
Abstract
Objective:
Aripiprazole, an atypical antipsychotic drug, has shown potential as a promising candidate for the treatment of Tourette's disorder (TD). However, the effectiveness and the tolerability profile of aripiprazole in the reduction of tics in children and adolescents with TD have not been systematically analyzed. This meta-analysis aimed to evaluate the effectiveness and tolerability of aripiprazole in children and adolescents with TD.
Methods:
We searched for clinical trials that investigated the effect of aripiprazole in children and adolescents with TD in PubMed and Web of Science. The outcomes of interest comprised the Yale Global Tic Severity Score (YGTSS) total tic scores and the Clinical Global Impressions Scale for Tic Severity (CGI-S) scores. The pooled effect size (ES) and 95% confidence interval (CI) were calculated to assess the effectiveness of aripiprazole in children and adolescents with TD.
Results:
Ten studies were retrieved from 122 citations for the analysis, and in total, 302 patients (mean age, 11.6 years; median follow-up, 9 weeks) were included in the analysis. After synthesis of the data, the meta-analysis showed significantly greater improvement in the mean change in the YGTSS total tic scores (ES = −1.99, 95% CI = [−2.26]–[−1.72]; p = 0.001) and the mean CGI-S scores (ES = −2.34, 95% CI = [−2.96]–[−1.73]; p = 0.001) from pretreatment to posttreatment. Adverse events were reported in nine trials. Drowsiness (28.5%), nausea (20.2%), and headache (13.8%) were common adverse events.
Conclusions:
The use of aripiprazole is safe, and shows therapeutic effectiveness in children and adolescents with TD.
Introduction
T
Aripiprazole, an atypical antipsychotic drug, has been used to treat various adult and pediatric disorders (Bowles and Levin 2003; Stigler et al. 2009). This drug is proposed to have a unique mechanism of action (as a partial dopamine receptor agonist) (Yokoi et al. 2002) and is relatively tolerable. Several small-scale studies have shown the potential of aripiprazole as a promising candidate for the treatment of TD (Yoo et al. 2007; Cui et al. 2010; Yoo et al. 2011). However, the effectiveness and tolerability profile of aripiprazole in the reduction of tics in children and adolescents with TD have not been systematically analyzed.
Here, we performed a meta-analysis focusing on children and adolescents with TD who had been treated with aripiprazole. Our data indicated that there was symptom improvement from pretreatment to posttreatment in the child and adolescent patients with TD.
Materials and Methods
Literature search, selection, and data collection
Studies regarding pediatric TD patients treated with aripiprazole that were listed in PubMed and Web of Science between January 2000 and November 2014 were included in this meta-analysis. The following search terms were used:
Data abstraction and analysis were performed by two different researchers (Z.W., Y.L.) and were reported on standardized forms. The pretreatment and posttreatment mean and standard deviation (SD) of the Yale Global Tic Severity Score (YGTSS) total tic scores and the Clinical Global Impressions Scale for Tic Severity (CGI-S) scores were assessed as efficacy outcome measures. Additional subgroup analyses were performed in an attempt to gain more insight into the parameters or conditions that might improve outcomes in the future. The subgroup analyses included study design, publication year, follow-up duration, and dosage, as well as ethnicity.
Data analysis
The primary efficacy measure was the mean change from pretreatment to posttreatment in the total scores for the YGTSS and CGI-S, which were the most frequently used scales in the OTs and RCTs included in the present meta-analysis. The effect sizes for primary efficacy measures in each study were presented as the standardized mean difference (SMD) with a 95% confidence interval (CI). According to a previous description (Sockol et al. 2011), the SMD calculations were based on the following: 1) (Meanpost−Meanpre)/pooled SD, where the pooled SD is defined as
A random-effects model or a fixed-effects model was used to combine subgroups to yield the overall effect. The choice of model was based on the results of a heterogeneity test, which employed the previously described Q statistic and I2 index (Sockol et al. 2011). If the Q test reported a p value <0.1 or I2 > 50%, substantial heterogeneity was considered to exist among the effect sizes, and a random-effects model was used. In addition, when statistical heterogeneity occurred, subgroup analyses were used to explore possible reasons for the heterogeneity, according to previous descriptions (Sockol et al. 2011).
Publication bias was tested using Begg's funnel plot and Egger's test (Egger et al. 1997). If the funnel plot was asymmetric, and Egger's test reported a p value <0.05, publication bias was probable.
Here, we performed all of the analyses using Comprehensive Meta-Analysis version 2.0 (CMA v2, Englewood, NJ) and STATA version 12.0 software (STATA Corporation, College Station, TX).
Results
Search results
The final search, which took place on November 30, 2014, resulted in 122 articles. Articles were excluded because of duplication, an unrelated topic, incorrect publication type (case report or review), non-English language, or unrelated assessment method. Finally, 10 articles were included in this meta-analysis (Murphy et al. 2005; Yoo et al. 2006, 2007; Seo et al. 2008; Lyon et al. 2009; Murphy et al. 2009; Cui et al. 2010; Yoo et al. 2013; Ghanizadeh and Haghighi 2014; Ho et al. 2014); these articles included 302 pediatric and adolescent TD patients who had been treated with aripiprazole. The review process is depicted in Figure 1, following previously published reporting recommendations (Moher et al. 2009). Of the studies, nine were OTs, and one was an RCT.

Flowchart of study inclusion.
Study characteristics
The average number of participating patients per study was 30 ± 25 (range, 6–81), and the mean age was 11.6 years (range, 4–19 years). The median follow-up duration for all of the studies was 9 weeks (range, 6–14 weeks). Of the studies, nine were OTs, and one was an RCT. The average daily dose of aripiprazole, the safety end-point, and the efficacy end-points for each individual study are listed in Table 1.
NP, not provided; OT, open trial; RCT, randomized controlled trial; ESRS, Extrapyramidal Symptom Rating Scale; YGTSS, Yale Global Tic Severity Scale score; CGI-I, Clinical Global Impressions-Improvement scale; CGI-S, CGI-Severity of Illness scale; CGI-Tics, the Clinical Tic Severity Scale for tics scale; CY-BOCS, Children's Yale-Brown Obsessive Compulsive Scale, CBCL, Child Behavior Checklist.
YGTSS
Effect size analysis was performed for the outcome YGTSS total tic score (10 studies), as sufficient data were available. All studies demonstrated significant negative effects, indicating improvement in, and not a worsening of, TD symptoms based on clinical scale scores, with the effect size ranging from −1.34 to −2.63. The overall effect size was −1.99 (95% CI = [−2.26]–[−1.72], p < 0.001; Fig. 2). We also performed a subgroup analysis by grouping the trials into OTs and RCTs, and the results showed that the overall effect sizes of the OTs and RCTs were −2.03 (95% CI = [−2.32]–[−1.74] and −1.71 (95% CI = [−2.15]–[−1.28]), respectively (Fig. 2).

Forest plot of primary efficacy measure of the Yale Global Tic Severity Score (YGTSS) total tic scores. The effect sizes for the primary measure in each study were presented as standardized mean differences, and a random effect model was used. ES, effect size; CI, confidence interval; OT, open labeled trial; RCT, randomized controlled trial.
The Q statistic indicated that there was significant heterogeneity among the effect sizes (p < 0.05). The I2 value indicated a substantial level of heterogeneity, with 57.8% of the variance in the effect size attributable to between-study variance. Exploratory analyses of potential moderators were conducted. Five characteristics of the included studies were assessed as potential moderators: Study design, year of publication, duration, dosage, and country (Table 2). No significant difference in the average effect size was found among the study design type, study duration, dosage and country. Studies for which the effect size was calculated using a publication year before 2010 had significantly larger effect sizes (g = 1.69, n = 6) than did studies for which the effect size was calculated using a publication year after 2010 (g = 1.13, n = 4).
CI, confidential interval; df, degrees of freedom; OT, open label trial; RCT, randomized controlled trial.
Significant difference.
CGI-S
Effect size analysis was performed for the outcome CGI-S score (three studies), as sufficient data were available. All studies demonstrated significant negative effects, indicating improvement over pretreatment, with effect sizes ranging from −2.19 to −2.76. The overall effect size was −2.34 (95% CI = [−2.96]–[−1.73], p < 0.001; Fig. 3).
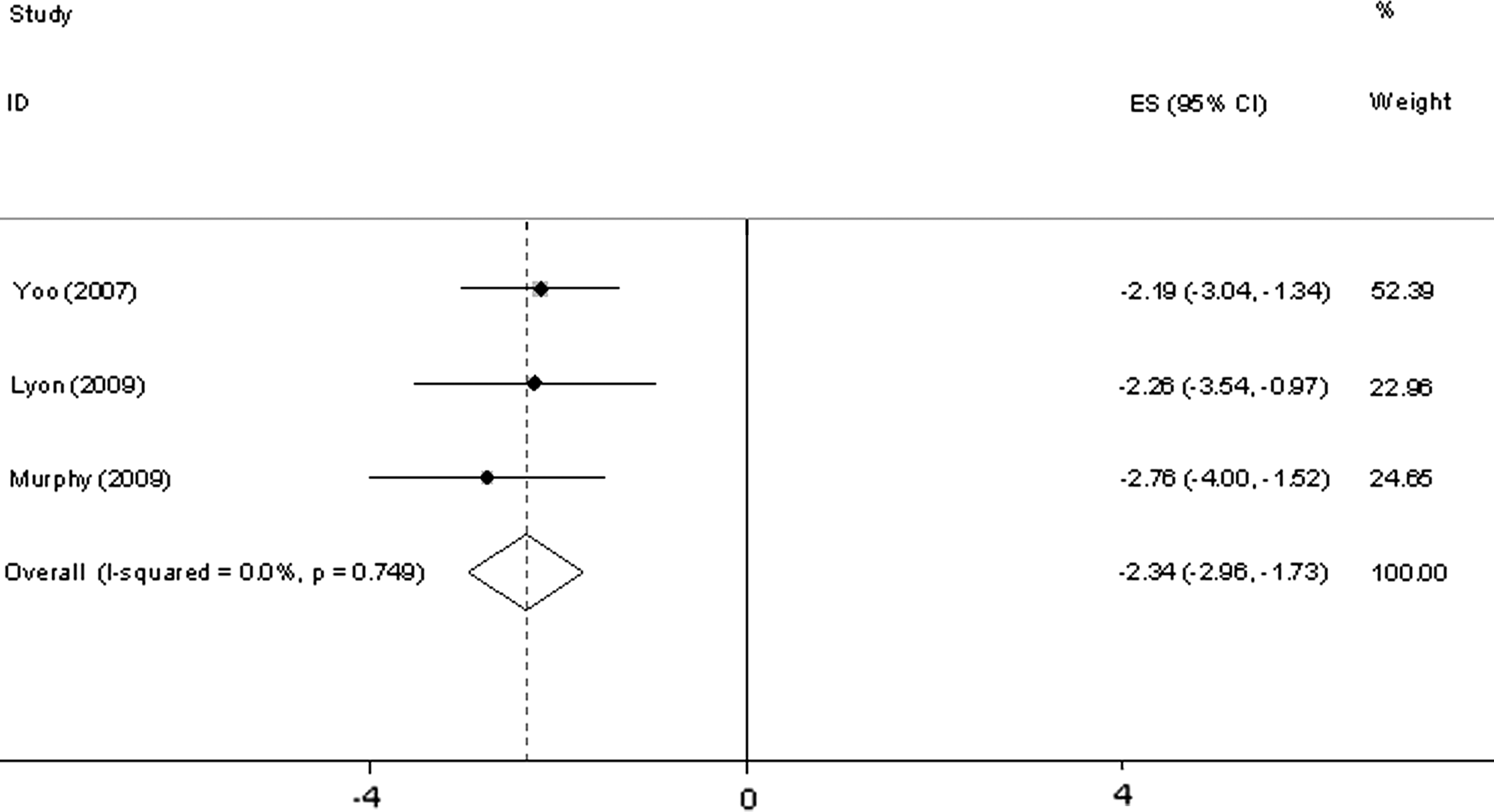
Forest plot of of primary efficacy measure of the Clinical Global Impressions Scale for tics (CGI-Tic) severity scores. The effect sizes for the primary measure in each study were presented as standardized mean differences, and a random effect model was used. ES, effect size; CI, confidence interval.
Tolerability
We analyzed the incidence of adverse events in the included studies, and the results are shown in Table 3. Sedation (or drowsiness), nausea (or gastrointestinal upset), and headache were the most common adverse events. The incidence of sedation (or drowsiness), nausea (or gastrointestinal upset), and headache were 28.5% (69/242), 20.2% (59/291), and 13.8% (22/159), respectively. In addition, we examined the number of patients who dropped out in each study, and the total dropout rate was 6.6% (20/302).
Yoo 2013 is a randomized controlled trial.
Publication bias
Begg's funnel plot for the YGTSS showed that the studies were equally distributed around the overall estimate (Fig. 4). Moreover, Egger's test showed no publication bias (p = 0.462).
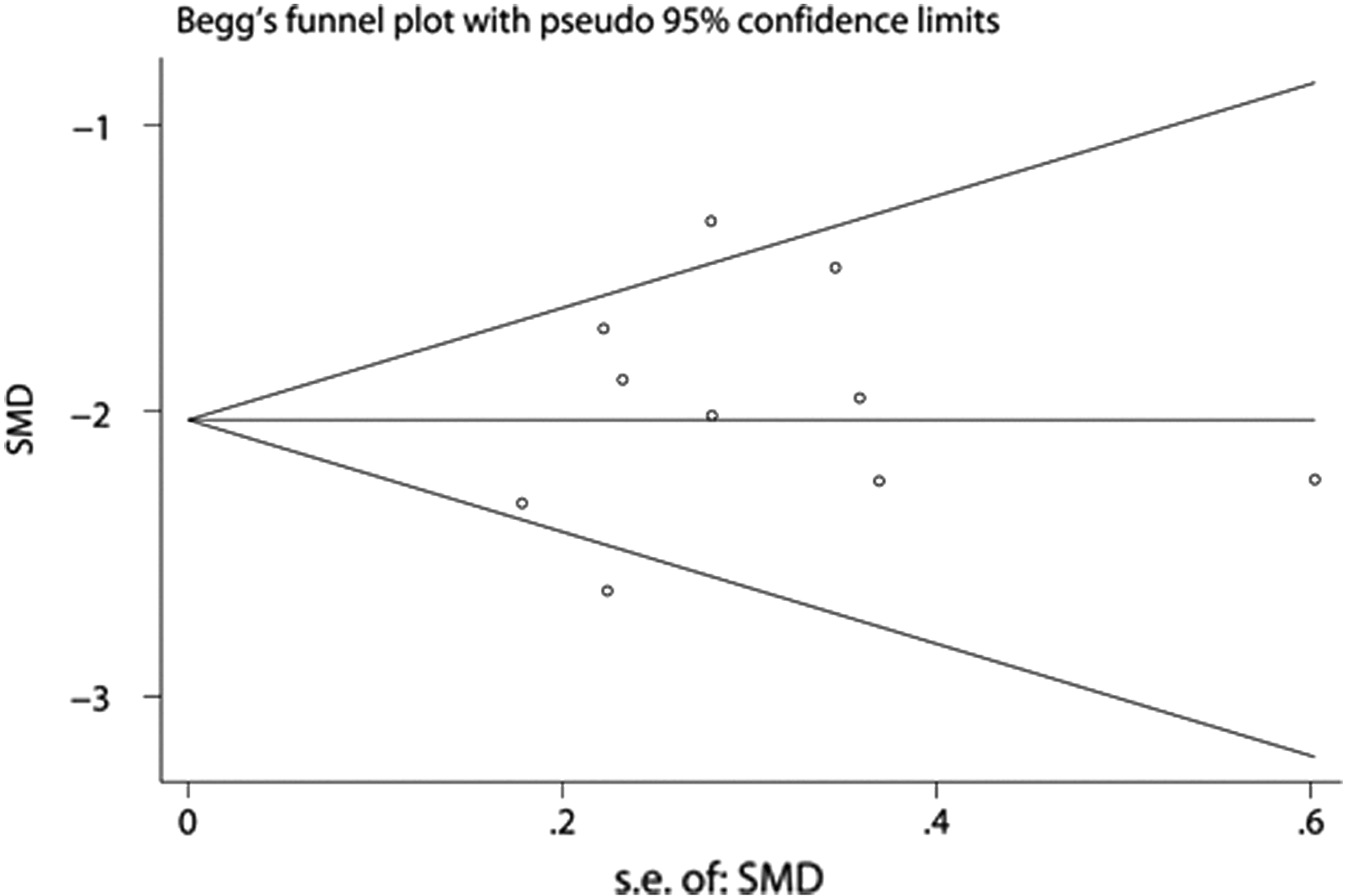
Begg's funnel plot for the Yale Global Tic Severity Score (YGTSS) total tic scores. logor, logarithm of odds ratio; s.e., standard error.
Discussion
In this study, the results of the above analyses provided evidence for the efficacy of aripiprazole in children and adolescents with TD. All of the OTs demonstrated symptomatic improvement starting after the treatment with aripiprazole, and the only RCT also demonstrated superiority to control conditions. The overall effect size was −1.99 (−2.26 to −1.73; mean change in the YGTSS total tic score). To the best of our knowledge, this is the first meta-analysis on the efficacy of aripiprazole in children and adolescents with TD.
We included 10 studies in this meta-analysis. Of the 10 studies, 9 were OTs, and only 1 RCT was included. A small proportion of RCTs could result in inaccurate baseline data, and ultimately lead to exaggeration of the efficacy of aripiprazole. However, with the help of reasonable calculation methods, our data may reflect the true therapeutic effect of aripiprazole.
Currently, the YGTSS is the most commonly used outcome measure for TD (Jankovic et al. 2010; Gabbay et al. 2012; Kurlan et al. 2012); other measurement scales include the CGI, the Global Severity Score, and Children's Yale-Brown Obsessive Compulsive Scale (CY-BOCS) (Yang et al. 2013). In our study, all 10 studies used the YGTSS for outcome measurement, and 3 studies used the CGI-S for outcome measurement, whereas the other measurement scales were employed in fewer than 3 studies. Therefore, we synthesized the data for the YGTSS total tic scores and the CGI-S scores to obtain the effect size data.
The Q test and I2 results for the overall YGTSS total tic score showed that substantial heterogeneity might exist among the effect sizes; therefore, we performed a subgroup analysis to explore the possible reasons. Three types of moderators were included in our analyses: the first were variables that reflected elements of research design; the second were variables related to characteristics of interventions, such as treatment duration and dosage; and the third were variables related to characteristics of the study, such as publication year and country of origin. No significant difference was found in the effect size when study design, treatment duration, dosage, or country of origin was used. However, studies for which the effect size was calculated using a publication year before 2010 had significantly larger effect sizes (g = 1.69, n = 6) than did studies using a publication year after 2010 (g = 1.13, n = 4).
Limitations
The limitations of our study included the following. 1) The number of RCTs was limited. The databases searched in the present meta-analysis were confined to PubMed and Web of Science, which encompass published journal articles; therefore, we could not collect all of the available clinical trial data. However, no publication bias was found. 2) The data on metabolic syndrome-type side effects were limited. These side effects are viewed as being more common with atypical antipsychotics, particularly aripiprazole. 3) The longest follow-up duration was 14 weeks, which could have resulted in a lack of a long-term effect. 4) CGI-S data were only available in three studies; therefore, we were not able to achieve multiple verification.
Conclusions
In conclusion, the use of aripiprazole is well tolerated and shows therapeutic effectiveness in children and adolescents with TD. However, further high-quality, randomized, placebo-controlled trials are needed to confirm these results.
Clinical Significance
This article presents a meta-analysis of aripiprazole in children and adolescents with Tourette's disorder. We searched for clinical trials using aripiprazole to treat Tourette's disorder in children and adolescents patients, and we pooled the data on YGTSS total tic score, and the CGI for tics (CGI-Tic) severity scores to assess the state of the evidence for the effectiveness and tolerability of aripiprazole treatment.
Footnotes
Disclosures
No competing interests exist.