
Abstract
Objective:
Clinical reviews of practice outcomes of adolescent patients who have received electroconvulsive therapy (ECT) remain relatively rare. This study reports the clinic practice and outcome of adolescents receiving ECT at a tertiary medical center.
Methods:
From April 1991 through November 2013, 51 adolescents (30 female; mean [SD] age, 16.8 [1.6] years) received ECT. The electronic medical record at the time of the first ECT session was reviewed for the clinical diagnosis, ECT lead placement and general administration, seizure duration, adverse effects, concurrent medications, and clinical outcome.
Results:
ECT was recommended for primary mood and psychotic disorders or catatonia. Patients received a mean (SD) of 9.3 (3.5) treatments, with initial bitemporal lead placement in 36 patients (71%). Thirty-nine patients (77%) were much or very much improved based on Clinical Global Impressions–Improvement scale at the end of the acute treatment. Prolonged seizure duration (>120 seconds) was relatively common (63%) but appeared to decrease in older patients.
Conclusions:
This report describes the largest group of adolescents receiving ECT since 1947, and supports ECT as a safe and effective modality for most treatment-recalcitrant psychiatric illness in youth.
Introduction
I
Research and adoption of ECT use in youth remains a challenge, because of substantial drug development for pediatric and adolescent depression, bipolar disorder, and schizophrenia over the past decade (i.e., United States Food and Drug Administration [FDA] approval of fluoxetine and escitalopram [for major depression]; lithium, risperidone, and aripiprazole [for bipolar disorder]; and risperidone and aripiprazole [for schizophrenia]) and, more importantly, because of the lack of systematic clinical investigation of ECT in nonadult populations. To address this challenge, we reviewed the practice approach and outcome of 51 adolescents treated with ECT over the past 20 years at a tertiary medical center.
Methods
This retrospective study waiver of informed consent was approved by our institutional review board. We identified adolescent patients (12–19 years of age) who underwent at least one ECT session from April 8, 1991, through November 11, 2013.
All patients were initially inpatients and were evaluated by a board-certified attending child psychiatrist of record for hospitalization. Most patients also received two additional consultations with nontreating board-certified child psychiatrists before initiation of ECT. Per institutional policy, minors were allowed to undergo ECT only with consensus of these separate providers regarding suitability and safety of the treatment. All patients underwent a comprehensive preanesthesia medical examination to ensure medical suitability to undergo ECT.
ECT was performed as previously described (Pullen et al. 2011). Electrode placement was either bitemporal, right unilateral, or bifrontal. A Thymatron System IV ECT apparatus (Somatics, Inc) was used to deliver the electrical pulse. Seizure duration was monitored and recorded centrally via electroencephalography and peripherally (i.e., motor seizure) by placing a blood pressure cuff on the patient's distal extremity before succinylcholine administration.
Data from the first course of ECT were abstracted from the electronic medical record or from paper medical record charts. Abstracted data included sex, age, ethnicity, psychiatric diagnosis, psychotropic medication trials, and temporal clinical response to ECT. Given the 2011 FDA Neurologic Devices Panel's recommendations for differential risk classification of ECT devices when used to treat catatonic patients, patients who received ECT for catatonic syndromes were also identified (United States Food and Drug Administration 2011). Data abstraction was performed consistent with guidelines outlined by Gearing and colleagues (2006). Two authors independently reviewed all available clinical records for a description of symptoms, diagnoses, and rationale for ECT use. When available, symptoms before, during, and after treatment were noted. To standardize clinical severity and impairment, the Clinical Global Impressions–Severity (CGI-S) and Clinical Global Impressions–Improvement (CGI-I) scales (Guy 1976) were retrospectively quantified by review of the medical record.
Results
Fifty-one patients were included in this study (30 female; age range, 12–19 years; mean [SD] age, 16.8 [1.6] years). Patients were predominantly white (n = 48 [94%]), with one patient each of African, Asian, and Hispanic ancestry. The primary affective (n = 33 [65%]) and psychotic (n = 9 [18%]) disorder diagnoses for which ECT was indicated included major depressive disorder (n = 21), major depression with psychosis (n = 6), bipolar affective disorder manic/mixed (n = 3), schizoaffective depression (n = 2), schizoaffective bipolar disorder (n = 1), schizophrenia (n = 1), corticosteroid-induced psychosis (n = 1), and psychosis not otherwise specified (n = 7). ECT was also indicated for catatonic syndromes (n = 9 [18%]). Treatment resistance to at least two adequate medication trials for the index episode of illness was identified in the majority of patients (n = 45 [88%]). Six patients (12%) were given emergent ECT before having two failed medication trials for indications including psychosis (n = 1), catatonia (n = 4), and major (severe) depressive disorder (n = 1).
Treatment characteristics
The majority of patients (n = 36 [71%]) were treated with bitemporal electrode placement. Right unilateral (n = 11 [22%]), bitemporal plus right unilateral (n = 3 [6%]), and bifrontal (n = 1 [2%]) electrode placement occurred less frequently. Treatment was typically initiated at a setting of 5% maximum output, and was subsequently titrated on the basis of seizure duration. The modal final treatment setting was 30% (range, 10–100%). Most commonly, patients required only one course of treatment (n = 47 [92%]), although a second course (i.e., resumption of ECT after at least 1 month without treatment) was identified in four cases (8%). One patient received court-ordered maintenance ECT treatments over a period of 12 weeks. Treatments were administered weekly for the first 6 weeks and every other week for the following 6 weeks. No subsequent maintenance treatments occurred following the expiration of the court order. Patients required a mean (SD) of 9.3 (3.5) treatments (range, 4–23 sessions) during their initial treatment series; the four patients with a second treatment course required a mean (SD) of 11.5 (2.3) treatments (range, 9–15 sessions) for a relapse of symptoms. The mean (SD) seizure duration measured by electroencephalography was 84.4 (56.2) seconds (range, 16–600 seconds). The mean (SD) peripheral motor seizure duration was 43 (23.8) seconds (range, 0–197 seconds).
As shown in Figure 1, seizure duration was inversely related to age. Prolonged seizures, variably defined as a central seizure duration >120 seconds (Scott et al. 2005) or 180 seconds (Ghaziuddin et al. 2004), were relatively common, with 32 patients (63%) having at least one seizure exceeding 120 seconds and 20 patients (39%) having at least one seizure >180 seconds. Of the 506 recorded seizure events in this patient population, 108 (21%) were >120 seconds and 33 (7%) were >180 seconds.
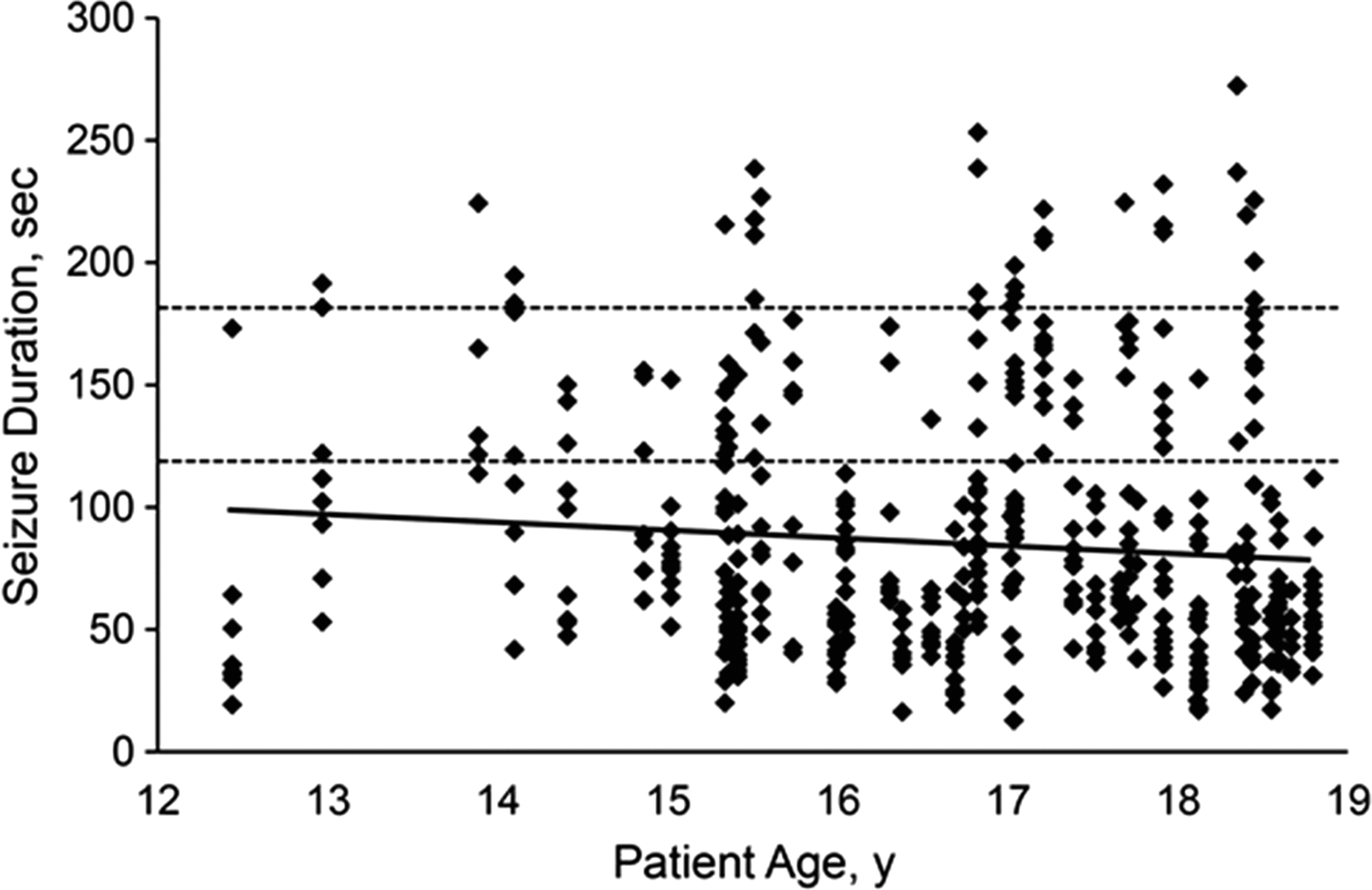
Seizure duration, stratified by patient age. Duration was determined by electroencephalography. The dashed lines indicate the threshold for prolonged seizures (variably defined as central seizure duration longer than 120 seconds or 180 seconds). The solid line is a linear trend line for this data series (applied through Excel software [Microsoft Corp]).
Medications
We noted the medications prescribed at the time of ECT (n = 51) and at 1 year after ECT (n = 29). The mean (SD) number of concurrent medications at initiation of ECT was 2.8 (1.1) (Fig. 2). Atypical antipsychotics were the most common class of psychotropic medications prescribed to patients undergoing ECT (n = 33 [65%]), followed by selective serotonin reuptake inhibitors (SSRIs) (n = 30 [59%]), non-SSRI antidepressants (n = 27 [53%]), benzodiazepines (n = 17 [33%]), mood stabilizers (n = 15 [29%]), typical antipsychotics (n = 11 [22%]), and other medications (n = 7 [14%]).

Concurrent medications at initiation of electroconvulsive therapy.
Of the patients with available follow-up data 1 year after ECT, 12 of 29 patients (41%) were receiving one less medication, 6 patients (21%) were receiving two fewer medications, and 1 patient (3%) was receiving three fewer medications. Six patients (21%) had no change in the number of active medications. Three patients (10%) were receiving one more active medication 1 year after ECT, and one patient (3%) was receiving two more medications. Overall, patients were receiving a mean (SD) of 0.76 (1.1) fewer medications 1 year after ECT.
Adverse effects
Nausea was the most common adverse event, affecting eight patients (15.7%). Headaches (n = 7 [13.7%]), postemergence agitation (n = 4 [7.8%]), spontaneous seizure (n = 2 [3.9%]), urinary retention (n = 1 [2.0%]), and status epilepticus (n = 1 [2.0%]) were less common. Information regarding cognitive impairment and memory disruption was not collected because of the lack of formal, objective measures of cognitive performance across subjects.
CGI Ratings
As presented in Figure 3, mean CGI-S scores improved after treatment for all patient groups, with mean (SD) CGI-I scores of 2.00 (0.71), 2.05 (0.86), and 2.09 (0.95), for patients with psychotic, affective, and catatonia disorders, respectively. Similarly, the mean change from preceding phase or CGI-I was ∼2.0 (much improved) for the psychosis, affective, and catatonic subgroups (Fig. 3). At the end of acute treatment, 39 patients (77%) were much or very much improved based on CGI-I scores. Although five patients were thought to have no measurable change in symptoms during the ECT course, no patients had symptoms worsen as a result of ECT.
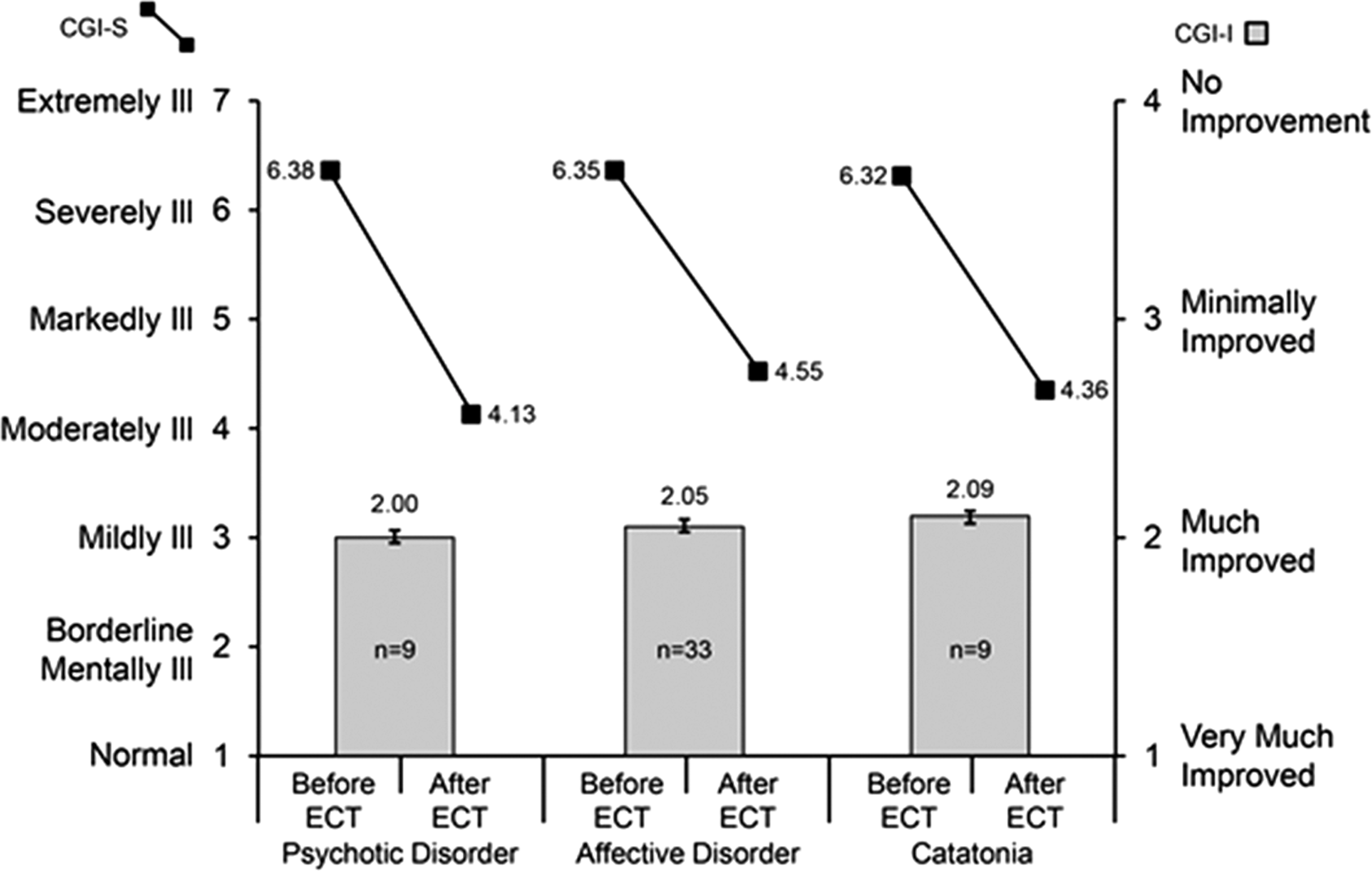
Average CGI‐S and CGI‐I scores in adolescents receiving ECT. CGI-I, Clinical Global Impressions–Improvement; CGI-S, Clinical Global Impressions–Severity; ECT, electroconvulsive therapy.
Discussion
ECT is most often used for patients with severe, treatment-resistant depression or during life-threatening circumstances (e.g., catatonia, suicidality, malnourishment). The clinical outcomes documented for this group of 51 adolescent patients who received ECT suggest that it is an effective, safe, and tolerable treatment for patients with severe, life-threatening psychiatric symptoms. Notably, the patients in this study had severe symptoms, with most categorized as severely ill (n = 28 [55%]) or most extremely ill (n = 20 [39%]). The severity of disease also reflected a high degree of treatment resistance, given the common practice of considering ECT only after intensive psychiatric interventions that included hospitalization, aggressive psychopharmacology, and/or psychotherapy. Within 2–3 weeks after treatment, most of the adolescents showed dramatic improvement in symptoms, with the most frequent posttreatment CGI-S rating being moderately ill. Although complete resolution of psychiatric symptoms did not often occur during the acute course of ECT, patients frequently were able to resume outpatient care. Per the available medical records and to our clinical knowledge, none of the patients died of psychiatric symptoms or suicide during a mean follow-up period of 3.6 years (maximum, 16.5 years). Further, reduction in psychotropic medication burden was also common after ECT, indicating both improvement and confidence in the outcome by the treating physicians.
On the basis of our clinical experience, the earlier work of Schneekloth and colleagues (1993), and the results of this review, ECT clearly should be seriously considered and used in adolescents as a means of reducing severe psychopathology that is not amenable to other treatment approaches. We note that the prevalence of adverse effects in the study population mirrored data previously reported in adolescent and adult populations (Devanand et al. 1995; Rey and Walter 1997). This review confirms the opinions expressed by Lima et al. (2013) that ECT use in adolescents is a highly efficient option for treating several psychiatric disorders, achieving high remission rates. We also agree with Croarkin et al. (2009) that it is important to rigorously and prospectively study treatment outcomes to provide a more robust understanding of the biologic, psychologic, and social impacts of ECT as an intervention in severe adolescent psychopathology.
Despite these positive findings, the current review has a number of limitations related to the nature of retrospective analyses. Rating scales were not applied consistently by treating physicians at the time of treatment. Consequently, we retroactively applied CGI ratings on the basis of the clinical documentation available for review, which often appeared to be subjective. Although the ratings were independently applied, the results remain subject to confirmation bias from the treating physicians.
Despite good evidence supporting the efficacy and safety of this intervention, it continues to be at the bottom of treatment algorithms, which may unnecessarily prolong treatment of severely ill children and adolescents. Additional barriers to treatment include considerable stigma associated with public perception of ECT, compounded by relative inexperience and lack of confidence in prescribing or providing ECT, as reported by many child and adolescent psychiatrists (Parmar 1993; Walter et al. 1997; Ghaziuddin et al. 2001). However, when ECT is offered to patients with severe mental illness, research suggests that most adolescents (69%) would undergo treatment again if it were advised by their physician (Walter et al. 1999a). Further, many patients and their parents viewed ECT as less aversive than the illness itself, and 77% would recommend the treatment to others (Walter et al. 1999a,b).
Adding to the cautious use of ECT in youth is concern about long-term outcomes and adverse effects associated with ECT, particularly in the developing brain. Cohen and colleagues (23) reported no measurable cognitive impairment 3.5 years after ECT. Taieb and colleagues (2002) reported that 11 adolescents who received ECT for bipolar disorder did not differ in subsequent school and social function 5 years later when compared with carefully matched controls. To our knowledge, no reports have been published that describe long-term outcomes such as alteration of disease course as it relates to subsequent psychiatric diagnoses, rehospitalization, medication burden, or suicidality.
Adverse effects
ECT is not benign; however, the observed adverse effects were generally transient. The most commonly reported treatment-related effects included nausea, headaches, postanesthesia agitation, and spontaneous seizure. The paucity of formalized neurocognitive testing before and after treatment precludes our ability to provide more insight into the effect of ECT on cognition in adolescents. However, the clinical notes suggest that the physicians, nurses, and families did not report notable disturbances in memory during or after ECT. This is important to note because 36 patients (71%) had bitemporal electrode placement, which has been implicated in retrograde autobiographical amnesia (Weiner et al. 1986). Although we are unable to definitively conclude that ECT is less likely to have dramatic effects on memory and cognitive function in youth, the clinical records suggest good cognitive tolerability in this population. Furthermore, a systematic focus by Cohen and colleagues (2000) reached a similar conclusion about the cognitive effects of ECT in adolescents. Current American Academy of Child and Adolescent Psychiatry guidelines suggest that every adolescent undergoing ECT must have a memory assessment before treatment, at treatment termination, and at an appropriate time after treatment (Ghaziuddin et al. 2004). Unfortunately, no tools have been recommended for memory assessment, possibly because little consensus exists on the type, scope, and validity of memory assessment tests in this particular population.
Conclusions
In adolescents with severe psychiatric symptoms (eg, catatonia, psychosis, mania) or severe, recalcitrant depression and suicidality, the most common and widely available interventions are hospitalization, psychotherapy, and psychopharmacology. However, these interventions may require months of treatment at a time when efficacy and time are of paramount concern and ultimately yield limited to modest results (Weisz et al. 2006; Bridge et al. 2007).
Despite nearly 70 years of scientific evidence of both safety and efficacy of ECT in adolescents, it remains underutilized. As stated by Fink et al (2014), “concerns about the use of ECT by child and adolescent psychiatrists and governmental restrictions on its use in adolescents, ECT is often not an option [in many psychiatric treatment settings]. The growing successful experience in these age groups suggests that ECT does warrant increased and early consideration, as well as removal of the legal impediments to the treatment.” When comparing this relatively safe and rapidly effective treatment approach against prolonged titration and manipulation of multiple psychopharmacologic agents and prolonged psychiatric hospitalization, as well as the psychosocial consequences of untreated illness in adolescence, the rationale for ECT is sound and should be confidently discussed and offered as a potentially life-saving treatment intervention.
Footnotes
Disclosures
No competing financial interests exist.