
Abstract
Objective:
No studies in Europe have assessed the extent of nonmedical attention-deficit/hyperactivitiy disorder (ADHD) medication use among adolescents, while also, in Europe, prescribing of these medicines has increased. Our objective was to study the prevalence and motives for nonmedical ADHD medication use among secondary school students in the Netherlands.
Methods:
Adolescent students 10–19 years of age from six secondary schools were invited to complete an online survey on use of ADHD medication, tobacco, alcohol, and drugs. Nonmedical ADHD medication use was defined as self-reported use without a prescription during the previous 12 months.
Results:
Survey data were available for 777 students (15% response rate). The overall proportion of students self-reporting nonmedical ADHD medication use was 1.2% (n = 9), which represented almost 20% of the adolescents who reported ADHD medication use (n = 49). Most adolescents reported self-medication or enhancing study performance as motives for ADHD medication use.
Conclusions:
The proportion of the study sample reporting nonmedical ADHD medication use in our study is lower compared with that in previous research conducted in the United States and Canada; however, on a population-based level, there might be a considerable proportion of recreational users.
Introduction
S
Methods
We conducted a cross-sectional study among secondary school students in the province of Utrecht, the Netherlands (1,200,000 inhabitants, 7% of the total Dutch population). From the 78 secondary schools in the province of Utrecht that were approached to join this study, 6 schools accepted our invitation to participate in the study during the specified time period (April–June 2014). Approximately 5200 adolescent students 10–19 years of age from these six secondary schools in the Utrecht area were invited through their school's email service or virtual learning system to complete an online survey on use of ADHD medication, alcohol, and drugs. The sample included both schools located in smaller towns and schools located in larger cities in the province of Utrecht. Participation was voluntary and anonymous. Monetary incentive was offered upon survey completion: One tablet computer and three giftcards (15€) were raffled among participants. The study protocol was approved by the Institutional Review Board of the Division of Pharmacoepidemiology and Clinical Pharmacology, Utrecht University.
Self-reported ADHD medication use and motives for use were assessed through an online questionnaire containing multiple choice questions. The survey included sociodemographic questions (age, gender, ethnic background, and secondary school educational level), use of (both medical and nonmedical) ADHD medication during the previous 12 months, motives for use, and questions about use of alcohol, drugs, and tobacco.
Medical use of ADHD medication was defined as self-reported use during the previous 12 months with a physician's prescription. Nonmedical use of ADHD medication was defined as self-reported use without a prescription during the previous 12 months. Recreational drug use during the previous 12 months was defined as at least one episode of use of any illicit drug, such as cannabis, methyleendioxymethamfetamine (MDMA or XTC), gamma-hydroxybutyric acid (GHB), and cocaine. Alcohol consumption was defined as consuming any alcoholic drink(s) during the previous 12 months. Tobacco use was defined as using any type of tobacco.
The survey was online during different time slots in the participating schools between April 11 and July 1, 2014. Data were collected using LimeSurvey, and data analysis was performed using IBM SPSS for Windows, version 20.0. Descriptive statistics were calculated. Chi-square tests were used to compare student substance use between medication use groups (no use vs. the other two groups [medical use, nonmedical use]). All tests were two tailed and p values <0.05 were considered statistically significant.
Results
In total, 1376 students opened the link to the survey of which 793 completed the survey. During the data cleaning process 16 questionnaires were rejected because of missing data or irrelevant answers, resulting in a final data set comprising data from 777 students (15% response of the total of 5200 students in the participating schools). The general characteristics are shown in Table 1: 60% were females, and the sample mainly consisted of native ethnic Dutch students (96%). The proportion of non-natives in the general Dutch population is higher (∼20%), and there seem to be more highly educated students in our sample than in the Dutch student population in general (Centraal Bureau voor de Statistiek 2015a,b).
Based on country of birth.
Self-reported use of any prescription medication.
ADHD, attention-deficit/hyperactivity disorder.
The overall proportion of the study population reporting ADHD medication use during the previous 12 months was 6.3% (n = 49). Users were classified as medical and nonmedical users: 82% of the ADHD medication users reported medical use (they received a prescription) (n = 40, 5.1% of the total study population) and almost 20% reported ADHD medication use without a prescription (n = 9, 1.2% of the total study population).
Both medical and nonmedical users of ADHD medication more often reported use of tobacco, alcohol, and recreational drugs than did nonusers of ADHD medication (p < 0.05) (Table 2).
Compared with other two groups.
Self-reported use of any prescription medication.
ADHD, attention-deficit/hyperactivity disorder.
Figure 1 shows the motives for medical and nonmedical use of ADHD medication. Most adolescents reported a medical reason or enhancing study performance as reasons for ADHD medication use. Further, motives such as to relieve stress or to feel better were mentioned.
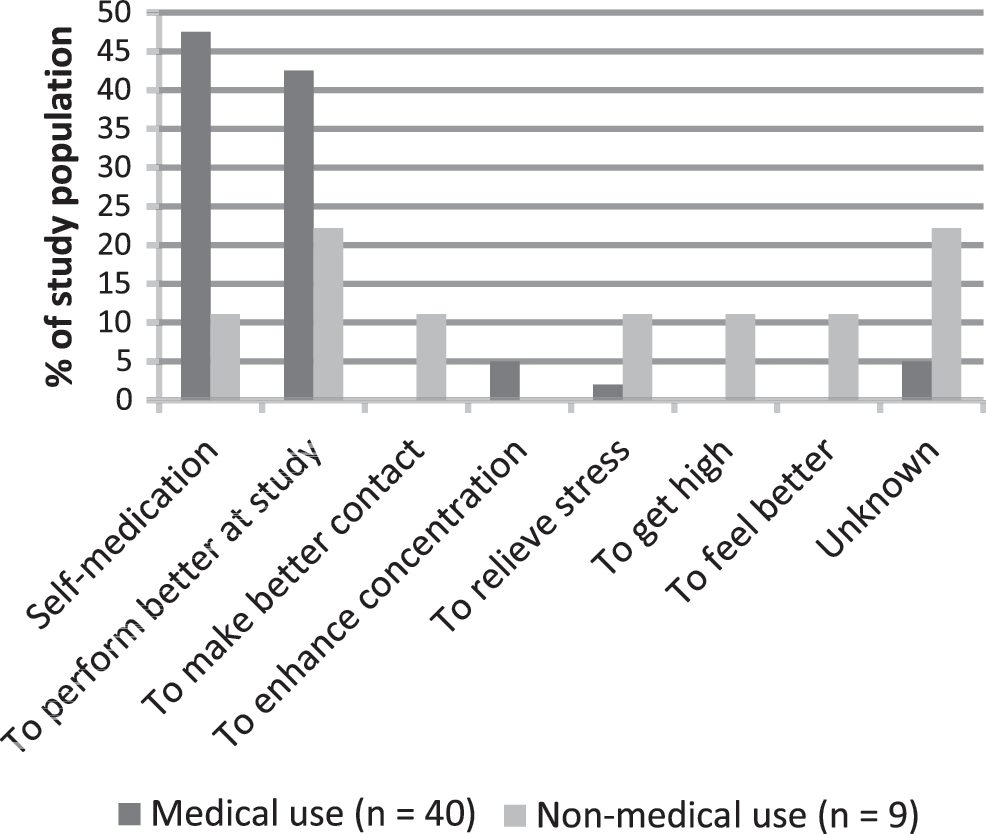
Primary motives for use.
Discussion
To our knowledge, this is the first study in the Netherlands assessing nonmedical ADHD medication use among adolescent students. In our sample of 777 adolescent secondary school students, almost one fifth of the ADHD medication users (1.2% of the total study population) reported ADHD medication use without having had a physician's prescription. The overall proportion of nonmedical use found in our study was lower than in studies previously performed in Canada and the United States (Teter et al. 2003, 2005; Boyd et al. 2006; Poulin 2007; Young et al. 2012). These studies also used anonymuous self-report web surveys for data collection and reported a 2–7% prevalence for past year nonmedical stimulant use among undergraduate students in United States grades 7–12 (ages 12–18) (Teter et al. 2005; Boyd et al. 2006; Young et al. 2012). In line with previous survey studies conducted in the United States (Teter et al. 2003; McCabe et al. 2007), nonmedical users of ADHD medication also seemed to more often report use of other substances such as alcohol, tobacco, and recreational drugs. Adolescents reported several reasons for nonmedical use of ADHD medication. Because of the low prevalence of nonmedical ADHD medication use, this was a very small group.
This is the first study in the Netherlands describing nonmedical use of ADHD prescriptions among adolescents. Through online assessment, we were able to collect data from a substantial population of young adolescents in a relatively short period. Moreover, the nature of online surveys ensures perceived and actual anonymity of the participant, decreasing potential sources of bias (peer pressure or socially desired answers) and incrementing level of self-disclosure. However, because this study relied completely on self-report, certain well-known forms of bias inherent to self-report (such as reliability of answers resulting in over- or underreport) can never be excluded completely, and must always be kept in mind when interpreting self-reported outcomes. The proportion of natives and more highly educated students in our sample seems to be higher than the Dutch student population in general (Centraal Bureau voor de Statistiek 2015a,b). Generalizibility might, therefore, be a problem, as the majority of the included students were of native (Dutch) origin, and we only included participants in the region of Utrecht, although we have included schools located in smaller towns in this provence and schools located in the (larger) cities, reflecting different demographic areas. However, cultural and socioeconomic diversity in the sample may be limited, as we also mainly included students at higher educational levels. The prevalence of nonmedical use seemed to be highest among non-natives, although numbers are small. Therefore, a future study should also include schools from other areas in the Netherlands (and pay specific attention to lower edecuational levels) to gain insight into the nationwide prevalence of nonmedical stimulant use and to study differences among students from different backgrounds.
Conclusions
In conclusion, the proportion of secondary school students in our sample reporting nonmedical ADHD medication use in the past year was 1.2%. This is almost 20% of ADHD medication users (both medical and nonmedical users) in our population; therefore, on a population-based level, there might be a considerable proportion of recreational users. We have shown that those students using ADHD medication for nonmedical purposes were also more likely to use alcohol, tobacco, and other drugs. High school students might use ADHD medication illicitly for many reasons. More research is needed to quantify differences in use in different populations.
Clinical significance
This is the first study in the Netherlands describing the prevalence of nonmedical use of ADHD prescriptions among adolescent secondary school students. Almost 20% of the ADHD medication users in our study were recreational users (n = 9, 1.2% of the study population). Students using ADHD medication for nonmedical purposes were also more likely to use alcohol, tobacco, and other drugs.
Footnotes
Disclosures
No competing financial interests exist.