
Abstract
Objective:
Irritability in disruptive mood dysregulation disorder (DMDD) may be associated with a biased tendency to judge ambiguous facial expressions as angry. We conducted three experiments to explore this bias as a treatment target. We tested: 1) whether youth with DMDD express this bias; 2) whether judgment of ambiguous faces can be altered in healthy youth by training; and 3) whether such training in youth with DMDD is associated with reduced irritability and associated changes in brain function.
Methods:
Participants in all experiments made happy versus angry judgments of faces that varied along a happy to angry continuum. These judgments were used to quantify a “balance point,” the facial expression at which a participant's judgment switches from predominantly happy to predominantly angry. We first compared balance points in youth with DMDD (n = 63) versus healthy youth (n = 26). We then conducted a double-blind, randomized controlled trial of active versus sham balance-point training in 19 healthy youth. Finally, we piloted open, active balance-point training in 14 youth with DMDD, with 10 completing an implicit functional MRI (fMRI) face-emotion processing task.
Results:
Relative to healthy youth, DMDD youth manifested a shifted balance point, expressed as a tendency to classify ambiguous faces as angry rather than happy. In both healthy and DMDD youth, active training is associated with a shift in balance point toward more happy judgments. In DMDD, evidence suggests that active training may be associated with decreased irritability and changes in activation in the lateral orbitofrontal cortex.
Conclusions:
These results set the stage for further research on computer-based treatment targeting interpretation bias of angry faces in DMDD. Such treatment may decrease irritability and alter neural responses to subtle expressions of happiness and anger.
Introduction
S
Three factors inform this work. First, as will be elaborated, prior research suggests that youth with conduct problems respond to a computer-based treatment targeting a form of HIB (Penton-Voak et al. 2013). Second, as will also be detailed below, youth with chronic irritability have deficits in labeling face emotions. Finally, chronic, severe irritability in youth shares concurrent, longitudinal, and genetic associations with depression and anxiety (Brotman et al. 2006; Stringaris et al. 2009; Leibenluft 2011; Copeland et al. 2014; Stringaris et al. 2014; Savage et al. 2015) for which interpretation biases of ambiguous cues are established targets for cognitive bias modification training (Hallion and Ruscio 2011; MacLeod and Mathews 2012).
HIB has been associated with irritability-related phenomena such as dispositions toward anger (Wilkowski and Robinson 2010) and verbally or physically aggressive reactions (Crick and Dodge 1996; Orobio de Castro et al. 2002). Targeting HIB, Penton-Voak and colleagues (2013) conducted two randomized controlled trials of sham versus active computer-based training to shift participants' judgments of ambiguous facial expressions from “angry” to “happy.” Active training was associated with decreased anger in healthy young adults and aggression in youth with conduct problems, measured by blinded self and youth program staff ratings.
Irritable youth with severe mood dysregulation (SMD) (Leibenluft et al. 2003), a syndrome that was defined for research purposes and formed the basis for DMDD, tend to rate themselves as more afraid of neutral faces than do youth without psychopathology (Brotman et al. 2010). SMD youth also exhibit perturbed neural and attentional responses to face emotions signifying threat (Brotman et al. 2010; Hommer et al. 2013). However, other studies report generalized labeling deficits across emotions in SMD youth, without specific hostile interpretation biases (Guyer et al. 2007; Rich et al. 2008). Therefore, although the data are somewhat mixed, prior work suggests that HIB may be present in DMDD, raising the question of whether training to reduce this bias might decrease impairing irritability.
To provide preliminary evidence on the potential utility of interpretation bias training in DMDD, we report on an open trial of such training. As context, we first demonstrated the presence of HIB in youth with DMDD, as measured by happy/angry judgments of ambiguous facial affect (Experiment 1). Next, we showed that active, but not sham, training shifted emotional judgments of ambiguous faces in healthy youth (Experiment 2). In Experiment 3A, we conducted an open trial of interpretation bias training in DMDD youth. Concurrently, we explored putative neural mechanisms for this open trial by testing post- versus pretraining responses to subtle emotional expressions in key components of the threat monitoring system; that is, the orbitofrontal cortex (OFC) and amygdala (Experiment 3B).
Methods
Methods common to all experiments
The study was approved by the National Institute of Mental Health (NIMH) Institutional Review Board. Written informed consent was obtained from parents and assent was obtained from youth. Families were paid for participation. All experiments accrued convenience samples. Inclusion criteria and assessment techniques are detailed in the supplementary material (see online supplementary material at
Experiment 1: Interpretation bias in DMDD versus healthy volunteer youth
Participants with a lifetime diagnosis of DMDD (n = 70; ages 8–18 years) and healthy volunteer (HV) youth (n = 27; ages 8–18 years) attempted to complete the interpretation bias task (IBT), with 63 DMDD and 26 HV youth providing acceptable data (see subsequent description of quality assurance; participant characteristics are given in Table 1). Lifetime rather than current DMDD was the inclusion criteria, because the goal of Experiment 1 was to identify a stable trait cognitive marker for DMDD.
Any anxiety disorder includes generalized anxiety disorder, social phobia, or separation anxiety disorder
ODD diagnoses are for comparing to the prior literature. In DSM-5, a diagnosis of DMDD precludes a diagnosis of ODD.
HV, healthy volunteer; DMDD, disruptive mood dysregulation disorder; IQ, intelligence quotient; K-SADS, Kiddie Schedule for Affective Disorders and Schizophrenia for School-Aged Children; ADHD, attention-deficit/hyperactivity disorder; ODD, oppositional defiant disorder; MDD, major depressive disorder, DSM-5, Diagnostic and Statistical Manual of Mental Disorders, 5th ed.
Parent- and self-report forms assessed irritability (Affective Reactivity Index [ARI]) (Stringaris et al. 2012), anxiety (Screen for Child Anxiety Related Disorders [SCARED]) (Birmaher et al. 1999), anger (State Trait Anger Expression Inventory, Second Edition, Child Adolescent [STAXI-2 C/A]) (Brunner and Spielberger 2009), and depression (Children's Depression Inventory [CDI]) (Kovacs 1992).
The IBT developed by coauthors K.M. and Y.B. used happy and angry face-emotion pictures (stimuli from Tottenham et al. 2009). For each identity, 15 “morphs” were created that were equally spaced on a continuum from happy to angry. Each trial consisted of a fixation cross (800–1200 ms), image presentation (200 ms), visual noise mask (200 ms), and a response screen with a question mark. The response screen remained until the participant made a forced-choice response of “angry” or “happy.” Each morph was presented three times for a total of 180 trials.
To assure engagement with the task, participants who failed to correctly identify at least 70% of the four overtly angry and happy facial expressions were excluded (one HV and seven DMDD youth; see supplementary material for determination of this threshold).
The response variable was judgment (happy or angry), and the independent variables were group (DMDD or HV) and morph (1–15). Using morph as a continuous variable, we tested between-group differences in the point at which judgments switch from predominantly happy to predominantly angry (i.e., the balance point) by fitting a four parameter logistic curve to group-level data (see online supplementary material at
In other analyses within the DMDD group, we correlated balance point with level of irritability (ARI), trait anger (STAXI-2 C/A, T scores relative to a gender and age norm), state anger (STAXI-2 C/A, T scores relative to a gender and age norm), anxiety disorder symptoms (SCARED), and depressive symptoms (CDI). Participants or their caregivers who completed these measures within 2 days of performing the IBT task were included in these analyses (n's = 41–48). To estimate individuals' balance points for this within-DMDD group analyses, we defined individual-level balance points as the inflection point of logistic curves fit to individual-level data.
Experiment 2: Active versus sham interpretation bias training in HV youth
Twenty HV youth were randomly allocated to active (n = 8) and sham (n = 12) interpretation bias training. One sham participant dropped out after allocation, because of misunderstanding participation instructions. Youth in the active or sham arm did not differ by age (mean [SD] active = 13.8 (1.7) years, sham = 14.7 [2.8] years; p = 0.38), gender (% female active = 63%, sham = 82%, p = 0.60), or intelligence quotient (IQ) (mean [SD] active = 112 [11.4], sham = 106 [5.1]; p = 0.20).
We used the training IBT (tIBT) procedure developed by coauthors I.P.V. and M.M. (Fig. 1); (Penton-Voak et al. 2013). Because they were designed for separate studies, the task in Experiment 1 (IBT) and the training tasks in Experiments 2 and 3 (tIBT) have minor differences in timing, and they differ in stimuli. They are reported here because they are closely related in that they target interpretive bias. Unlike the IBT, the tIBT used one face-identity of a prototypical male, derived from composite images of 20 male individuals from the Karolinska Directed Emotional Faces (Lundqvist et al. 1998). As in the IBT, 15 morphs on a continuum of happy to angry were generated. The tIBT included a sham and an active version. In both versions, each training session consisted of an assessment block, followed by six training blocks, and ended with another assessment block.
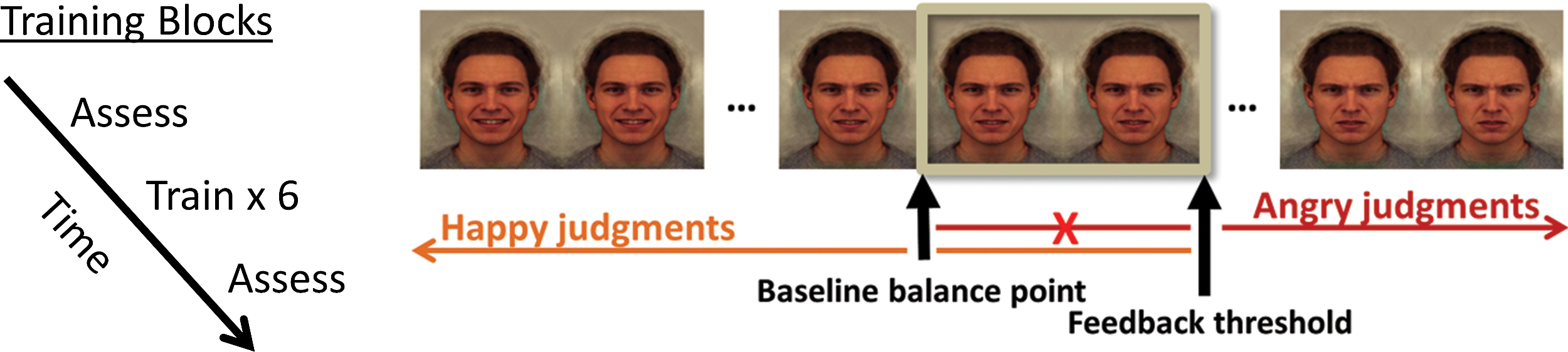
The procedure for a single training session. Training is designed to shift interpretation of ambiguous morphs bias toward happy judgments. There are two types of blocks: Assessment blocks determine balance point and training blocks shift balance point toward more happy judgments. Seven of 15 morphs are displayed here. Subjects see them in random order, but here, for presentation purposes, they are shown along a continuum of happy to angry. The balance point (i.e., the morph at which judgments switch from predominantly happy to predominantly angry) is measured during assessment blocks. During active training, feedback is given after each response. The feedback threshold is the baseline balance point, measured during the first assessment block, shifted two morphs toward the angry end of the continuum. In sham training, the feedback threshold is the same as the baseline balance point. A color version of this figure is available in the online article at
All trials consisted of a fixation cross (1500–2500 ms), image presentation (150 ms), visual noise mask (250 ms), and response screen with a question mark. The response screen remained until the participant made a response of “angry” or “happy.” In the assessment block, each morph was presented three times in random order. Data from the assessment block were used to estimate the balance point for each individual (Penton-Voak et al. 2012). The balance point was estimated as the proportion of happy responses to total responses multiplied by 15. Therefore, in this instance, the balance point was estimated from the proportion of happy responses over all morphs as in Penton-Voak et al. (2013), rather than using the more precise logistic curves used in Experiment 1. The simplified, proportion-based calculation of the balance point could be performed in real time during a training session by custom software written by us in Tcl (
In the training blocks, timing and stimulus presentation were the same as in the assessment block except that feedback was provided after each response. Active training is designed to shift the balance point (measured at the beginning of each training session, during that session's pretraining assessment block) toward happy judgments of ambiguous faces. Participants receive positive feedback for rating as happy (and negative feedback for rating as angry) two ambiguous morphs. These two ambiguous morphs were those that, during the pretraining assessment block of each training session, were nearest the balance point and had been rated as angry by the participant. Similarly, sham training provided feedback based on the balance point measured at the beginning of each session during the pretraining assessment block. In the case of sham training, the feedback was designed to reinforce, rather than shift, the current balance point. Both conditions presented each morph twice in random order during each training block. There were six training blocks consisting of 180 total trials. Both the active and sham versions of tIBT ended with a second assessment block. All participants completed four sessions of once-daily training, with any missed sessions made up with another day of training. Participants trained using their own computer or a laptop loaned to them. Participants completed the first and last training sessions at the NIMH and the middle two training sessions at home. Day 1 was defined as the first day of training. One and two weeks after the final session (Days 10 and 17), a participant's balance point was assessed with a single assessment block.
The outcome measure was change in balance point as calculated based on the posttraining assessment block from the final training session, relative to the pretraining assessment block from the first training session. As noted, this was estimated from the proportion of happy responses over all morphs as in Penton-Voak et al. (2013), rather than the more precise logistic curves. We used a linear mixed-effects (LME) model with no imputation of missing data to test the effect on the balance point of the factors group (active or sham) and session (pretraining, posttraining, 1 and 2 weeks posttraining).
Experiment 3A: Interpretation bias training in youth with DMDD
To be included in Experiment 3 (the open clinical trial), youth had to have 1) a lifetime diagnosis of DMDD and 2), at the time of enrollment into the trial, clinically significant DMDD symptoms, operationalized as a score ≥3 on the Clinical Global Impressions Scale-Severity (CGI-S) (Guy 1976) for the preceding month. Fourteen youth enrolled in the trial (Table 2). The CGI scales are clinician-rated measures of the severity (CGI-S) or improvement (CGI-I) of a specific disorder. In this instance, the CGI scales integrated clinical impressions of the severity of DMDD, whose hallmark symptom is irritability.
Any anxiety disorder includes generalized anxiety disorder, social phobia, or separation anxiety disorder.
ODD diagnoses are for comparing to the prior literature. In DSM-5, a diagnosis of DMDD precludes a diagnosis of ODD.
CGI-S, Clinical Global Impressions-Severity, caused by irritability; 3, 4, and 5 represent mild, moderate, and marked illness, respectively. A score of 3 was the minimum score required for open trial inclusion.
ARI, Affective Reactivity Index, a 12 point scale from 0 = no irritability to 12 = extreme irritability. Irritability in mental disorders characterized by severe, chronic irritability is often reported as ∼4–5 by self-report and 5–8 by parent report (Stringaris et al. 2012).
DMDD, disruptive mood dysregulation disorder; IQ, intelligence quotient; K-SADS, Kiddie Schedule for Affective Disorders and Schizophrenia for School-Aged Children; ADHD, attention-deficit/hyperactivity disorder; ODD, oppositional defiant disorder; MDD, major depressive disorder, DSM-5, Diagnostic and Statistical Manual of Mental Disorders, 5th ed.
At the start of the trial, two CGI-S measurements were obtained. One was for the month prior to training. This measurement was used to determine the severity of DMDD for inclusion. The other CGI-S covered the week prior to the start of the trial and served as a baseline for CGI-I ratings throughout the trial. The eight point version of the CGI-I (Klein et al. 1992) was used as a primary outcome measure of DMDD-related clinical improvement. CGI-I ratings compared the severity of symptoms during the week being rated to the severity of symptoms during the baseline week. The CGI scales are commonly used in psychiatric clinical trials, for which they have established utility and reliability (Berk et al. 2008). Ratings were performed by master's- or doctoral-level clinicians. Raters conducted simultaneous, independent CGI ratings of DMDD in youth participating in several studies, and met weekly to discuss the ratings to achieve consensus. No formal reliability measures were obtained for clinician CGI ratings.
Participants had no changes in their outpatient treatment regimens (medications or psychosocial treatments) for at least 2 weeks prior to training and throughout their participation. Training comprised four sessions of the active tIBT task from Experiment 2. Participants received standardized ratings by clinicians at baseline, posttraining on Day 6, and 1 week after training on Day 10. The time intervals covered by these three ratings were the month and the week prior to training, the week of training, and the week posttraining. In addition, participants and their caregivers completed the ARI immediately prior to training (Day 1), posttraining (Day 6), and 1 and 2 weeks (Days 10 and 17) posttraining.
The outcome measures were balance point, calculated as in Experiment 2, DMDD-related clinical improvement (CGI-I) (Guy 1976), and irritability (parent- and self-report ARI, analyzed separately). We used an LME model to test any change in the repeating measures, with no imputation of missing data, participant as a random factor, and session as a fixed factor. As CGI-I scores reflect a change, we used one-sample two-tailed t tests of CGI-I scores centered on 5, a score corresponding to no clinical change. Exploratory Spearman's correlations were conducted between change in balance point after training and the CGI-I and ARI measures.
Experiment 3B: Amygdala and OFC responses to subtle affect after interpretation bias training in DMDD
During each of two fMRI scanning sessions, 10 of the 14 participants from Experiment 3A completed a task adapted from Kim et al. (2012) before and after training (see online supplementary material at
Regions of interest were each of the amygdalae and lateral OFC (extracted from the DKD_Desai_MPM atlas packaged with Analysis of Functional Neuroimages (AFNI) neuroimaging processing software) (Cox 1996; Desikan et al. 2006). For each participant, neural activity within each region was estimated by computing the mean percent BOLD signal change of all voxels in its volume. Because we were interested in neural responses to subtle emotional expressions, we extracted the contrast of neural activity to 50% emotional intensity relative to fixation for each of the three face-emotions. We used an LME model to test the change in posttraining versus pretraining neural response to emotion (fearful, happy, and angry), with participant as a random factor.
Results
Experiment 1: Interpretation bias in DMDD versus HV youth
Accuracy of labeling the two morphs on each extreme of the happy–angry continuum did not differ between groups (mean [SD] accuracy HV = 88.8 [6.8]%, DMDD = 89.9 [7.6]%; t[52.1] = 0.66, p = 0.51). Relative to HV, DMDD youth required less angry affect in morphs to switch their judgments from predominantly happy to predominantly angry (b[SE] balance point HV = 7.56 [0.10]; DMDD = 7.27 [0.07]; t[87] = 2.39, p = 0.017; d = 0.51; a “medium” effect; Cohen 1992). When we analyzed each of the four face-identities presented in the IBT separately, the difference appeared to be driven by an angry judgment bias in DMDD to one male face-identity (p < 0.001), but not to the three others (p's > 0.1) (Fig. 2).
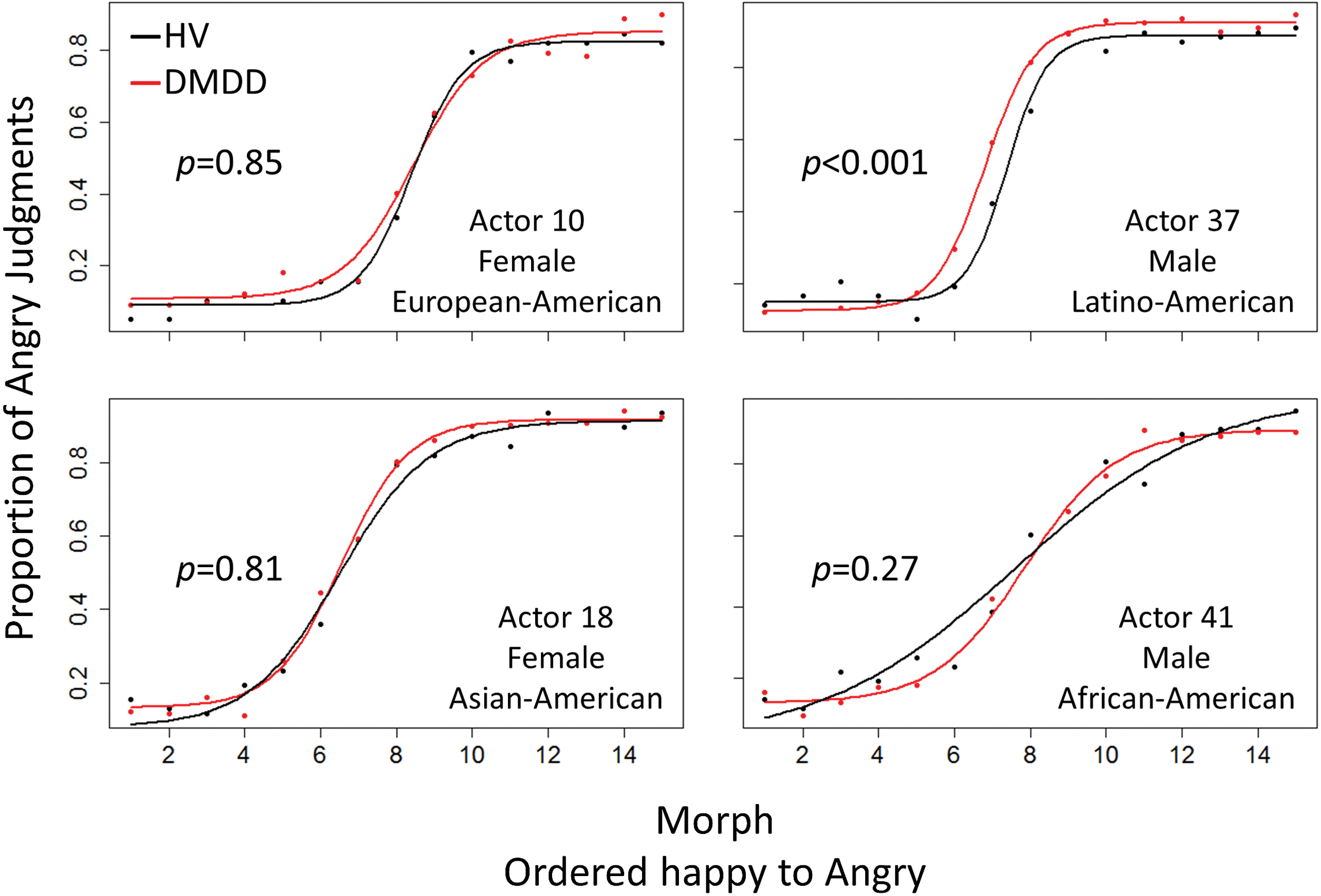
Relative to healthy volunteer (HV) youth (n = 26), disruptive mood dysregulation disorder (DMDD) youth (n = 63) have a bias toward judging ambiguous morphs as angry for the male face in the upper right panel (p < 0.001). Mean proportions of angry responses are plotted against facial morphs, ordered from happy to angry. For each group, solid lines represent the fitted four parameter logistic curves. A DMDD bias toward judging ambiguous morphs as angry is indicated by a leftward shift of the red curve relative to the black curve. Note that judgments differ by face-identity. Ethnicity descriptions and pictures of each actor can be found at
Within the DMDD group, individual balance point estimates did not differ by gender (t[52.7] = 0.59, p = 0.56) or age (r = 0.16, p = 0.20). Exploratory correlations did not detect associations between balance point and any self or parent measures of irritability, anxiety, depression, or anger.
Experiment 2: Active versus sham interpretation bias training in HV youth
The two groups did not differ in pretraining balance point (b[SE] active group = 7.0 [0.77] versus sham group = 7.03 [1.03]; t[17] = 0.01, p = 0.99]. The balance point of HV youth in the sham condition did not change, with the balance point remaining reliably consistent across all four training sessions (intraclass correlation coefficient ICC[2,1] = 0.76, F[10,30] = 15, p < 0.001) (Fig. 3). However, in the active group only, the balance point increased (i.e., shifted away from an angry judgment bias) after four sessions of daily active training, (b[SE] = 2.9 (0.67) morphs, t[46] = 4.4, p < 0.001). This increase was maintained at both 1 and 2 weeks after training, b(SE) = 2.5(0.79) and 2.2(0.67) morphs, respectively, p's < 0.003. Active and sham balance points differed at each post-training interval (p's < 0.005) (Fig. 3).

Interaction plot of active (n = 8) versus sham (n = 11) double- blind, randomized controlled trial of training in healthy volunteer (HV) youth. Asterisks represent p < 0.01 from the linear mixed-effects model parameter estimate t tests between the two groups at the sessions indicated. Error bars show standard error.
Experiment 3A: Interpretation bias training in youth with DMDD
In 14 youth with DMDD, the pretraining balance point was b(SE) = 7.37(0.47) morphs. After four sessions of daily training, balance point increased (away from an angry judgment bias) by b(SE) = 2.25(0.41) morphs. This increase was maintained 1 and 2 weeks after training, b(SE) = 2.16(0.41) and 2.54(0.41) morphs, respectively, p's < 0.001 (Fig. 4).
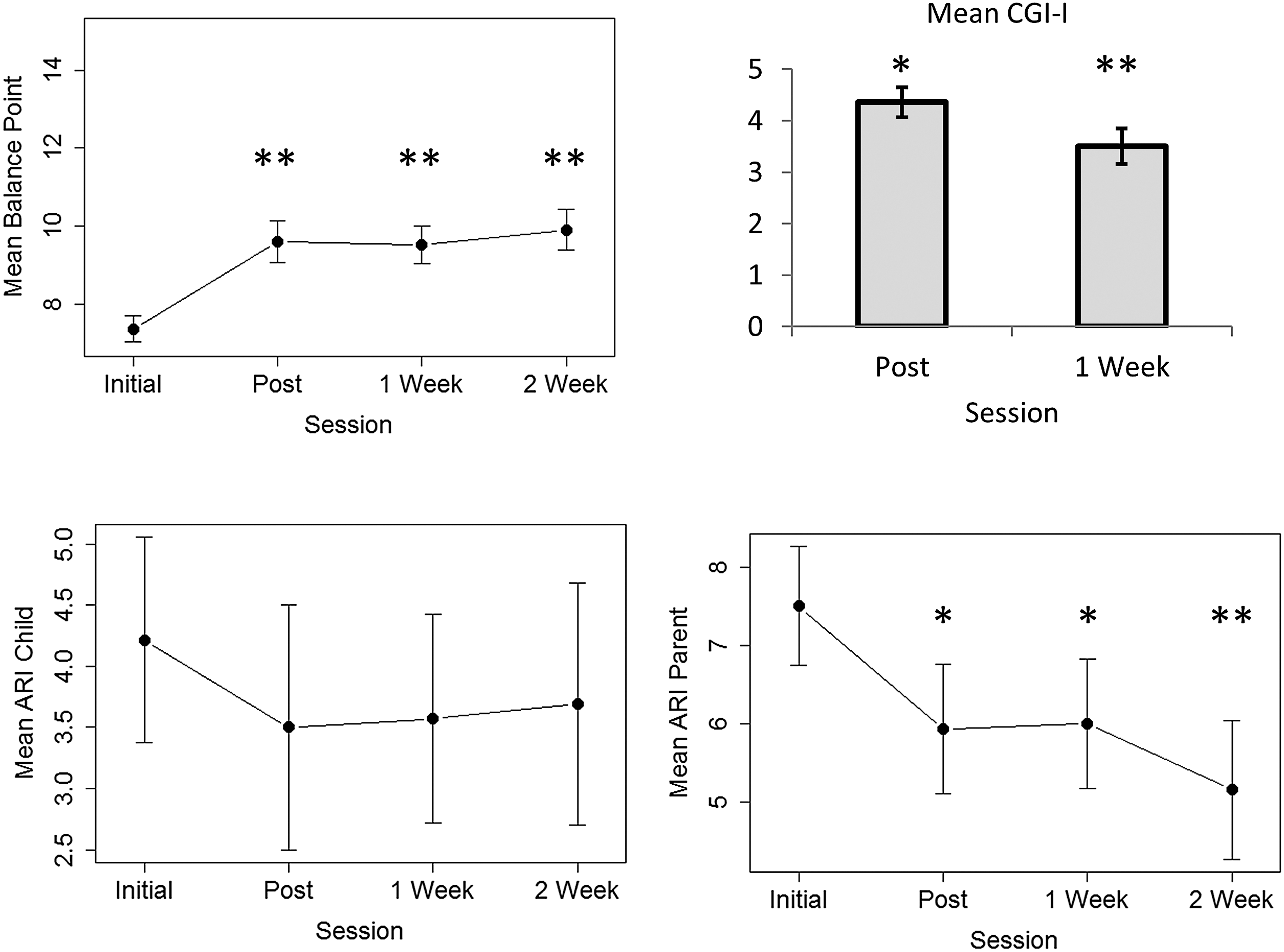
Disruptive mood dysregulation disorder (DMDD) youth (n = 14) responded to four daily sessions of training toward happy judgments of ambiguous faces, reflected by increasing balance points, decreased parent-report irritability (Affective Reactivity Index [ARI]), and clinical improvement (mean Clinical Global Impressions-Improvement [CGI-I] scores <5). For balance point and parent-report ARI, asterisks indicate p values for posttraining assessment versus initial parameter estimates. For CGI-I, asterisks indicate p values of t tests versus a score of 5, which indicates no improvement. *p < 0.05, **p < 0.01, error bars show standard error.
Clinician-rated CGI-I scores covering the immediate posttraining to the pretraining period were in the “slightly improved” range (mean[SD] = 4.4[1.1], t[13] = 2.2, p = 0.044, d = 0.59). Scores comparing 1 week posttraining to immediately posttraining were in the “improved” range (mean[SD] = 3.5[1.3], t[13] = 4.4, p < 0.001, d = 1.17). Training was associated with reductions in parent-reported irritability with a pretraining parent ARI rating of b(SE) = 7.50(0.81) points that decreased immediately after training by b(SE) = −1.57(0.64) points, p = 0.017. These reductions in parent ARI ratings persisted 1 and 2 weeks after training, b(SE) = −1.50(0.64) and −2.41(0.65) points, respectively, p's ≤ 0.023. Training was not associated with changes in self-reported irritability on the ARI (p = 0.484).
Exploratory correlations may indicate the degree to which learning more benign interpretations is associated with clinical improvement. With Spearman's rank correlations, we measured associations between differences in the post- versus pretraining balance point, and change in irritability by 1) parent and child reports (post- minus pretraining ARI) and 2) clinician rating (posttraining CGI-I). We did not detect significant associations between changes in the balance point and CGI-I (rs [12] = −0.49, p = 0.079) or change in self-report ARI (rs [12] = −0.52, p = 0.056) or parent-report ARI (rs [12] = −0.24, p = 0.417). However, the correlation coefficients suggest a medium-sized association between the degree of balance point shift and clinical improvement (r ≥ 0.3; Cohen 1992) (Fig. 5).
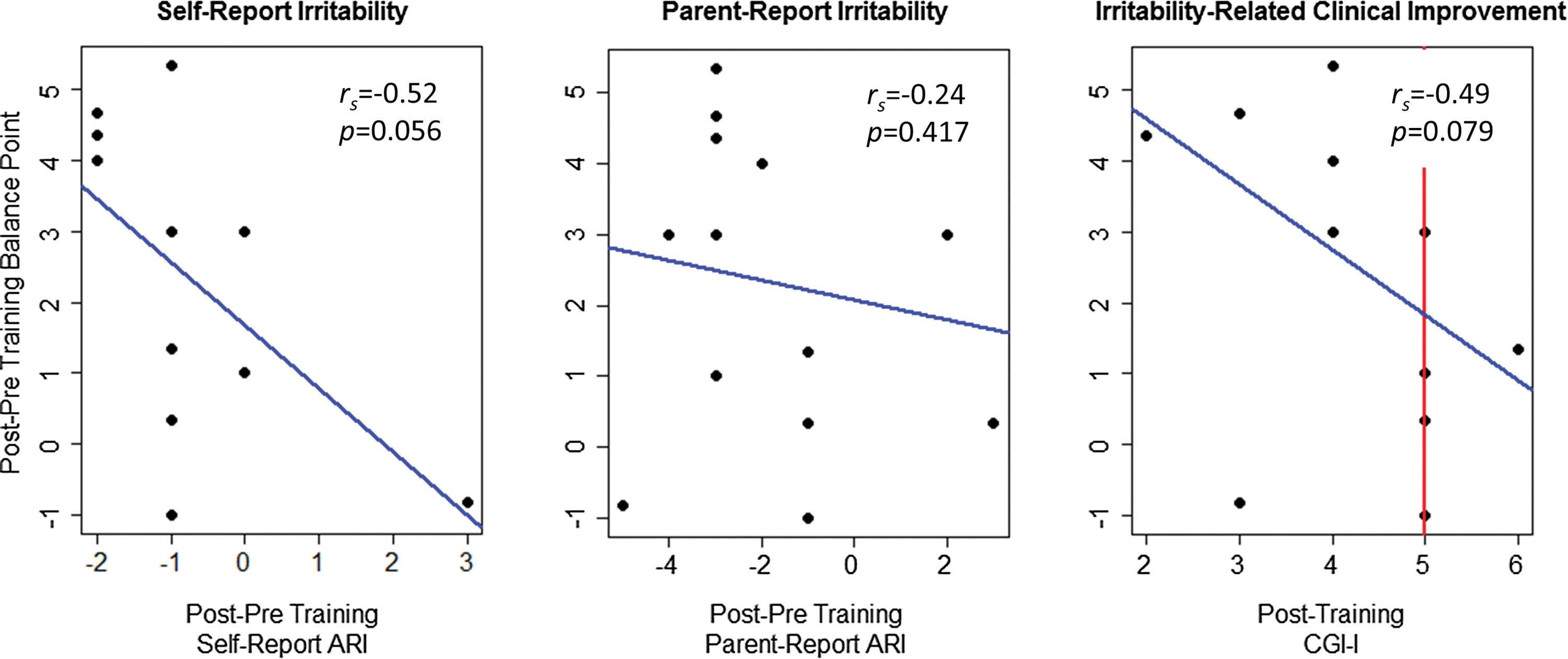
An increased bias toward happy judgments after training may be associated with reduced irritability and irritability-related clinical improvement in 14 youth with disruptive mood dysregulation disorder (DMDD). Blue trend lines are from outlier resistant “robust regression,” using reweighted least squares regression. The red line at a score of 5 in the Clinical Global Impressions-Improvement (CGI-I) corresponds to no clinical improvement, values <5 indicate improvement, and values >5 indicate clinical worsening. Insets contain Spearman's correlation coefficients and uncorrected p values. A color version of this figure is available in the online article at
Experiment 3B: Changes in amygdala and OFC responses to subtle affect after interpretation bias training in DMDD
After training, neural activation to subtle (i.e., 50%) expressions of happiness increased relative to subtle expressions of anger in the right lateral OFC, b(SE) = 0.19(0.08), p = 0.021, and the left lateral OFC, b(SE) = 0.21(0.08), p = 0.009, with a trend in the left amygdala b(SE) = 0.15(0.08), p = 0.072 (Fig. 6).

Interpretation bias training is associated with increased neural activity in response to subtle expressions of happiness, relative to anger, in the bilateral orbitofrontal cortex (OFC) and left amygdala. The brain image shows the four regions of interest (ROIs) (lateral OFCs and amygdalae) that were examined. Bar charts indicate mean % blood–oxygen-level dependent (BOLD) signal change to each 50% emotion-neutral facial morph, relative to a fixation cross, measured before (solid bars) and after (striped bars) four sessions of daily training. Asterisks represent p values for the pre-versus posttraining, angry versus happy contrast parameter estimates.
p < 0.1, *p < 0.05, **p < 0.01. A color version of this figure is available in the online article at
Discussion
Three experiments laid the groundwork for a controlled trial of interpretation-bias training treatment in irritable youth. Experiment 1 showed evidence of biased rating of face emotion in youth with DMDD. Experiments 2 and 3 showed that daily computer-based training could shift such ratings toward happy judgments and away from angry judgments, and that this shift persisted for 2 weeks without further training. Finally, Experiment 3, in youth with DMDD, suggested that having four sessions of daily open interpretation bias training was associated with reduced irritability and, possibly, altered brain function in the lateral OFC and amygdala in response to subtle expressions of happiness relative to anger.
We expected to find an interpretation bias toward angry judgments of ambiguous facial affect in DMDD based on earlier work in SMD (Brotman et al. 2010; Hommer et al. 2013) and the foundational work of Dodge (Crick and Dodge 1994; Wilkowski and Robinson 2008). It is of note that we found a clear interpretation bias to only one male face-identity in the IBT task. Although our data do not allow us to draw any conclusions as to why this may have occurred, this finding highlights the importance of future research on the possible effect of nonemotional facial features on interpretations of hostility (Marsh et al. 2005).
We found a training effect in HV and DMDD youth, consistent with prior work in healthy adults and in adolescents with conduct problems (Penton-Voak et al. 2013). Such training could reduce irritability by altering interpretative biases that promote anger-based reactions, a possibility supported by our preliminary fMRI results suggesting that tIBT may alter circuits mediating responses to ambiguous social threat cues (Hooker et al. 2006; Brotman et al. 2010; Thomas et al. 2012, 2013). However, more work is needed to establish a brain-based mechanism mediating interpretation bias training and its possible effects on irritability. These results are also consistent with two meta-analyses of trainings targeting a variety of disorder-specific negative interpretation biases. These studies have shown small effects on clinical depression and anxiety (Hallion and Ruscoe 2011; Cristea et al. 2015). Another type of training, attention bias modification, also has also shown small to moderate effects on depression and anxiety symptoms (Hakamata et al. 2010; Linetzky et al. 2015).
Limitations
As an early investigation of interpretation bias in pathologic irritability, this study has limitations. We have not developed a nonlinear model to assess the influence of potential confounds, such as gender and anxiety, as covariates. The results of Experiment 1 may not be directly comparable with the results in Experiments 2 and 3, because Experiment 1 used a different task and analytic method than Experiments 2 and 3. Results may be confounded by high psychiatric comorbidity in DMDD. In the open trial, we cannot distinguish between the effects of expectancy, observer bias, social desirability, regression to the mean, or interpretation bias training on irritability and irritability-related clinical improvement. Additionally, the sample size of both the pilot clinical trial and the fMRI study was quite small. A randomized controlled trial of tIBT in a larger sample of DMDD, with pre- and posttraining fMRI, is needed to confirm these results and provide more data regarding potential mechanisms.
Conclusions
We provide preliminary evidence that youth with DMDD exhibit a hostile interpretation bias, as measured by a bias toward judging ambiguous facial expressions as angry, which is likely moderated by a participant's reaction to nonemotional facial features. A small, open, pilot trial of training toward benign interpretations of ambiguous facial expressions suggests that such training may be associated with reduced irritability and decreased clinical impairment caused by DMDD, possibly with alterations in relevant brain circuitry.
Clinical Significance
Few evidence-based treatments exist for pathologic irritability. We provide preliminary evidence that a novel, computer-based treatment targeting interpretation bias warrants further testing as a novel intervention designed to decrease irritability in youth with DMDD.
Footnotes
Acknowledgments
We thank the participants and families who were involved in this study, and the staff of the Emotion and Development Branch at NIMH. We also thank Dr. Gang Chen, statistical mathematician at the NIMH Scientific and Statistical Computing Core, for his aid in developing our analytic methods.
Disclosures
Drs. Munafò and Penton-Voak are codirectors of Jericoe Ltd., which produces software for the assessment and modification of emotion recognition. The other authors have no conflicts of interest or outside financial support to report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.