
Abstract

To The Editor:
N
Case Report
The patient was an 11-year-old Hispanic male with no history of significant medical illnesses and a past psychiatric history of attention-deficit/hyperactivity disorder (ADHD), pervasive developmental disorder (PDD), and posttraumatic stress disorder (PTSD) secondary to severe physical abuse by his stepfather. This patient presented to the emergency room with complaints of increasing irritability accompanied by violent, aggressive, and impulsive behavior. He had experienced one prior inpatient psychiatric hospitalization of 11 days for similar behavior. His mother had a history of clinical depression, for which she had received psychopharmacological treatment in the past. At presentation, our patient had already been compliant with outpatient treatment, including risperidone 0.5 mg p.o. twice daily, and lisdexamfetamine 40 mg p.o. daily. He was admitted to the inpatient children's unit for evaluation and further management. Admission blood testing revealed significant neutropenia; his WBC and ANC were 4.3 × 109/L (normal range 5.3–15.0 × 109/L) and 1.0 × 109/L (normal range 1.5–8.0 × 109/L), respectively. Risperidone was immediately discontinued, and the patient was carefully monitored for signs and symptoms of possible infection. The decision to immediately discontinue risperidone was based on his clinical picture and United States Food and Drug Administration (FDA) advisory committee recommendations; the general consensus for managing an abrupt drop in ANC or severe neutropenia (ANC < 1.0 × 109/L) during treatment with risperidone is immediate discontinuation of the medication (Risperdal® package insert 2012).
After discontinuation of risperidone, the patient's WBC and ANC levels returned to the normal range in 4 days (ANC 2.0 × 109/L and WBC 4.7 × 109/L), but irritability, anger, and aggression gradually worsened. He was continued on lisdexamfetamine. On Day 10, aripiprazole treatment was initiated, based on reports of its benefit in management of irritability and aggression in PDD (Politte and McDougle 2014). The safety of this treatment appeared more favorable than alternative approaches given the lack of previous reports of neutropenia associated with aripiprazole as monotherapy, and because aripiprazole has a different chemical structure (dihydroquinolinone) than risperidone, clozapine, olanzapine, and quetiapine (Wilson and Offenberger 2013). Importantly, several case reports have suggested that aripiprazole can be used in management of antipsychotic-induced neutropenia (Nair and Lippmann 2005; Yalcin et al. 2008). On the day aripiprazole was initiated, his WBC and ANC were 5.8 × 109/L and 2.0 × 109/L, respectively. Following initiation at 2 mg p.o. daily, the dose was increased to 4 mg p.o. daily within 1 week. The following week, his WBC and ANC had declined to 4.1 × 109/L and 1.4 × 109/L, respectively. Two days later, WBC and ANC levels decreased further to 4.0 × 109/L and 1.2 × 109/L, although the patient did not show any signs of infection, and his disruptive behaviors started to show some improvement.
In the context of published reports of diurnal variation in neutrophil counts for adults on neuroleptic medications (Hummer et al.1994; Ahokas and Elonen 1999; Esposito et al. 2003,\ 2005; Singh and Kodela 2009), complete blood counts with differential were performed at both 08:00 hours and 15:00 hours. on 6 days during a 2 week period. The patient continued taking aripiprazole during this time. His WBCs were consistently between 4.1–5.2 × 109/L in the morning and 4.8–6.0 × 109/L in the afternoon. His ANCs were between 1.2–1.6 × 109/L in the morning and 1.8–2.8 × 109/L in the afternoon, suggesting transient pseudoneutropenia in the morning (Fig. 1).
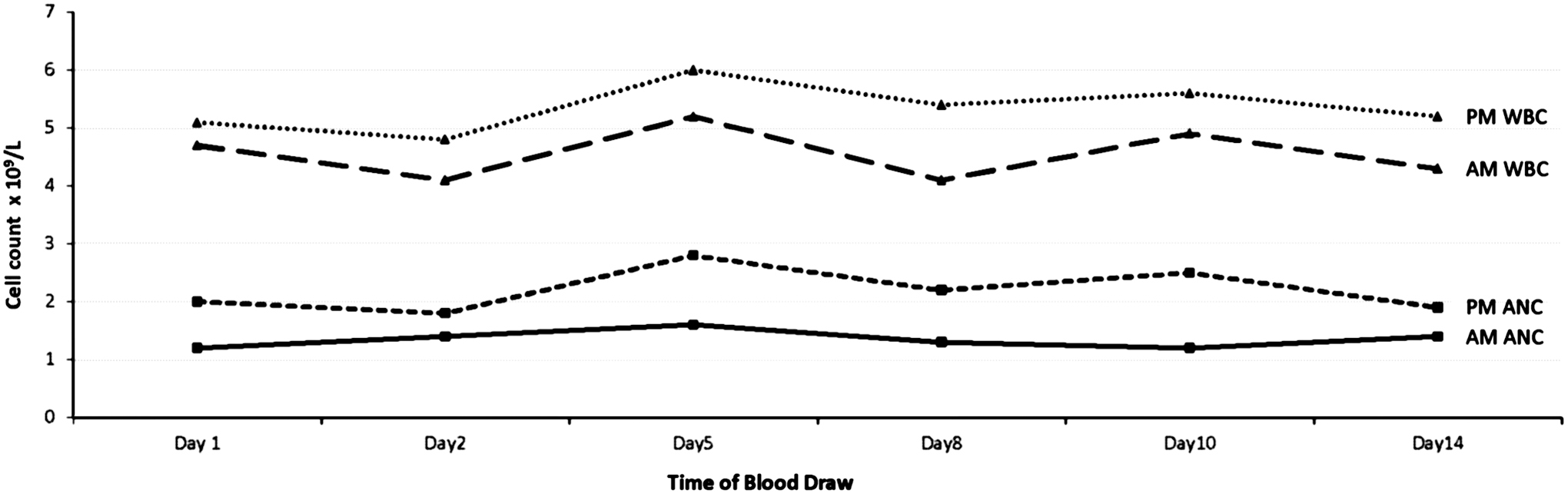
Morning (a.m.) and afternoon (p.m.) white blood cell (WBC) and absolute neutrophil counts (ANC) during a 2 week period while taking aripiprazole.
Discussion
In agranulocytosis, neutrophil precursors and mature neutrophils are affected, whereas in mild to moderate neutropenia, only peripheral cells are affected (Whiskey and Taylor 2007). It is hypothesized that compensatory mechanisms including cytokines, such as granulocyte colony-stimulating factor, may stimulate granulopoiesis sufficiently in cases of transient neutropenia. If the cytokine compensation is insufficient, neutropenia may become significant and even progressive (Hummer et al. 1994).
Levels of circulating blood cells exhibit circadian variations in healthy individuals; WBC have more diurnal variation than red blood cells, likely because of the high turnover rate for these cells. These intraindividual biological variations are not clinically significant at the upper end, but may be noted or become clinically relevant at the lower end of the reference interval (Sennels et al. 2011).
Little is known regarding the mechanism of neuroleptic-induced transient neutropenia. It has been hypothesized that clozapine may amplify the diurnal variations in circulating neutrophils by affecting the endogenous production of hematopoietic cytokines (Hummer et al. 1994). This explanation may also apply to other neuroleptic medications, including aripiprazole.
Previous reports suggest that patients with transient neutropenia are not categorically predisposed to developing agranulocytosis. Therefore, it is crucial to differentiate between transient pseudoneutropenia and persistent malignant neutropenia. If morning levels are below the normal range, WBC and ANC should be checked systematically in the afternoon or evening on the day of morning blood assays, to evaluate for pseudoneutropenia. The risks of medication discontinuation should be weighed against potential risks of side effects when pseudoneutropenia is encountered. Because it is important to monitor for progressive development of leukopenia and potential agranulocytosis, to ensure safety, WBC and ANC counts should be repeated regularly for patients who have low levels early in the course of treatment with neuroleptic medications.
Footnotes
Acknowledgments
The authors thank the patient who provided assent and the mother (legal guardian) of the patient, who provided consent for both research and anonymous publication.
Disclosures
Drs. Pinnaka, Roberto, Giordano, and Siller received no financial support and have no other disclosures. Dr. Lapidus received research support from the Brain and Behavior Research Foundation, Education and Research Foundation for Nuclear Medicine and Molecular Imaging, Le Foundation, and Simons Foundation; serves on the advisory board for Halo Neuroscience; has received travel support from Brainsway and devices from Medtronic and Halo Neuroscience; and consults for LCN Consulting, Inc.