
Abstract
To The Editor:
A
Case Report
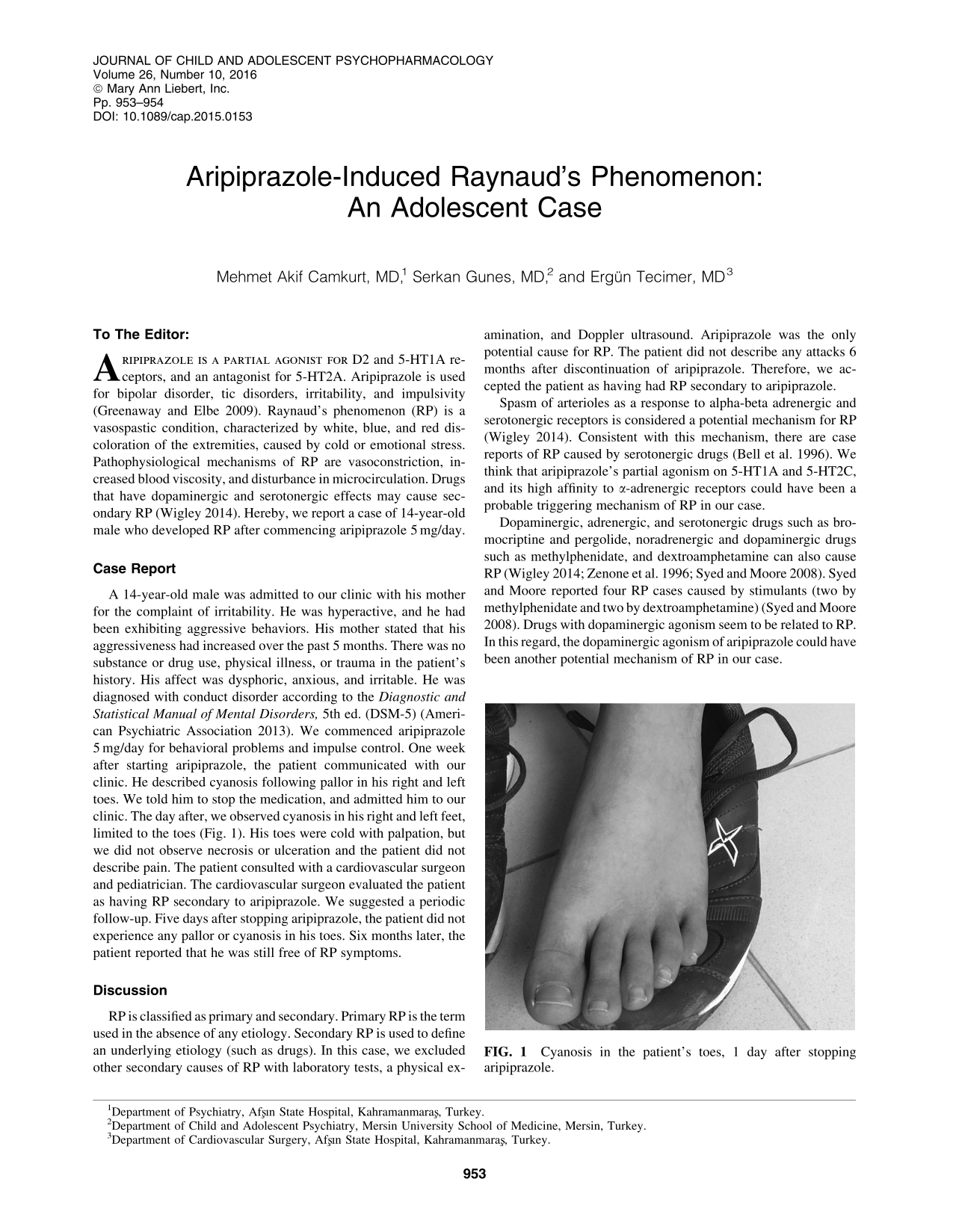
A 14-year-old male was admitted to our clinic with his mother for the complaint of irritability. He was hyperactive, and he had been exhibiting aggressive behaviors. His mother stated that his aggressiveness had increased over the past 5 months. There was no substance or drug use, physical illness, or trauma in the patient's history. His affect was dysphoric, anxious, and irritable. He was diagnosed with conduct disorder according to the Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5) (American Psychiatric Association 2013). We commenced aripiprazole 5 mg/day for behavioral problems and impulse control. One week after starting aripiprazole, the patient communicated with our clinic. He described cyanosis following pallor in his right and left toes. We told him to stop the medication, and admitted him to our clinic. The day after, we observed cyanosis in his right and left feet, limited to the toes (Fig. 1). His toes were cold with palpation, but we did not observe necrosis or ulceration and the patient did not describe pain. The patient consulted with a cardiovascular surgeon and pediatrician. The cardiovascular surgeon evaluated the patient as having RP secondary to aripiprazole. We suggested a periodic follow-up. Five days after stopping aripiprazole, the patient did not experience any pallor or cyanosis in his toes. Six months later, the patient reported that he was still free of RP symptoms.

Cyanosis in the patient's toes, 1 day after stopping aripiprazole.
Discussion
RP is classified as primary and secondary. Primary RP is the term used in the absence of any etiology. Secondary RP is used to define an underlying etiology (such as drugs). In this case, we excluded other secondary causes of RP with laboratory tests, a physical examination, and Doppler ultrasound. Aripiprazole was the only potential cause for RP. The patient did not describe any attacks 6 months after discontinuation of aripiprazole. Therefore, we accepted the patient as having had RP secondary to aripiprazole.
Spasm of arterioles as a response to alpha-beta adrenergic and serotonergic receptors is considered a potential mechanism for RP (Wigley 2014). Consistent with this mechanism, there are case reports of RP caused by serotonergic drugs (Bell et al. 1996). We think that aripiprazole's partial agonism on 5-HT1A and 5-HT2C, and its high affinity to α-adrenergic receptors could have been a probable triggering mechanism of RP in our case.
Dopaminergic, adrenergic, and serotonergic drugs such as bromocriptine and pergolide, noradrenergic and dopaminergic drugs such as methylphenidate, and dextroamphetamine can also cause RP (Wigley 2014; Zenone et al. 1996; Syed and Moore 2008). Syed and Moore reported four RP cases caused by stimulants (two by methylphenidate and two by dextroamphetamine) (Syed and Moore 2008). Drugs with dopaminergic agonism seem to be related to RP. In this regard, the dopaminergic agonism of aripiprazole could have been another potential mechanism of RP in our case.
Clinicians should keep in mind that aripiprazole could cause peripheral vascular side effects.
Footnotes
Disclosures
No competing financial interests exist.