
Abstract
Background:
Prescriptions of antipsychotic drugs (AP) in children and adolescents have significantly increased in Europe as well as in the United States. However, there is limited evidence of the cardiac safety of second-generation antipsychotics (SGA) in the pediatric population.
Objective:
The aim of the study is to evaluate the cardiac side effects of SGA in children and adolescents, and how they are influenced by clinical, demographic, and treatment factors.
Methods:
This article presents a naturalistic, longitudinal, multicenter study conducted in 216 treatment-naïve or quasi-naïve children and adolescents receiving AP treatment. It analyzed the possible influence of AP treatment on variables such as corrected QT (QTc) intervals and heart rate for a period of 12 months (baseline, 3 months, 6 months, and 12 months). Differences among the three main prescribed drugs used in the sample (risperidone, quetiapine, and olanzapine) were assessed.
Results:
A total of 211 received one of the three most prescribed AP (quetiapine, risperidone or olanzapine). There were no significant QTc variations in the sample during follow-up (p = 0.54). There were no differences in QTc rates between the different SGA (risperidone–olanzapine p = 0.43; risperidone–quetiapine p = 0.42; olanzapine–quetiapine p = 0.23). When demographic, clinical, or concomitant treatment variables were considered, only baseline overweight correlated with QTc prolongation (p = 0.003). The heart rate in the whole sample tended to decrease during follow-up (p = 0.054). However, patients on quetiapine showed increased heart rate compared with those on risperidone (p = 0.04).
Conclusions:
In this sample, SGA seem to have a safe heart side effect profile in the child and adolescent population. There was no observed mean increase in QTc or in heart rate.
Introduction
T
In the past decade, various antipsychotic drugs (AP) such as sertindole, thioridazine, and droperidol were removed from the market because of cardiac side effects (Buckley and Sanders 2000; Glassman and Bigger 2001; Fraguas et al. 2008). Other AP drugs such as ziprasidone were examined in further specific safety studies (Ziprasidone Observational Study of Cardiac Outcomes [ZODIAC Study]) (Strom et al. 2011; Camm et al. 2012), triggering an extensive debate regarding the cardiac safety of specific AP drugs (Fraguas et al. 2008). Various studies found an association between AP use and increase in corrected QT interval (QTc) (Buckley and Sanders 2000; Glassman and Bigger 2001).
Many AP drugs can, in various ways, prolong the QTc interval of the electrocardiogram and, in the presence of tachycardia, can provoke an increased risk of potentially lethal arrhythmias known as “Torsade de pointes” (Glassman and Bigger 2001; Silke et al. 2002; Alvarez and Pahissa 2010; Zuddas et al. 2011).
In children and adolescents, cardiovascular side effects associated with the use of SGA and FGA include orthostatic hypotension, tachycardia, QTc prolongation, and arrhythmias (Cheng-Shannon et al. 2004; Correll et al. 2006; Jerrell et al. 2008; Jones et al. 2013). In a study with a pediatric population, AP group, gender, age, smoking status, substance abuse, and diagnosis were unrelated to QTc change after introduction of the AP (de Castro et al. 2008).
In a recent meta-analysis of 55 studies with >5000 youth patients, the risk of pathological QTc prolongation seemed low during treatment with the nine AP studied in otherwise healthy young people. Nevertheless, because individual risk factors interact with medication-related QTc effects, both medication and patient factors need to be considered when choosing AP treatment (Jensen et al. 2015).
Although the cardiovascular side effects during treatment with AP drugs may be less common in children and adolescents than in adults (Masi and Liboni 2011), the benefit of the electrocardiogram (ECG) screening is not yet clear in the pediatric population.
Our objective is to evaluate cardiac symptoms in a large sample of treatment-naïve (no previous AP) or quasi-naïve (AP exposure for <30 days) pediatric patients for a period of 12 months.
Methods
A prospective, naturalistic, longitudinal multicenter study was conducted during a 12 month follow-up period, by analyzing the principal cardiovascular risk markers, namely QTc interval, and the main treatment-influenced factors, as well as the heart rate. The differences between the different AP were also analyzed.
Subjects
Four Spanish hospitals participated: Hospital General Universitario Gregorio Marañón in Madrid (HGUGM), Hospital Clínic in Barcelona (HC), Hospital Niño Jesús in Madrid (HNJ), and Hospital Sant Joan de Déu in Barcelona (HSJD).
Recruitment was conducted between May 2005 and February 2009. All patients seen in short-term inpatient units and outpatient clinics of each hospital during the recruitment period and who met the inclusion criteria were invited to participate in the study (for a complete description of the study design, see Merchán-Naranjo et al. 2012). Detailed descriptions of diagnoses associated with AP treatment and other AP characteristics are described elsewhere (Baeza et al. 2014).
Inclusion criteria were age <18 years at baseline, any psychiatric diagnoses from the Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) (American Psychiatric Association 1994), first prescription of any AP within 30 days prior to enrollment, and at least two visits during follow-up. At baseline, patients were classified as treatment naïve (no previous AP) or quasinaïve (AP initiated in the 30 days prior to enrollment). A total of 265 subjects were asked to participate and accepted. Patients with an eating disorder diagnosis were excluded from the analysis (n = 31) to avoid interference with cardiac effects of malnutrition. Patients who did not have any recorded QTc measurement were also excluded (n = 18). Ultimately, a total of 216 patients were analyzed (Fig. 1).
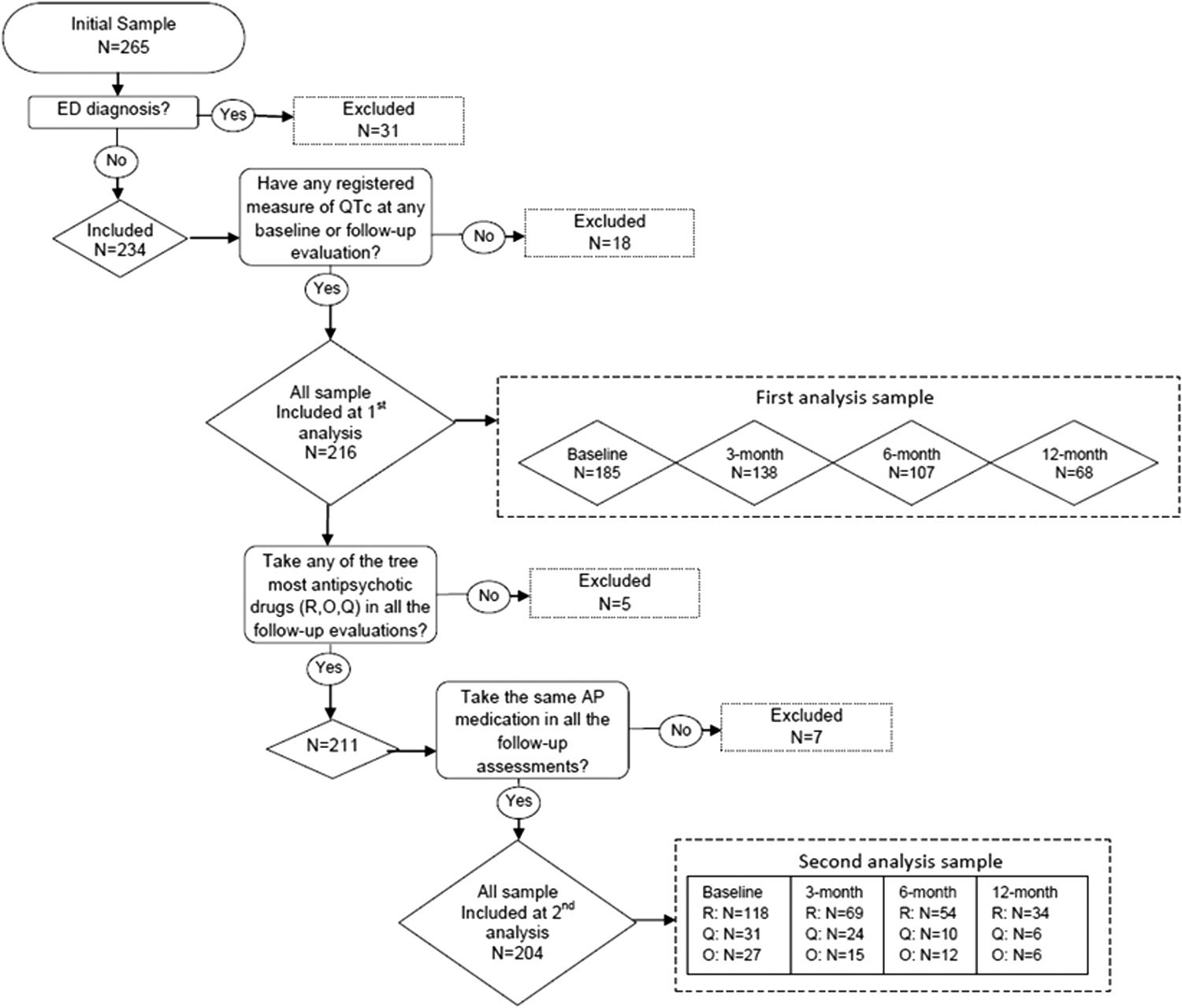
Flowchart of the analyzed sample. ED, eating disorder; R, risperidone; O, olanzapine; Q, quetiapine; AP, antipsychotic drug.
Concomitant treatment with antidepressants, anticholinergics, mood stabilizers, and benzodiazepines was permitted.
This study was approved by the ethics committees of all participating sites. All parents or legal guardians of participants gave written informed consent prior to enrollment, and subjects >12 years of age agreed to participate.
Assessment
Demographic, clinical, and treatment characteristics
Demographic and clinical characteristics of the sample were collected at baseline from parents or legal guardians and the patient. The diagnoses were made by child and adolescent psychiatrists, based on the DSM-IV diagnostic criteria.
Treatment information was evaluated at baseline and during follow-up (1, 3, 6, and 12 months) through exhaustive recording of the AP given and the dose administered. The equivalent chlorpromazine dose was calculated to compare all total cumulative doses of the different AP administered throughout the study. The concomitant medication received was also recorded.
Biological measurements
It was collected each patient's weight, height, abdominal perimeter, blood sample (potassium levels, with <3.5 mEq/L defined as hypokalemia) and blood pressure at baseline and at 1 month, 3 months, 6 months, and 12 months (with intervals of ± 10, ± 20, ± 30 and ± 60 days, respectively).
The scales used for weight and height measurement at each hospital were the Asimed S.A. (HGUGM), the SosPanduri (HC), Soehnle (HNJ), and the Vogel & Halke Hamburg Model 701 and SECA 220 (HSJD). Weight was recorded in kilograms and height in meters. With these measurements, the body mass index (BMI) was calculated: Weight in kg/height in meters squared (kg/m2). The BMI z score was also calculated using the standard Spanish tables (Sobradillo et al. 2004). This score was used to categorize the weight in the sample: Normal (percentile <85), or overweight (percentile ≥85) in accordance with the 2000 Centers for Disease Control (CDC) criteria (Kuczmarski and Flegal 2000).
An ECG was performed with the patient in the supine position at baseline and at the 3, 6, and 12 month follow-up visits. The ECGs used at the sites were Cardioline Delta Plus Version Base (HGUGM), Delta 1Plus Digital Electrocardiogram (HNJ), Siemens Scard 440 (HC), and Bio-Tek (Lionheart-1) (HSJD). The parameters obtained with the ECG were heart rate (beats per minute [BPM]), PR (ms), QRS (ms), and QTc (ms). The QTc was determined with Bazett's formula using a standard 12 lead ECG (25 mm/second and 1 mV). The QT was measured from the onset of the QRS complex to the end of the T wave, defined as the point of return of the T wave to the isoelectric line or to the nadir between the T and U waves in cases in which a U wave was present. In individuals with a broad QRS (≥ 120 ms), the JT interval was used (Lepeschkin and Surawicz 1952). All measurements were taken blind by two independent cardiologists who measured the QTc simultaneously, and the value used was the mean. The interobserver variability was <2%.
Not all authors are in agreement about the pathological levels of QTc in children and adolescents, as this varies depending upon both gender and age (Rautaharju et al. 1992). Whereas some studies consider QTc levels >450 ms to be pathological (Labellarte et al. 2003), others subdivide QTc levels based on gender, and consider a QTc interval >450 ms to be pathological for males, and values >470 ms to be pathological for females (de Castro et al. 2008; Margari et al. 2013). Others (Wilens et al. 1996; Blair et al. 2005; Correll et al. 2011) consider a QTc to be pathological when values are >440 ms, irrespective of gender. In this study, we also chose to consider a QTc interval >440 ms to be pathological for both males and females, in agreement with the latest literature in pediatric cardiology (Van Dorn et al. 2011).
Data analysis
Cardiac function was analyzed using the QTc and BPM variables of the entire sample, in all four mentioned periods of time. In order to prove the effect of the independent variables on these dependent variables over time, and to minimize the effect of those missing, a linear mixed model of repeated measures was used, with the patients as a random effect. All the subjects with at least one measure of QTc at any evaluation time were included in the analysis (Fig. 1). The QTc and BPM were introduced as dependent variables. The independent variables introduced were those sociodemographic, analytical, and clinical variables relevant to heart function according to the literature (Fraguas et al. 2008; Correll et al. 2011). In this case, the variables used were age, gender, potassium levels, weight (defined as BMI z score), total cumulative dose of AP (in chlorpromazine equivalents), presence/absence of antidepressant medication, and time (defined as months exposed to the treatment). For the statistical analysis, only visits at which an ECG was performed (baseline and 3, 6, and 12 month follow-up) were included.
The variable hypokalemia could not be included in the analysis, as there were no patients with potassium levels <3.5 mEq/L.
For the analysis of possible relations between patients with QTc >440 and the pertinent variables at each time, the Fisher Exact Test and the nonparametric Mann–Whitney U Test were used, depending upon the variables.
A second analysis was conducted to detect the variability of the dependent variables as a function of the type of AP drug administered. Three groups were created in the sample, based on the most commonly prescribed drugs (risperidone, quetiapine, and olanzapine). Patients were assigned to one of the three groups using the AP recorded at the month 1 visit. Subjects who required a change in AP were excluded from the analysis thereafter. To identify differences in the three groups, ANOVA and the χ2 test were used. Lastly, a second linear mixed model for repeated measures analysis was conducted. All subjects with any QTc measure at any time of evaluation were included in this analysis (Fig. 1). The covariables introduced in this analysis were only those that appeared to have an influence on the model in the first analysis (BMI, z score, antidepressants, gender), as well as age.
R free statistical software version 3.0.2 with the nlme and glmer packages was used to perform the calculations. All tests were two tailed and, in general, statistical tests with a p value <0.05 (significant α level of 5%) were considered significant.
Results
The clinical and demographic characteristics of the 216 subjects included in the study are shown in Table 1. All patients received an SGA. The number of patients evaluated at each visit was: Baseline n = 185, 3 months n = 138, 6 months n = 107, and 12 months n = 68 (Fig. 1).
Naïve patients were distributed among the three groups according to the antipsychotic treatment recorded at the first month measurement; 66 patients were switched to risperidone, 14 patients were switched to olanzapine and 17 patients were switched to quetiapine.
Differences among the three groups depending upon antipsychotic treatment.
Other races/ethnicities: African 1.2% (n = 3); Hispanic 6.5% (n = 14); Middle Eastern 2.3% (n = 5); Asian 0.9% (n = 2); Gypsy 0.9% (n = 2).
Include diagnosis of schizophrenia, schizoaffective disorders, brief psychosis, psychosis not otherwise specified.
Naïve patients who had not taken any antipsychotic treatment before the study.
Pimozide (n = 1) and chlorpromazine (n = 1).
Analysis performed: *χ2 and **ANOVA.
ADHD, attention-deficit/hyperactivity disorder; OCD, obsessive compulsive disorder; BMI, body mass index.
As shown in Table 1, the three treatment groups (risperidone, quetiapine, and olanzapine) were different with regard to age (p = 0.019), psychiatric diagnosis (p = 0.004), use of concomitant selective serotonin reuptake inhibitors (p < 0.0001), and presence of psychotic symptoms (p = 0.026) (Table 1).
QTc variations in the total sample
The average baseline QTc interval was 396.74 ms (SD = 29.99). The QTc values did not significantly vary throughout the study. No patient was excluded from the study because of a prolonged QTc. There were no QTc values >500 ms at any of the time assessments (Table 2).
Baseline follow-up = differences between baseline and follow-up; significance was assessed by means of mixed model.
bpm, Beats per minute.
There were no differences in baseline QTc interval between treatment-naïve and quasi-naïve patients (396.74 ± 30.45 vs. 396.54 ± 28.80, p = 0.999) or over time in the entire sample (p = 0.34).
With regard to gender, females presented a larger QTc interval at baseline than males (401.86 ± 33.61 ms vs. 392.65 ± 25.37 ms, p = 0.002), and although they continued to have a larger QTc interval during the study, the differences stopped being significant (p = 0.856).
We did not find a relationship between BMI and QTc values during the study (p = 0.13). When the sample was analyzed according to normal weight (BMI z score <85) or overweight (BMI z score ≥85), we observed that patients who were overweight at baseline had a lower QTc interval than normal weight patients (p = 0.022). However, QTc intervals of overweight patients increased more than normal BMI patients (p = 0.003).
There were no differences in QTc interval (ms) with regard to diagnosis at baseline (p = 0.334) or during the entire 12 month study (p = 0.150). Also, there was no difference based on presence or absence of psychosis at baseline (p = 0.674) or during the entire 12 months (p = 0.368). There were no differences in QTc during the 12 months based on use of tobacco (p = 0.617), alcohol (p = 0.800), or cannabis (p = 0.610).
There were no correlations found between age and QTc intervals at baseline (p = 0.074) or follow-up (p = 0.801).
There were no QTc changes found based on cumulative chlorpromazine-equivalent dose at the time of assessment (p = 0.66).
The patients who took antidepressants at baseline tended to have higher QTc values (p = 0.072). However, QTc decreased significantly over the study in those receiving concomitant antidepressants compared with those who did not (p = 0.039).
There were only nine patients (4.9%) with QTc >440 ms at baseline. At 3 months, nine patients (6.5%) presented a QTc >440 ms, at 6 months, six patients (5.7%) presented a QTc >440 ms, and at 12 months no patients presented a QTc >440 ms. When analyzing possible relations between QTc >440 ms and other pertinent variables at each time period, there were no significant differences with respect to QTc >440 ms and type of AP (baseline p = 0.24, 3 months p = 0.15, 6 months p = 1); cumulative dose of the drug at each time period (baseline p = 0.951, 3 months p = 1, 6 months p = 0.952); or antidepressant use (baseline p = 0.39, 3 months p = 0.22, 6 months p = 0.66). With respect to weight, only at the 6 month assessment was the BMI z score significantly lower in the group with QTc >440 ms (baseline p = 0.54, 3 months p = 0.92, 6 months p = 0.044), compared with patients with normal QTc measures.
Variations of the QTc comparing the three main AP drugs
There were no differences in QTc values at any time when comparing the three main AP drugs (risperidone, quetiapine, and olanzapine) (Table 3). When controlling for the possible effect of significant variables such as gender, age, antidepressant use, or weight, the difference among the three main AP drugs remained not significant (risperidone–olanzapine p = 0.578; risperidone–quetiapine p = 0.216; olanzapine–quetiapine p = 0.528). There were also no differences among the three AP based on total cumulative dose in chlorpromazine equivalents (risperidone p = 0.54, olanzapine p = 0.33, quetiapine p = 0.45).
Significance was assessed by means of mixed model.
BL, baseline; B-F, differences between baseline and follow-up; 3-m, 3 months; 6-m, 6 months; 1-y, 1 year; M, mean; SD, standard deviation; R-O, risperidone-olanzapine; R-Q, risperidone-quetiapine; O-Q, olanzapine-quetiapine; bpm, beats per minute.
Heart rate variations
The baseline heart rate (BPM) inversely correlated with age (p = 0.003), and it was higher in females than in males (p = 0.036). Heart rate tended to decrease with time, although it did not reach statistical significance (p = 0.054) (Table 2). There were no differences in presence of tachycardia (BPM >100) during follow-up (p = 0.93). With respect to differences in AP, patients on quetiapine had significantly increased heart rates compared with those on risperidone (p = 0.04); there was also a tendency toward decreasing BPM over time in the risperidone group (p = 0.051) (Table 3). However, there was no statistical difference among the three AP when controlling for cumulative chlorpromazine dose.
Discussion
In this large sample with antipsychotic-naïve or quasi-naïve children and adolescents treated mainly with SGA, QTc intervals and heart rate did not increase during the 1 year follow-up. BMI appears to be the only clinical variable affecting QTc values. Quetiapine increased heart rate more than risperidone.
In this sample, in keeping with other studies in pediatric populations (de Castro et al. 2008; Correll et al. 2011; Margari et al. 2013), we did not find variations in QTc in relation to AP use either at baseline or during the longitudinal 12 month period. Although there are also some studies suggesting that SGA may increase QTc in pediatric populations, this prolongation seems to be significant only for ziprasidone (Correll et al. 2006; Jensen et al. 2015).
Previous studies in pediatric populations have shown a correlation between obesity and QTc prolongation (Correll et al. 2011), which may be meaningful, as SGA significantly increase weight (Correll et al. 2009; De Hert et al. 2011; Fraguas et al. 2011). In our study, the results regarding the relation of BMI and QTc prolongation were not as conclusive. In our sample, contrary to what was expected, a lower baseline QTc interval was found in overweight patients, and lower BMI was observed in patients with prolonged QTc at 6 months assessment. Even though, it should be noted that, in overweight patients, QTc intervals increased over the 12 month period more than in the normal weight patients. For this reason and because of the known association between SGA and weight gain, longer follow-up studies should be conducted in pediatric populations to further evaluate this relationship.
Although the combination of AP with antidepressants induced a QTc increase in the adult population (Sala et al. 2005), this has not been confirmed in other studies with children (McIntyre and Jerrell 2008; Correll et al. 2011). The same occurred in our pediatric population in which patients receiving antidepressant treatment tended to have lower QTc interval measurements over the study. It should be noted that these decreased QTc values were not even close to values considered clinically significant (Anttonen et al. 2009; Shah 2010).
There are no conclusive results with regard to the possible influence of psychiatric diagnosis on QTc lengthening. There are studies that demonstrate a relationship between this increase and greater presence of schizophrenic spectrum disorders in pediatric samples (Correll et al. 2011). Moreover, recent studies have demonstrated ECG changes in adults with schizophrenia in comparison with healthy controls, even without the presence of AP treatment (Blom et al. 2014). In this study, there were no differences found when the sample was divided in two subgroups based on presence or absence of psychosis, in keeping with other studies in pediatric populations (de Castro et al. 2008).
It is important to emphasize that, even having selected less restrictive values for QTc changes (>440 ms) (Van Dorn et al. 2011), only a small proportion of patients (4.9%) presented values >440 ms at baseline, and it remained stable as the study progressed. Further, it is important to highlight that the increased QTc values did not relate to any of the three evaluated SGA, there were no cases in which QTc intervals were >500 ms, and no patients were discontinued on the basis of prolonged QTc.
Studies demonstrate different effects on QTc prolongation by different AP, in both adult (Buckley and Sanders 2000) and pediatric populations (Labellarte et al. 2003). Several studies have involved typical AP such as thioridazine (Hartigan-Go et al. 1996; Glassman and Bigger 2001), pimozide (Fulop et al. 1987; Flockhart et al. 2000), or droperidol (Reilly et al. 2000), with a larger increase in QTc. These data could not be evaluated in this study in which only two patients received treatment with pimozide, without finding any abnormal QTc values, and there was no prescription of any other typical AP in this group. With regard to atypical drugs, it is worth mentioning ziprasidone, with some studies in adult (Keck et al. 2001) and pediatric (Blair et al. 2005; Jensen et al. 2015) populations reporting QTc prolongation; however, in the pediatric population, these results are questionable (Loebel et al. 2006). Another study (Correll et al. 2011) suggested a potentially low arrhythmogenic effect in adolescents with a normal baseline ECG receiving this medication. In our sample, the bulk of the subjects (99.1%) were taking atypical AP. The three main prescribed AP were analyzed individually (risperidone, quetiapine, and olanzapine), and no differences were found among them in terms of influence on QTc.
As expected (Rautaharju et al. 1992; Shin et al. 2005), females in our sample also showed greater QTc prolongation during the baseline period than did males. However, as in other pediatric studies (de Castro et al. 2008), gender did not result in a variable that could increase QTc during the time when those patients are in treatment with SGA.
There have been several studies reporting increased heart rate in children and adolescents as a side effect of AP use (McIntyre and Jerrell 2008), but others have not found similar changes (Findling et al. 2000, Buitelaar et al. 2001; Findling et al. 2009; Haas et al. 2009). This effect has been emphasized especially with clozapine (Midbari et al. 2013), but also with risperidone (McCracken et al. 2002; Masi et al. 2003; Shea et al. 2004), olanzapine (Tohen et al. 2007), quetiapine (DelBello et al. 2009), and ziprasidone (Blair et al. 2005). This study was unable to evaluate the effect of clozapine on heart rate because of the limited number of patients involved. Regarding SGA, we found that quetiapine showed a greater increase in heart rate than risperidone. The declining BPM during the 12 month period in the whole sample may be explained by the age of the patients, more important in those treated with risperidone, who were significantly younger.
Finally, it must be emphasized that this study had a 12 month longitudinal design with treatment-naïve or quasi-naïve patients. The fact that this is a naturalistic study in both inpatient and outpatient children and adolescents allows its results to be generalized to different treatment settings.
Limitations
First, the naturalistic, nonrandomized design of the study and the risk of selection and attrition bias were limitations of our study. It should also be pointed out that there was important loss of patients to follow-up during the study, which led us to use mixed models in the statistical analysis in order to limit its impact. The limited use of certain AP with a higher risk of cardiovascular side effects, such as ziprasidone, clozapine, and FGA, do not allow us to draw conclusions regarding these AP. It was not possible to measure the effects of aripiprazole, as it was just beginning to be marketed in our country at the time the study was conducted. The study permitted the use of concomitant medications. Given that antidepressants can increase QTc, they were included in the mixed model. The limited number of patients on other drugs precluded us from assessing the potential effects of those drugs on the QTc interval.
Conclusions
The SGA evaluated in this study (risperidone, olanzapine, and quetiapine) appear to be safe in the child and adolescent population, with regard to QTc and heart rate. This is backed up in this study by the fact that there were no major arrhythmias reported. The fact that there was no QTc prolongation during the time period, regardless of the AP used and the unrelated cumulative chlorpromazine dose, would appear to reinforce their safety in the pediatric population. The study also questions the influence of factors such as gender and concomitant use of antidepressants on increased QTc interval in the pediatric population receiving AP, and only overweight appears to be related to QTc prolongation. Among the three SGA evaluated, only quetiapine showed a major effect on increasing heart rate in our pediatric population.
Clinical Significance
This study broadens our knowledge regarding the cardiac safety of AP use in the child and adolescent population. This study demonstrates that AP appear to be safe from the point of view of electrocardiographic side effects in the pediatric population, in keeping with a recent meta-analysis (Jensen et al. 2015), as our sample does not present QTc prolongation or increased heart rate. It did not support the validity of some clinical and demographic variables suggested in previous studies to define the population most at risk. Determining in which cases a routine ECG is indicated remains a controversial subject. Several studies suggest the feasibility of performing routine ECGs in children and adolescents receiving AP treatment (Labellarte et al. 2003; Masi and Liboni 2011), whereas others question the routine procedure in all patients when the prevalence of QTc changes is low, and advocate restricting it only to patients considered high risk (Correll et al. 2011), as it is done in patients with attention- deficit/hyperactivity disorder (ADHD) treated with methylphenidate (Perrin et al. 2008; Cooper et al. 2011). Our data would support restricting routine ECG at follow-up in patients taking the three study SGA to the population at risk (e.g., with clinical risk factors or congenital and family history of heart disease) (Jensen et al. 2015) as well as considering it in patients in whom weight gain is observed.
Footnotes
Acknowledgment
We thank the Centre of Biomedical Research in the Mental Health Network (CIBERSAM), Madrid (Spain).
Disclosures
Dr. Alda has been a consultant to or has received honoraria or grants from Agència d'Informació, the Alicia Koplowitz Foundation, Avaluació i Qualitat en Salut (AIAQS), Eli Lilly, Instituto de Salud Carlos III, Janssen Cilag, Rovi, Shire, and the Spanish Ministry of Health. Dr. Muñoz-Samons has received grants from Instituto de Salud Carlos III and has received support from Otsuka for attending some conferences. Drs. Tor, Merchán-Naranjo, and Tapia have no conflict of interest. Dr. Baeza has received grants from CIBERSAM, Fundación Alicia Koplowitz, and Instituto de Salud Carlos III, and has received honoraria as a speaker for Janssen, as well as support from Otsuka for attending some conferences. Dr. Calvo-Escalona has received grants from Fundació La Marató-TV3, Fundación Alicia Koplowitz, and Instituto de Salud Carlos III, and travel support to attend scientific meetings from Janssen, Otsuka, and Shire. Dr. Castro-Fornieles has received grants from Fundació TV3, Fundación Alicia Koplowitz, Generalitat de Catalunya, and Instituto de Salud Carlos III. Drs. Martínez Cantarero, Andrés Nestares, and Fernández-Avilés have no conflict of interest. Dr. Arango has been a consultant to or has received honoraria or grants from Abbott, Amgen, AstraZeneca, Bristol-Myers Squibb, Caja Navarra, CIBERSAM, Fundación Alicia Koplowitz, Instituto de Salud Carlos III, Janssen Cilag, Lundbeck, Merck, Ministerio de Ciencia e Innovación, Ministerio de Economía y Competitividad, Ministerio de Sanidad, Mutua Madrileña, Otsuka, Pfizer, Roche, Servier, Shire, Schering Plough, and Takeda.