
Abstract
Objectives:
To compare child and adolescent psychiatrists' (CAPs) practices in the treatment of preschool children with attention-deficit/hyperactivity disorder (P-ADHD) with published guidelines, and to determine which clinical factors most influence physicians' decisions to initiate pharmacotherapy for P-ADHD.
Methods:
We developed and mailed the Preschool ADHD Treatment Questionnaire (PATQ) to a randomly selected national sample of ∼2200 CAPs trained in the management of ADHD. The PATQ asked CAPs about their approach to clinical management of children ages 4–5 years with ADHD—specifically, how often they recommend parent training in behavior management, medication as a first- or second-line treatment, and which medication they typically choose first. CAPs also rated the perceived importance of 19 different clinical factors in their decision to initiate pharmacotherapy. These 19 factors reflected five child-centered areas of concern: ADHD risk factors, education concerns, social issues (SI), emotional stress, and physical safety (PS). The physicians were asked to rate each factor on a 4-point Likert scale from “not important” to “very important.”
Results:
The final sample consisted of 339 board-certified CAPs. When adherence to the Academy of Child and Adolescent Psychiatry (AACAP) guidelines was defined as initial treatment with behavior management (not medication) and pharmacotherapy specifically with methylphenidate as second-line treatment, only 7.4% of CAPs followed clinical guidelines. Most physicians identified PS as an important or very important factor when initiating pharmacotherapy for P-ADHD (93.4%), followed by educational concerns (EC) (79.9%), emotional stress (69.6%), SI (52.8%), and the presence of risk factors for ADHD (32.7%).
Conclusions:
The overwhelming majority of CAPs do not follow current AACAP guidelines for treatment of P-ADHD, especially regarding medication initiation and selection. When deciding whether to prescribe medication for P-ADHD, safety and EC were the most important and historical risk factors for ADHD were the least important clinical factors.
Introduction
T
The AACAP's recommendation to use MPH as the first-line stimulant treatment for ADHD is based on findings from a large multicenter clinical trial. The Preschool ADHD Treatment Study (PATS), funded by the National Institute of Mental Health, was the first randomized clinical trial to evaluate MPH use in preschoolers with ADHD (Kratochvil et al. 2004; Greenhill et al. 2006). The PATS was designed to address systematically the efficacy and safety of immediate-release MPH (Kaplan et al. 2011). Subjects were boys and girls 3–5 ½ years of age who met the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) criteria for ADHD. MPH doses used in the study ranged from 1.25 mg thrice daily titrated up to a final dose of 7.5 mg thrice daily. Medication efficacy was measured using teacher and parent versions of the Swanson, Nolan, and Pelham Rating Scale. The study demonstrated significant reductions of ADHD symptoms in preschool children compared with placebo, although effect sizes (0.4–0.8) were smaller than those cited for school-age children treated with MPH (Greenhill et al. 2006).
Although ADHD treatment guidelines are now available for preschool children, to date no studies have examined to what extent child and adolescent psychiatrists (CAPs) follow these guidelines regarding initiation of pharmacotherapy. Similarly, there is no information about what factors influence a clinician's decision to initiate treatment with medication in young children with ADHD.
Methods
This study was reviewed and approved by the Institutional Review Board of the North Shore-Long Island Jewish Health System. Because the study consisted of an anonymous survey that presented minimal risk of harm to subjects, a waiver of consent documentation was granted.
Questionnaire design
For this study, the investigators created the Preschool ADHD Treatment Questionnaire (PATQ). This instrument was designed to obtain information about physician demographic characteristics—gender, board-certified specialty, type of practice, years in practice, and practice location—and physicians' practice patterns, including the number of child/adolescent patients seen per week, frequency with which they make a diagnosis of ADHD in preschool patients, their first-line medication of choice, and how often they use medication and/or behavioral management as part of their initial treatment plan. The PATQ also asked respondents to rate 19 clinical factors that might influence their decision to start medication. Respondents rated each factor on a four-point Likert scale: “not important,” “somewhat important,” “important,” and “very important.” The factors were grouped into five categories: physical safety (PS), educational concerns (EC), emotional distress (ED), social issues (SI), and historical risks factors (RF) for ADHD.
Subjects
Contact information for CAPs was obtained from a commercial list broker, medical marketing service (MMS), Inc. MMS, Inc. provided names and mailing addresses for 6141 CAPs. From this total cohort, questionnaires were mailed to 2200 randomly chosen CAPs who were practicing across the United States. Analyses were limited to responses from CAPs who indicated they were currently board certified in child and adolescent psychiatry.
Survey administration
The survey was mailed with a cover letter, postage-paid return envelope, and a complimentary copy of an ADHD Medication Guide (
Statistical analysis
Chi-square tests were used to compare respondents' answer choice frequencies across specialties for each question. Significant p-values for chi-square tests of multiple comparisons were determined by using the Bonferroni correction. The alpha was set at p < 0.003 (p < 0.05/19). Effect sizes (φ) were reported for significant chi-square values.
Results
Respondent demographics
Of the ∼2200 surveys that were mailed out to CAPs, a total of 356 surveys were returned, giving an overall raw response rate of 16.2%. Data from 11 respondents who were not board certified in child and adolescent psychiatry were excluded from the analysis, and six more respondents were excluded because they indicated that they never diagnose ADHD in preschool-age children. Thus, data from 339 CAPs were included in the analyses. The demographic and practice characteristics of the final sample are shown in Table 1. Of the 339 respondents, 53.4% were female. More than half (56.1%) had been in practice for more than 16 years and only 8.3% for fewer than 5 years. The vast majority of the sample (91.0%) reported seeing at least six children or adolescents with ADHD per week.
Missing data from 10 respondents; two respondents reported practicing in two different Census regions.
Geographic region as defined by the U.S. Census Bureau.
Missing data from two respondents.
Missing data from seven respondents.
Respondents able to select more than one practice setting.
ADHD, attention-deficit/hyperactivity disorder.
Preschool ADHD treatment recommendations
Tables 2 and 3 provide a detailed breakdown of the percentage of CAPs who would recommend parent training in behavior management and/or medication as treatment for a 4–5-year-old child with ADHD. Figure 1 and Supplementary Data (Supplementary Data are available online at
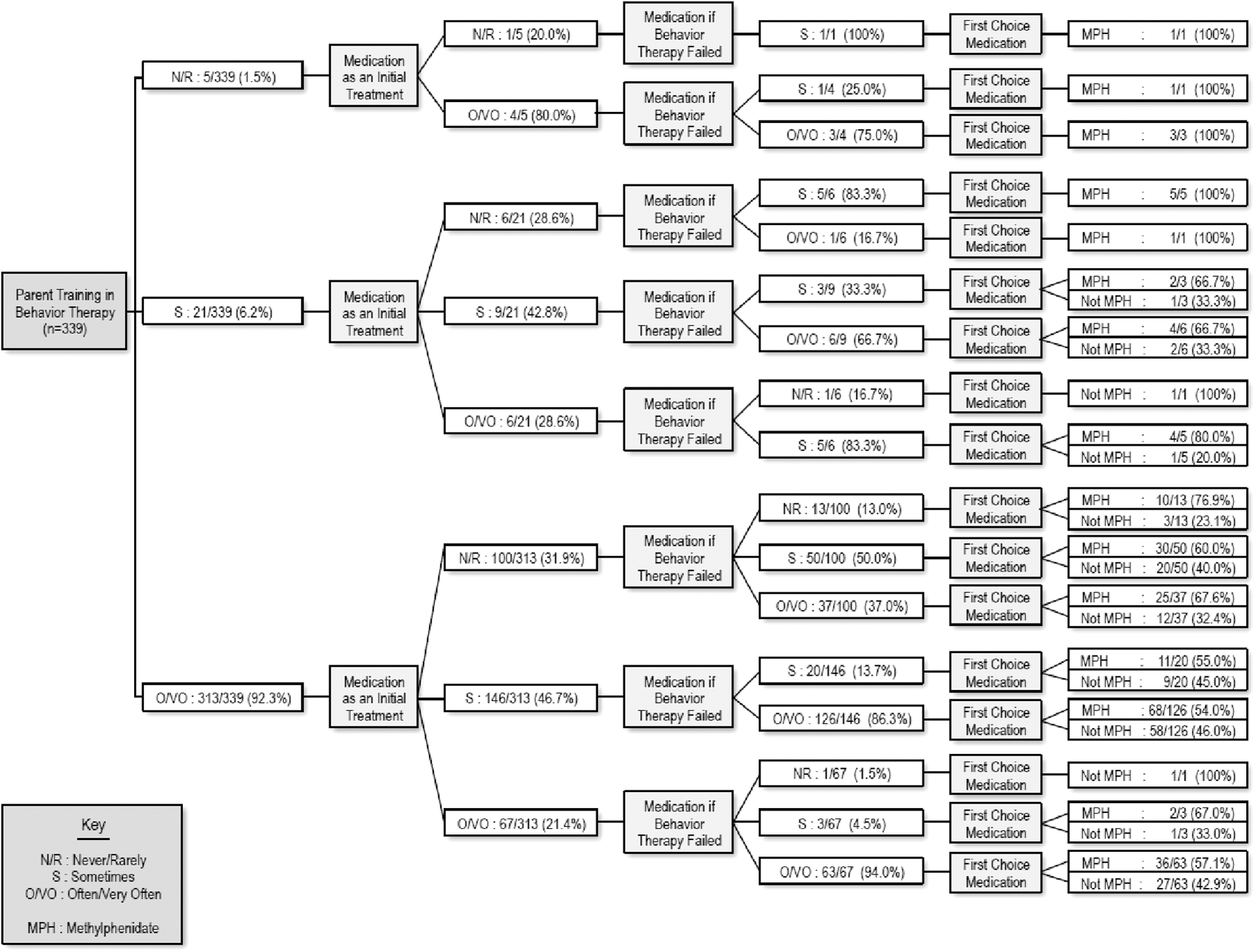
Schematic of responses by child psychiatrists regarding management of a preschool child with ADHD. ADHD, attention-deficit/hyperactivity disorder.
Missing data from six respondents (n = 333).
Missing data from one respondent (n = 338).
To determine how often physicians follow the AACAP guidelines for the treatment of preschool children with ADHD, we first calculated the percentage of CAPs who met each of the three requisite criteria individually: (1) “often” or “very often” recommend parent training in behavior management therapy (Recommendation #1), (2) “never” or “rarely” recommend medication as part of an initial treatment plan (Recommendation #2), and (3) choose MPH as the first choice medication (Recommendation #3) (Fig. 2 and Table 4).
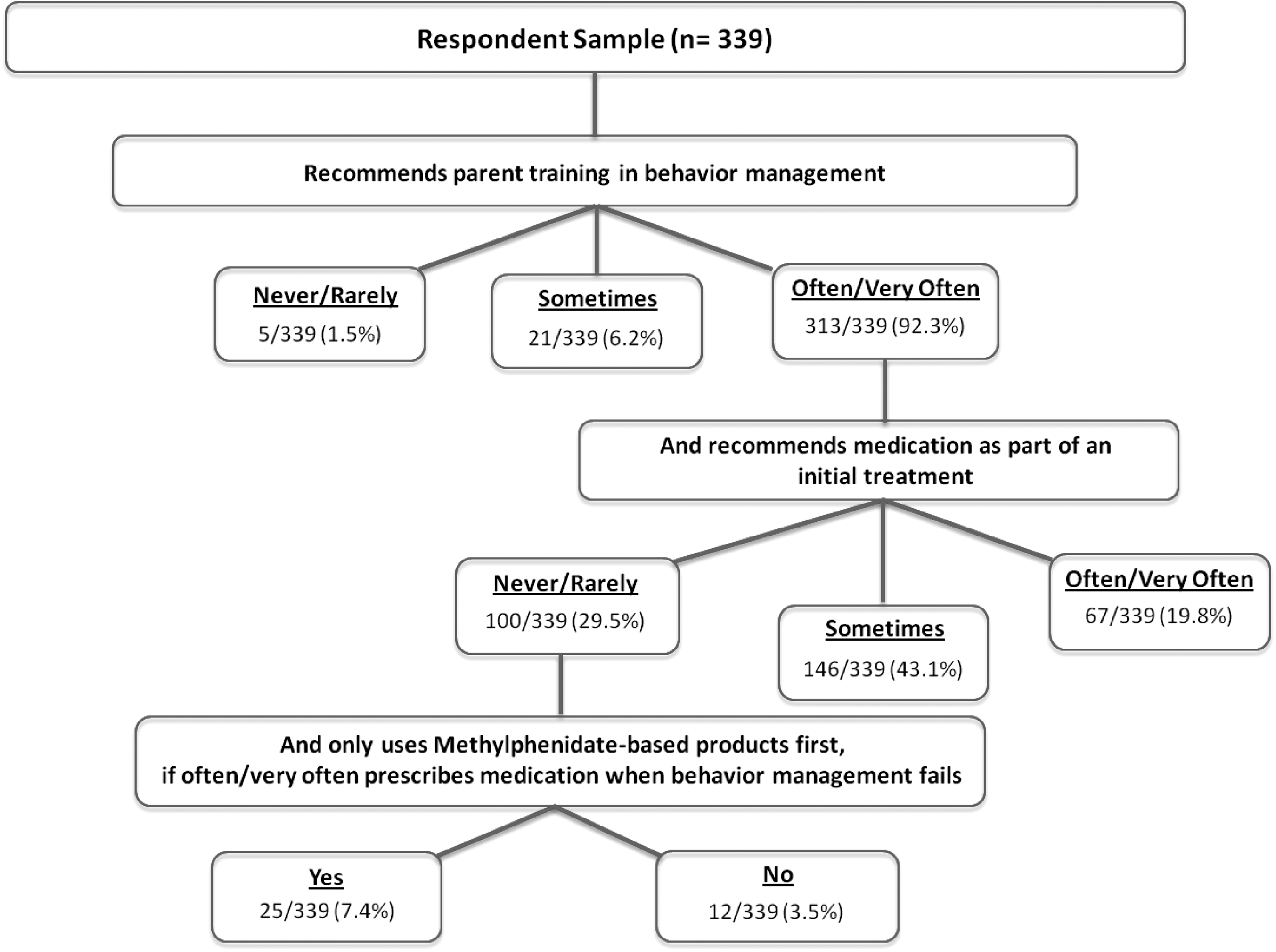
Adherence criteria for preschool ADHD treatment. ADHD, attention-deficit/hyperactivity disorder.
Missing data from six respondents.
Missing data from one respondent.
ADHD, attention-deficit/hyperactivity disorder.
Adherence to Recommendation #1
92.3% of all respondents reported that they “often” or “very often” recommend parent training in behavior management as a first-line treatment for P-ADHD.
Adherence to Recommendation #2
71.3% of all respondents reported that they “often” or “very often” recommend pharmacotherapy as treatment for P-ADHD when behavior management was unsuccessful. Of the 313 CAPs who recommend behavior therapy as a first-line treatment for P-ADHD, 11.8%, per guidelines, recommend medication as a second-line treatment if behavior management failed. Additional analyses revealed that 21.4% (67/313) of physicians who recommend parent training in behavior therapy “often” or “very often” recommend medication as a part of the initial treatment, and 36.4% (114/313) “never” or “rarely” recommend medication, even if behavior therapy had failed. Of the 107 physicians who reported they “never” or “rarely” recommend medication as a part of the initial treatment, 15 (14.0%) also do not recommend medication if behavior therapy has failed. Among all respondents, 8.6% (29/339) indicated that they would “never” recommend medication for a preschool child with ADHD and 27.4% (93/339) would only do so “rarely.”
Adherence to Recommendation #3
CAPs were asked which medication they “typically choose first” when prescribing medication for P-ADHD. Response options were limited to MPH, amphetamines (AMP), or nonstimulants. Twenty respondents (5.9%) selected two or more medications and were thus excluded from this analysis. Of the 319 CAPs who identified a single medication for initial treatment of P-ADHD, 63.3% (202/319) reported they use MPH, 20.4% (65/319) use an amphetamine preparation, and 16.3% (52/319) use a nonstimulant. Of the 241 CAPs who reported they recommend treatment with medication when behavior therapy failed, 86 (35.7%) indicated that they do not use MPH as their first-line medication, with 50 (20.8%) choosing an amphetamine and 36 (14.9%) a nonstimulant first.
Strict adherence (#1 and #2 and #3)
AACAP guidelines recommend MPH for initial treatment with medication, although CAPs do not always prescribe it. Overall, 7.4% (25/339) of CAPs indicated adherence to all three guideline recommendations for treatment of P-ADHD, which includes MPH as the first-choice medication when other treatment methods have failed.
Less stringent adherence (#1 and #3 only)
The CAPs were asked if they prescribe medication as part of their initial treatment plan; however, this question did not indicate whether parents had previously received training in behavior management. Thus, there was unintended ambiguity regarding whether or not a recommendation for “medication as part of an initial treatment” inherently deviated from AACAP guidelines. To eliminate this uncertainty, we reanalyzed the adherence rate based only on recommendations #1 and #3. Based on this alternate less rigid approach, 54% of CAPs follow AACAP guidelines, that is, by recommending behavior therapy first line and selecting MPH when prescribing medication.
Mediating variables
Post hoc analyses of respondents' number of patients with ADHD seen per week (0–5, 6–15, 16+) versus adherence to guidelines revealed that there was a significant difference in adherence to lenient criteria (χ 2 = 7.72; p = 0.02), but no significant difference with the strict criteria (χ 2 = 2.76; p = 0.25). Specifically, adherence to the less stringent guidelines was at 64% for CAPs who saw 6–15 patients with ADHD per week, whereas adherence was significantly lower for those who saw ≤5 ADHD patients (40%) or ≥16 patients (50%) per week (χ 2 = 7.72; p = 0.02). Additional post hoc analyses compared the number of years in practice among CAPS (<5 years, 5–15 years, and 16+ years) with their adherence to guidelines and found no significant differences for adherence to lenient (χ 2 = 0.66; p = 0.72) or strict (χ 2 = 1.45; p = 0.48) criteria.
Factors influencing the decision to treat preschool children with ADHD with medication
Although behavior therapy is recommended as a first-line treatment for P-ADHD, many communities may have limited professional resources to provide this form of therapy. To evaluate whether availability of behavioral treatments influenced the clinical approach of CAPs, respondents were asked “In your area, how available are behavioral counseling services for parents of preschoolers with ADHD?” One-fourth (25.7%) indicated it was “very available,” 53.7% “somewhat available,” and 20.6% “not very available.”As expected, CAPs were significantly more likely to “often” or “very often” recommend parent training in behavior management if it was perceived as being available in their local community. Behavior therapy was recommended by 96.5% of CAPs in communities, in which it was described as “very available,” versus 93.9% and 82.6%, in which it was described as “somewhat available” or “not very available,” respectively (χ 2 = 9.89; p < 0.007).
CAPs were also asked, “In addition to recommending parent counseling in behavior management, how important are each of …[nineteen] factors in deciding to treat [p-ADHD] with medication?” These clinical factors were then grouped into five domains as displayed in Table 5. CAPs viewed PS and EC as most important for initiating pharmacotherapy, followed by ED, SI, and ADHD risk factors.
All factors in Table 5 are listed with their corresponding letter and number combination referenced in the text.
N varies slightly for each factor based on the number of CAPs who responded.
These values represent the arithmetic mean for each category overall.
ADHD, attention-deficit/hyperactivity disorder; CAP, child and adolescent psychiatrist; EC, educational concern; ED, emotional distress; OT, occupational therapy; PS, physical safety; PT, physical therapy; SI, social issues; SLT, speech-language therapy.
A child's being in “danger of hurting self” and “danger of hurting others” was considered to be the two most important factors in their deciding to use medication. Seventy-six percent (255/337) of CAPs rated “danger of hurting self” as “very important.” Seventy-one percent (239/337) rated “danger of hurting others” as “very important.” Fifty-four percent (181/338) included “recent expulsion” as the next most important factor, while 48.7% (165/339) identified “requires adult supervision” and 48.8% (165/338) identified “risk of expulsion” as the next equally important factors. Forty-two percent (141/339) identified “history of maternal tobacco use during pregnancy” as “not important,” making it the least important factor in deciding to use medication. The other factors identified as least important, in descending order, included “child adopted from an overseas orphanage” (40.2%, 136/338), “premature birth” (34.8%, 118/339), “history of maternal alcohol use during pregnancy” (27.7%, 94/339), and “history of maternal cocaine use during pregnancy” (25.1%, 85/338).
Of the 333 respondents who answered the question about medication as an initial treatment for P-ADHD (Table 2), 107 (32.1%) said they never or rarely prescribe medication as an initial treatment, whereas 149 (44.8%) sometimes, and 77 (23.1%) “often” or “very often” do so. Analyses were done to determine if there were relationships between how physicians rated the importance of each clinical factor as being important and their likelihood to prescribe medication as an initial treatment. When comparing the never/rarely group with the often/very often group, no differences were noted with respect to the three most important factors (“physical safety”) or least four important factors (ADHD risk factors). Significant differences between the groups were noted for EC, ED, and SI. Family history of ADHD was the only risk factor for which differences were noted. There were also significant differences noted between the ratings of importance of factors in the five categories (Table 5): PS was significantly more likely than EC to be rated “important” or “very important” by CAPs (χ 2 = 92.84; p < 0.00001), EC significantly more likely than ED (χ 2 = 37.01; p < 0.00001), ED significantly more likely than SI (χ 2 = 48.92; p < 0.00001), and SI significantly more likely than ADHD risk factors (χ 2 = 136.98; p < 0.00001). Accordingly, PS was significantly more likely than RF to be rated as “important” or “very important” by CAPs (χ 2 = 1156.84; p < 0.00001). There was also a very significant difference in CAPs who rated factors in each of the five categories as “important” or “very important” versus other ratings (χ 2 = 1679.71; p < 0.00001).
Analyses were also done to determine if there was an association between the stated importance of each of the 19 clinical factors and the frequency with which CAPs reported using medication as an initial treatment for P-ADHD (Table 6). Of the 19 factors, 10 were identified as “important” or “very important” for CAPs in their treatment decisions regarding medication. Table 6 reports effect sizes only for significant chi-squares—all of which were moderate in size (φ = 0.20 to <0.30). Clinical factors that are identified in Table 5 as most important (Physical Safety) and least important (ADHD Risk Factors) did not significantly influence decisions by CAPs to recommend medication as an initial treatment for P-ADHD. The rated importance of clinical factors in the categories of educational, emotional, or social concerns did differ between those who indicated that they “often” or “very often” use medication as a first-line treatment compared to those who do so “never” or “rarely.”
N varies slightly for each factor based on the number of child psychiatrists that responded.
Effect size only calculated if chi-square is significant (p < 0.003). Chi-square compares CAPs who use medication as part of initial treatment never/rarely versus often/very often and who rated various clinical factors as important/very important versus not/somewhat important.
ADHD, attention-deficit/hyperactivity disorder; CAP, child and adolescent psychiatrist; EC, educational concern; ED, emotional distress; PS, physical safety; SI, social issues.
Discussion
Adherence to guidelines
This study is the first to assess in a national sample to what extent board-certified child and adolescent psychiatrists follow the 2007 clinical guidelines for the treatment of P-ADHD. On one hand, our findings confirm that almost all CAPs recommend parent training in behavior therapy as a treatment for P-ADHD. On the other hand, our results suggest that the overwhelming majority of CAPs who manage ADHD often deviate from the AACAP guidelines when treating 4–5-year-olds with ADHD; only 7.4% of all responding CAPs fully complied with AACAP guidelines.
Admittedly, this analysis may have been unduly rigid in that clinicians who indicated they prescribe medication as part of an initial treatment plan did not necessarily rule out behavior therapy as an adjunct or concurrent therapy. For this reason, we also analyzed our response data with a less strict definition of adherence. With these liberalized criteria, the nonadherence rate was drastically reduced from 92% to 46%; nonetheless, this still suggests that almost half of CAPs do not follow guidelines when treating P-ADHD.
In trying to identify predictors of guideline adherence, post hoc analyses were done examining the volume of ADHD patients seen weekly and number of years in practice. Interestingly, CAPs who saw the lightest or the heaviest volume of patients were less likely to follow guidelines. This is not unexpected in that those who treat ADHD infrequently may be not aware of AACAP guidelines and those who treat very large number of cases may feel that their experience and expertise justify deviation from published guidelines on a case by case basis. In hindsight, it would have been helpful to assess respondents' familiarity with the AACAP guidelines, although it is worth noting that physician responses were obtained in 2012, many years following the publication of AACAP's general practice parameters for ADHD (Dulcan et al. 1997) and subsequent guidelines for psychopharmacologic treatment for very young children (Gleason et al. 2007).
It is important to note that AACAP's guidelines are not intended as mandates to clinicians. When published, the Academy emphasized that its algorithm was “not intended to suggest certainty, where none exists,” and that clinicians may “determine that an alternative approach is indicated in a particular clinical situation” (Gleason et al. 2007). Although AACAP clearly recognized and acknowledged the need for clinicians to deviate from their published guidelines, it is hard to imagine that they would countenance clinicians' deviating from guidelines in as much as 46%–92% of the time.
Use of ADHD medication in preschoolers
Although it was still low, the reported rate of adherence to each individual guideline was considerably higher than was adherence to all of the guidelines combined. Current clinical guidelines recommend behavior therapy as a first-line intervention before initiating pharmacologic treatment for preschoolers with ADHD (Gleason et al. 2007; Subcommittee on Attention-Deficit/Hyperactivity Disorder et al. 2011). The bases for this guideline is the demonstrated efficacy of behavior therapy in reducing ADHD behaviors (Pelham et al. 1998; Greenhill et al. 2003) and the greater potential for side effects of medication in this age group (Wigal et al. 2006). A recent review study by Charach et al. (2013) examined eight previous studies on parent behavior training and determined that there is “high strength of evidence” for its improving ADHD symptoms in preschoolers. The review concluded that parent behavior training is the “best first-line treatment” for ADHD in preschool children. Although the benefit of behavior interventions has not been directly compared to pharmacotherapy in this population, it is important that physicians understand its benefits and empirical evidence supporting it as parent behavior training as the first line of treatment.
While a significant majority of responding physicians (92.3%) reported that they “often” or “very often” recommend parent training in behavior management as part of initial treatment, only 31.6% of the sample reported “never” or “rarely” prescribing medication as part of initial treatment. One possible explanation is that the P-ADHD patients referred to these CAPs had such severe symptoms or impaired function that there was perceived clinical urgency in initiating pharmacotherapy. Another possibility is that many of these preschool children had, before evaluation by these CAPs, failed to benefit from behavior therapy and, thus, prescribing medication was indeed not a deviation from AACAP guidelines.
While pharmacotherapy is not recommended as initial treatment, treatment with medication is indeed recommended for 4–5-year-olds with moderate to severe functional disruption in the home and other settings, despite behavior therapy (Gleason et al. 2007; Subcommittee on Attention-Deficit/Hyperactivity Disorder et al. 2011). However, 71.3% of the surveyed CAPs “often” or “very often” recommended medication when behavior therapy had failed. Thus, despite proven safety and efficacy, a considerable number of CAPs are still reluctant to medicate young children.
ACAAP guidelines recommend MPH as the first-line medication for preschoolers (Subcommittee on Attention-Deficit/Hyperactivity Disorder et al. 2011). However, only 63.3% of CAPs selected MPH as their first-line medication. The efficacy and safety of stimulant medication (MPH and amphetamine preparations) in children 6 years of age and older is well established. Two nonstimulants, guanfacine and atomoxetine, also have demonstrated efficacy and safety in this age group. Historically, the evidence from experience with older children had been extrapolated to guide treatment of younger (preschool age) children. The rationale for recommending MPH as the preferred stimulant treatment for P-ADHD is that it is the only medication that has been studied adequately in this age group (Greenhill et al. 2006). The largest study, involving 165 children, was the PATS, which was the first randomized multicenter clinical trial designed to systematically assess the safety and efficacy of immediate-release MPH in preschool children with ADHD (Greenhill et al. 2006). The findings indicated that MPH is generally effective, safe, and tolerable in treating P-ADHD and should be used as the preferred pharmacological treatment (Wigal et al. 2006; Ghuman et al. 2008). However, because of the small number of quality studies available, Charach et al. (2013) found that there is “low strength of evidence” for the ability of MPH to improve ADHD symptoms in preschool children. In addition, preschool children tend to be more susceptible to adverse effects of MPH, with more frequent rates of appetite loss, trouble sleeping, stomachaches, social withdrawal, and lethargy compared to placebo (Charach et al. 2013).
There is insufficient evidence for the safety and efficacy in this age group of amphetamines or any of the nonstimulant ADHD medications to recommend them (Subcommittee on Attention-Deficit/Hyperactivity Disorder et al. 2011). However, despite the paucity of evidence, short-acting amphetamine products (Adderall®, Zenzedi®, ProCentra®, and Evekeo™) are approved by the Food and Drug Administration (FDA) for use in children as young as 3 years, which may be confusing to physicians. At present, none of the long-acting stimulants is approved for use in children below age 6. The FDA recognizes that there is lack of clinical evidence to support use of amphetamines (short- or long-acting formulations) in young children and has requested that the manufacturer of lisdexamfetamine conducts studies to document safety and efficacy in 4- and 5-year-old children (Media, News, and Press Release 2014).
It is of interest that CAPs chose a nonstimulant as their first-line medication choice in as many as 1/5 cases. Although their rationale for doing so was not a focus of this study, considerations might have been that they were targeting other than core ADHD symptoms (e.g., aggression) or that many of these were children with an autism spectrum disorder. There have been other reports that appear to corroborate this phenomenon. For example, in an analysis of prescription data for preschoolers with emotional and behavioral disorders on Midwestern state Medicaid, mid-Atlantic state Medicaid, and a Health Maintenance Organization setting in the Northwest, investigators found that there was a 6.8- to 28.2-fold increase from 1991 to 1995 in the prevalence of clonidine use, as opposed to a 1.8- to 3.1-fold increase in stimulant use (Zito 2000).
There remains limited empirical evidence for ADHD medication efficacy and safety in preschoolers, and there is little doubt that guidelines will continue to evolve over time. Similarly, the availability of liquid, chewable, and transdermal stimulant formulations not only make it easier to administer stimulant medications to young children but they also allow these medications to be titrated more precisely (although off-label)—even at doses below current FDA recommendations. It is possible that specific medication prescribing trends will evolve as clinicians gain greater familiarity and experience with these various new formulations.
Factors influencing the initiation of pharmacotherapy in preschool children with ADHD
Since a large majority of CAPs use medication as initial therapy, it is important to examine which factors are important to them when making the decision to do so. The present study found that educational and PS concerns were the most important factors in considering whether to prescribe medication for preschool children with ADHD. In contrast, factors that confer an increased risk on children of having ADHD (especially maternal tobacco use during pregnancy) were reported to be the least important. It appears that clinicians will deliberately deviate from published guidelines in considering pharmacotherapy for preschool children with ADHD when, in their judgment, a child's physical well-being and/or developmental functioning are significantly at risk.
Although this study has many strengths and the findings are revealing, several methodological weaknesses and limitations must be acknowledged. First, as is typical of survey-based research involving clinicians, our overall response rate (16.2%) was low. Since we do not have demographic data for the sample to whom questionnaires were mailed, we cannot rule out that there are some demographic differences between our sample and the larger population of CAPs and that this may introduce some potential skew or bias in our results. In contrast, with responses from 339 CAPs, our sample was more than adequate for statistical analysis and the cohort was demographically varied in terms of age, gender, clinical practice setting, and volume of ADHD patients treated.
A second notable limitation of our study relates to the wording of the question about recommending medication as part of an initial treatment regimen. Although there was unintended ambiguity regarding whether or not behavior therapy had been previously implemented, this was not a significant factor. For example, the fact that 92.3% of respondents indicated that they “often” or “very often” recommend parent training makes it clear that the overwhelming majority of CAPs understood the intent of the question—that this was a treatment naive family (i.e., the family did not have prior behavioral therapy). Concern about ambiguity may only apply to the very small number of respondents (24/339) who indicated that they “never” or “rarely” recommend parent training. It is further reassuring that 6 of these 24 CAPs indicated they would only recommend medication if behavior therapy had failed.
Availability of parent training in behavior management significantly influenced whether or not CAPs recommended it as a first-line treatment. We cannot verify the accuracy of CAPs' perceptions regarding availability. If the CAPs' assessment of availability was indeed accurate, then one could argue that deviation from guidelines regarding behavior therapy was perhaps justified. This approach is formally suggested by the American Academy of Pediatrics. In their recent guidelines for ADHD, the AAP states that “In areas where evidence-based behavioral treatments are not available, the clinician needs to weigh the risks of starting medication at an early age against the harm of delaying diagnosis and treatment” (Subcommittee on Attention-Deficit/Hyperactivity Disorder et al. 2011). Of course, it is possible that CAPs may not have an accurate assessment of the availability of behavioral therapists and that their predilection to pharmacotherapy as a first-line treatment may influence their perception of resource access.
Conclusions and Clinical Significance
This study was the first to assess the extent to which CAPs follow published guidelines for the treatment of preschool children with ADHD and to determine which clinical factors are most important in deciding to initiate pharmacotherapy. It appears that the vast majority of CAPs recommend parent training in behavior therapy as a treatment for P-ADHD, but do not follow all of the pharmacotherapy guidelines outlined by AACAP. Specifically, contrary to the guidelines, most CAPs use medication as part of initial treatment at least “sometimes.” The most important factors to clinicians regarding use of pharmacotherapy for P-ADHD were PS considerations (for the preschool child and others) and educational/developmental concerns. In the future, it would be helpful to clinicians if AACAP guidelines were revised to delineate when treatment with medication can or should be considered as a first-line treatment for P-ADHD—either instead of or in conjunction with behavior therapy.
Footnotes
Disclosures
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.