundation.