
Abstract

To The Editor:
C
Case Report
Our patient was an 8-year-old Caucasian male with ASD, intermittent explosive disorder and a full-scale intelligence quotient (IQ) of 46. He presented for his 13th acute psychiatric admission because of increased aggressive behaviors at home and school. Medications at the time of admission included OXC 450 mg twice daily; clonidine 0.1 mg twice daily; and QTP 200 mg every morning, 200 mg at noon, and 300 mg at bedtime. The patient's history of impulsive and aggressive behaviors resulted in many past psychotropic medication trials that were discontinued for various reasons: Risperidone (weight gain), aripiprazole (lack of efficacy), guanfacine (lack of efficacy), lamotrigine (lack of evidence and efficacy), and bupropion (lack of evidence and possible activation). At the time of admission, drug–drug interactions were noted between OXC and QTP. QTP was initially increased to 300 mg three times daily because of the known drug–drug interaction. Upon reviewing available efficacy data for OXC in treating symptoms of aggression, it was decided to discontinue OXC. In order to avoid cholinergic system rebound effects, OXC was tapered over a two week period. The patient continued to struggle with agitation in the evenings, requiring nearly daily restraint procedures during the 1st week of the OXC taper. These behaviors were largely improved during week 2 of the OXC taper. The patient was discharged two weeks following the discontinuation of OXC with prescriptions for QTP 300 mg three times daily, clonidine 0.1 mg twice daily, and polyethylene glycol 17 g twice daily. Two months following discharge, the patient continued on the same medication regimen with no new or worsened adverse events, no physical aggression, and good attendance at school and medical appointments.
Therapeutic drug monitoring of serum QTP trough concentrations was conducted several times throughout the OXC taper and previously in 2013 in the absence of CYP3A4 inducing or inhibiting medications (Fig. 1). All serum QTP troughs were drawn after QTP had reached concentration steady-state (Css) and were quantified at ARUP Laboratories (Salt Lake City, UT). None of the obtained QTP serum concentrations were classified to be in the therapeutic range (100–500 ng/mL) (Hiemke et al. 2011).
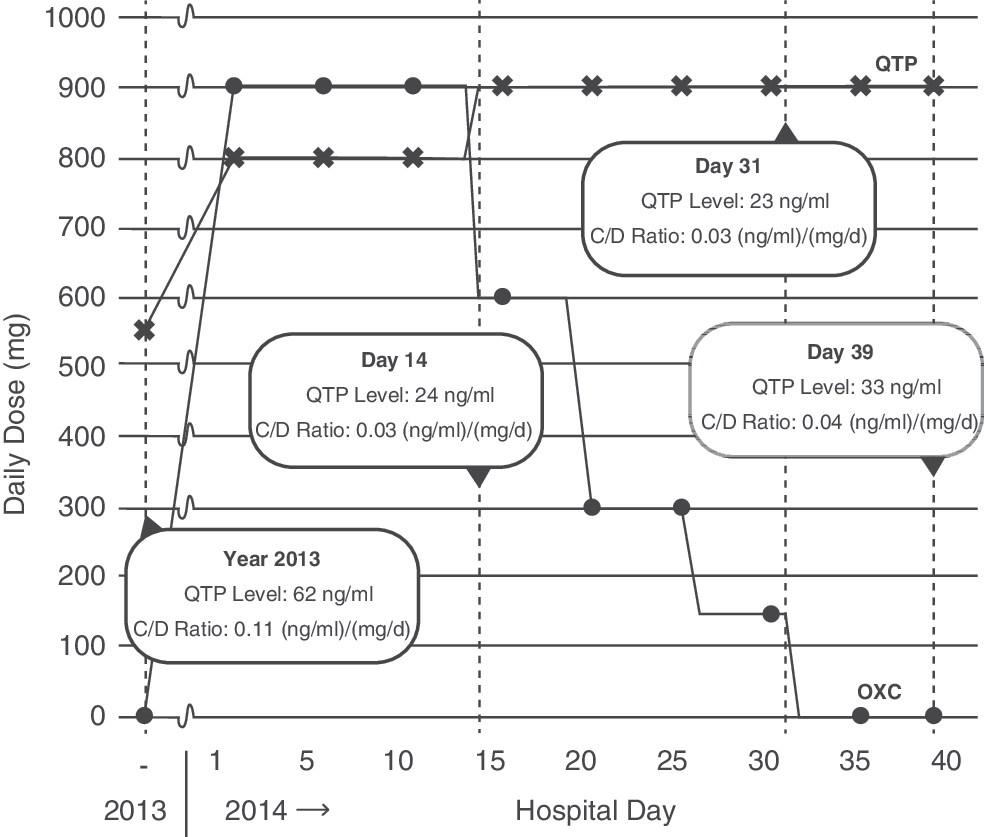
Oxcarbazepine and quetiapine dose changes with associated quetiapine concentration to drug (C/D) ratios.
Discussion
The addition of OXC appeared to have reduced the QTP C/D ratio by >70% in our patient (Fig. 1). This drug–drug interaction is clinically significant; however it is not emphasized in current literature (de Leon 2014). QTP is a substrate of CYP3A4, in which concomitant administration with a strong CYP3A4 inducing agent can reduce concentration maximum (Cmax) by 80% (Grimm et al. 2005). OXC is considered to be a moderate CYP3A4 inducer (Andreasen et al. 2007). Our patient's QTP C/D ratio was practically unchanged from the initiation of a two week OXC taper to drug discontinuation. This finding supports the theory that CYP3A4 induction diminishes slowly when OXC therapy is being discontinued (de Leon 2014).
There is currently a paucity of randomized, controlled trials evaluating the effectiveness of antiepileptic drugs in ASD. A recent meta-analysis suggested a modest effect for antiepileptic monotherapy in ASD, although no studies evaluating OXC were included (Hirota et al. 2014). This case demonstrates that the combination of OXC and QTP may significantly reduce QTP concentrations and, possibly, therapeutic efficacy. As no randomized, controlled trials evaluating the safety and efficacy of OXC for irritability in ASD currently exist, in addition to the risk of drug–drug interactions, we recommend careful consideration of risks and benefits prior to prescribing OXC in ASD, especially in patients receiving multiple medications.
Footnotes
Acknowledgments
We thank Kurt McGrane for assistance with the figure.
Disclosures
No competing financial interests exist.