
Abstract
Objective:
The purpose of this study was to examine long-term outcomes of nonpharmacological intervention in children and adolescents with stroke utilizing repetitive transcranial magnetic stimulation (rTMS) to the primary motor cortex combined with constraint- induced movement therapy (CIMT) to improve motor function in the paretic hand. Outcome measures included function, satisfaction, and medical status review.
Methods:
Fourteen of the original 19 participants (74%) from our rTMS/CIMT clinical trial (real rTMS+CIMT, n = 8; and sham rTMS+CIMT, n = 6) were evaluated. The median age of the subjects at follow up was 13.4 years (range 11–20 years old, 50% male). Median time to follow-up was 47.5 months (range 21–57 months). Descriptive statistics were conducted using frequencies and counts. Motor performance was measured using the Assisting Hand Assessment (AHA) and Canadian Occupational Performance Measure (COPM). Satisfaction was reported with use of the COPM and TMS Tolerance Survey. Open-ended interview was conducted for feedback on study experience and subjective perspectives of current functional status.
Results:
Overall, seven of eight individuals who received real rTMS and five of six individuals who received sham rTMS maintained or improved AHA scores. Six of 14 participants reported new onset of co-occurring conditions (four individuals in the real rTMS group, two individuals in the sham rTMS group). The majority (86%) of participants reported study satisfaction. Review of medical status revealed co-occurring conditions including: Epilepsy, obsessive-compulsive disorder, anxiety, depression, unspecified mood disorder, and undiagnosed inattentiveness.
Conclusions:
Long-term outcomes of rTMS/CIMT in pediatric stroke were investigated. Variability in performance and unattributed symptoms were noted. Considering the prevalence of co-occurring conditions in children and adolescents with stroke, new-onset symptoms were not attributed to original intervention. With the small sample size, the impact of rTMS on long-term outcomes cannot be fully determined from these data. Characterizing long-term outcomes through performance, participant perspectives, and medical status allows comprehensive assessment of rTMS/CIMT intervention efficacy.
Introduction
N
Long-term safety and efficacy is evident in CIMT (Olesch et al. 2010; Eliasson and Holmefur 2015). Safety of CIMT in children is measured by monitoring for functional decline in the restrained limb and parental stress (Cope et al. 2008; Fedrizzi et al. 2013). The strong evidence in pediatric CIMT has guided the translation of research outcomes to the clinical setting (Reidy et al. 2012).
Safety in neuromodulation studies has been measured through lack of declining performance and reports of both serious (seizure) and minor (e.g., headache, tingling at the site of stimulation) adverse events (Gillick et al., 2014a, 2015; Krishnan et al. 2015). Short-term safety outcomes reflect risks within session or between sessions across the study time frame with Gillick et al. (2015) reporting preliminary short-term safety evidence following a 10 day trial of repetitive transcranial magnetic stimulation (rTMS) combined with CIMT (Gillick et al. 2014a). Long-term safety outcomes reflect potential risks over time following the conclusion of the study.
Long-term neuromodulation safety for children with medication-resistant depression treated with rTMS was examined with a 3 year follow-up, revealing no decline in cognitive function or depressive symptoms in a small sample (n = 6) (Mayer et al. 2012). Gillick et al. (2014a) and Mayer et al. (2012) reported no serious adverse events following rTMS in children. However, long-term outcomes have not yet been reported on studies combining NIBS with motor interventions in children with hemiparesis.
Measuring long-term outcomes in pediatric populations is challenging, given indirect and direct influences. Results are often not clearly traceable to the original intervention because of maturation in the pediatric population. Biological development is compounded by co-occurring conditions that may develop as a child ages, such as seizures, executive dysfunction, inattentiveness, mental health issues (Depositario-Cabacar and Zelleke 2010; Bjorgaas et al. 2012; Weierink et al. 2013). Socioenvironmental determinants further amplify overall health, positively or negatively (Spencer and Strazdins 2015). The confluence of indirect factors can greatly impact a child's responsivity to direct therapeutic interventions aimed at improving daily functioning over a lifetime.
Despite the challenges of long-term reporting, novel interventions directly designed to impact brain function such as combining NIBS with motor interventions warrant comprehensive long-term follow-up studies. The purpose of this study is to report long-term outcomes on our original clinical trial of rTMS/CIMT in pediatric hemiparesis targeting improved upper limb function for daily activities and participation. Developmental outcomes were examined through behavioral testing, satisfaction measures, child/caregiver interviews, and medical status review. We hypothesized that there would be no differences between groups in the reports of new onset symptoms following original study participation.
Methods
Original intervention
Original study inclusion involved multiple criteria for children and adolescents 8–17 years of age with hemiparesis secondary to stroke or periventricular leukomalacia, minimal paretic hand movement, and the presence of a motor evoked potential (MEP) in the ipsilesional hemisphere using single-pulse TMS (Gillick et al. 2014b). Original exclusion criteria involved co-occurring diagnoses (recent seizure activity, vision, or communication deficits), spasticity injections within 6 months of enrollment, a lack of MEP, contraindications for neuroimaging or NIBS, or concurrent rehabilitation programming. Children on centrally acting medications for attention-deficit/hyperactivity disorder and seizures were excluded (e.g. Adderall, Keppra) given this was one of the first pediatric studies involving synergistic use of NIBS with CIMT. The original study design involved pre- and posttrial testing with 100% enrolled participant study completion. Methodology, behavioral, and short-term safety results were previously reported (Gillick et al. 2014a,b).
In brief, participants were assigned to real rTMS plus CIMT (n = 10) or sham rTMS plus CIMT (n = 9) (Gillick et al. 2014b). The rTMS intervention consisted of high-frequency 6 Hz priming followed by low-frequency 1 Hz rTMS to the contralesional primary motor cortex. A 70 mm figure-of-eight coil or sham coil with a Magstim 200 Stimulator was used for the rTMS intervention (Magstim Company Ltd, Dyfed, UK). Ten hours of CIMT was provided in a 1:1 goal-directed context by occupational therapists with formal training (UAB Civitan Sparks Neuromotor Training Program, Birmingham, AL). A high intensity restraint-wearing schedule and a daily home program were utilized.
Long-term follow-up study participants
All original participants were invited for the long-term follow-up study via an Institutional Review Board (IRB)-approved phone call. Fourteen of the original 19 participants (74%) responded to the invitation and completed the follow-up study. Of the five who did not participate, two declined and three did not respond (following three attempts). The majority of participants completed the study in the laboratory (71%). Four participants (28%) were seen in their homes because of transportation limitations. The Consolidated Standards of Reporting Trials (CONSORT) diagram illustrates initial randomization of groups in the original study and those who returned for long-term follow-up (Fig. 1). Approval was obtained from the IRB at the University of Minnesota and Gillette Children's Specialty Healthcare. Signed consent/assent forms were obtained from all parents/legal guardians and participants.
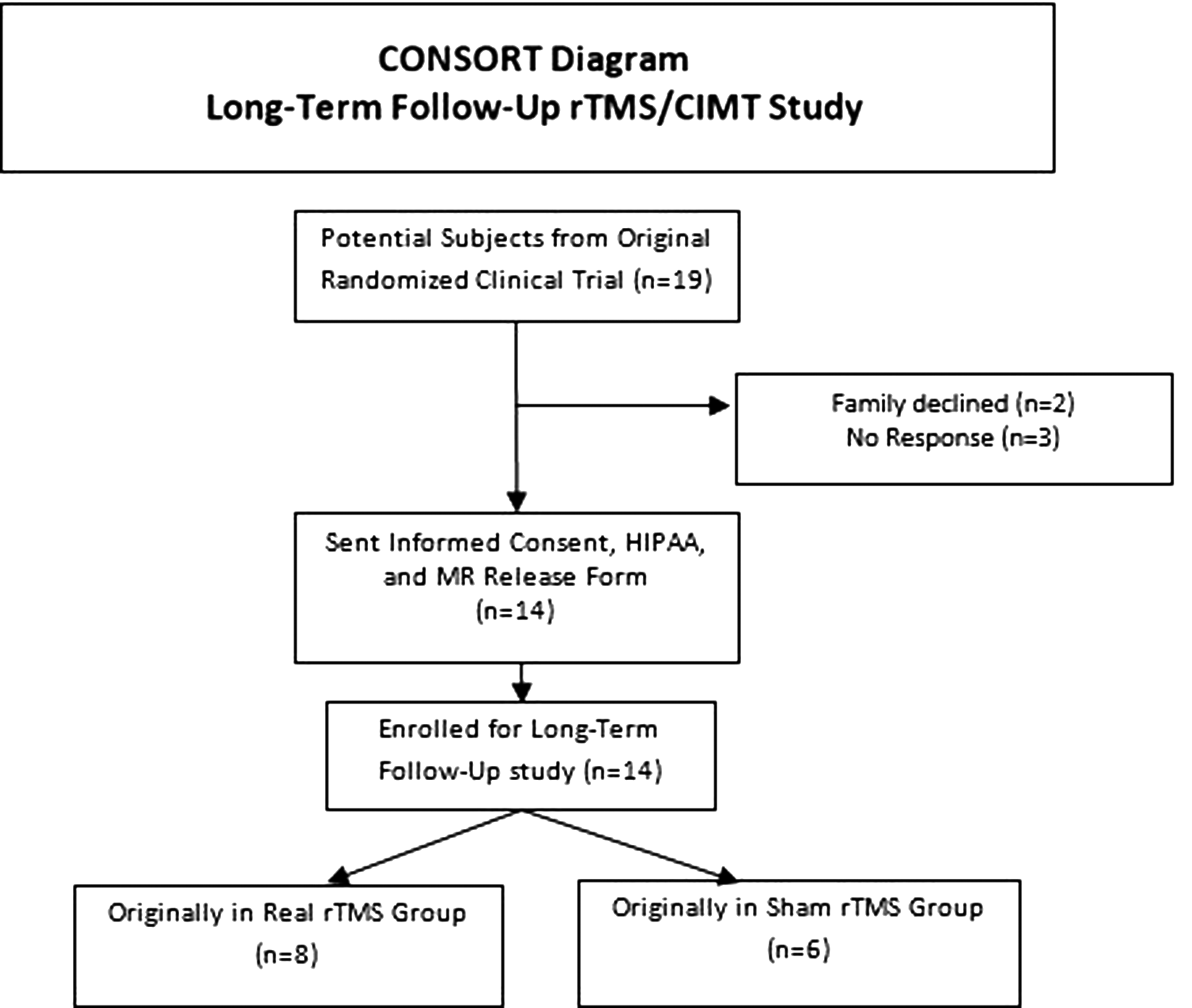
CONSORT flow diagram delineating follow-up and original group assignment. CONSORT, Consolidated Standards of Reporting Trials; rTMS, repetitive transcranial magnetic stimulation; CIMT, constraint-induced movement therapy; HIPAA, Health Insurance Portability and Accountability Act; MR, medical record.
The original study design was a staggered start with individual enrollment, which influenced the long-term follow-up timing. The median follow-up was 47.5 months post rTMS/CIMT study participation (range 21–57 months). Time since study participation is illustrated in Figure 2. Group demographics and reported interventions since study participation are displayed in Table 1. Recall was facilitated by completing the majority of sessions in the original intervention environment, verbally reorienting the participant to the intervention structure, and use of pictures of previous study staff. Outcome measures (performance, satisfaction, functional status, and safety measures) were repeated from the original trial for comparison (Gillick et al. 2014b).
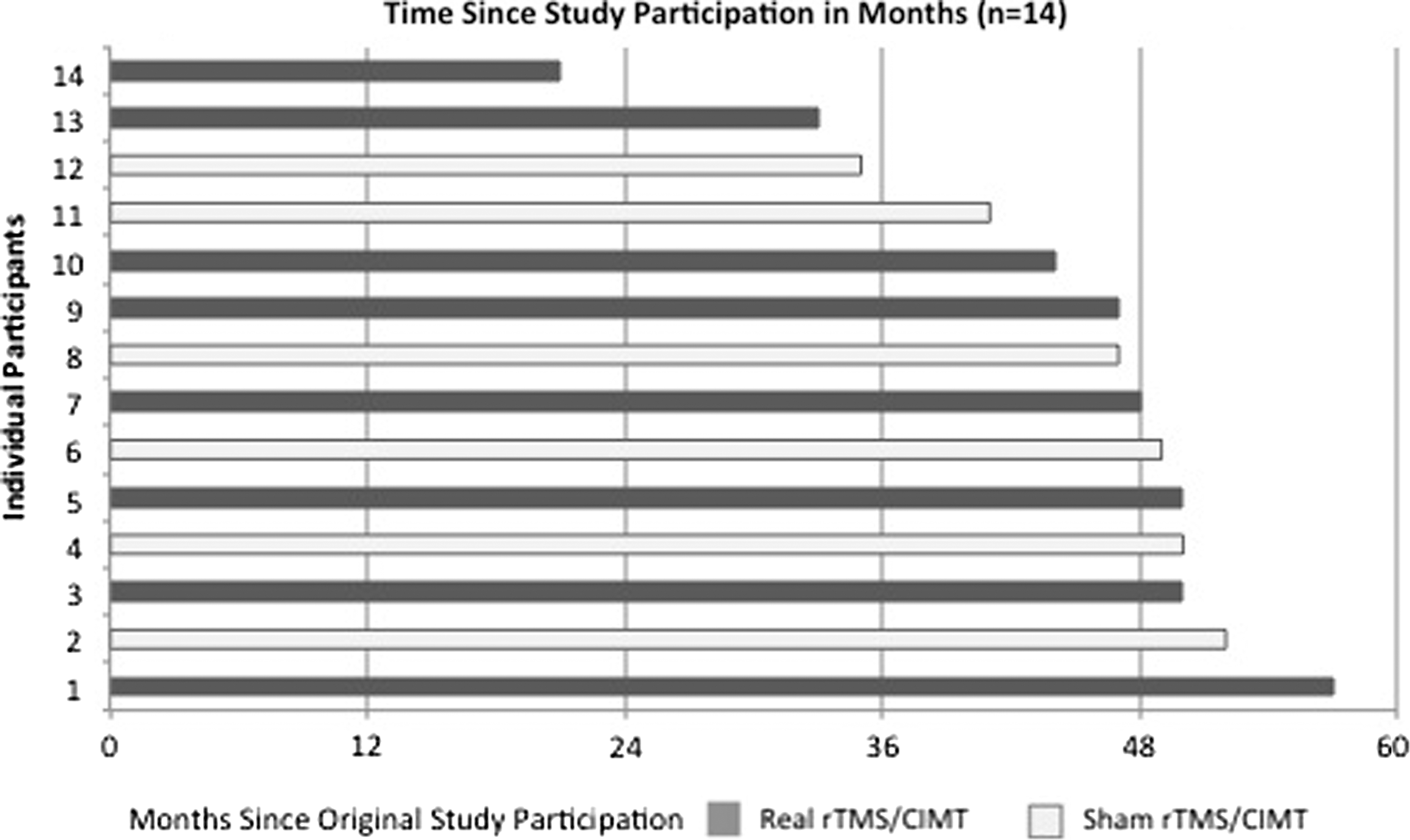
Time since study participation in months. Solid bars represent each individual in the real rTMS/CIMT group; open bars represent each individual in the sham rTMS/CIMT group. rTMS+CIMT, repetitive transcranial magnetic stimulation and constraint-induced movement therapy.
Numbers in parentheses after frequency counts are group percentages for categorical variables.
rTMS+CIMT, repetitive transcranial magnetic stimulation and constraint induced movement therapy; MACS, Manual Ability Classification System; UE, upper extremity.
Motor performance outcomes were evaluated using the Assisting Hand Assessment (AHA) (version 4.4). The AHA is a bimanual motor performance measure of spontaneous hand use during a structured play or functional activity. Reliability and validity of the AHA has been demonstrated for children up to 12 years of age (Krumlinde-Sundholm et al. 2007). The same version of the AHA (school age child vs. adolescent) was used as the original trial in the current study, as score consistency and interpretation when children transition between versions has not yet been demonstrated. Raw AHA scores were converted to the 0-100 logit-based AHA units (Krumlinde-Sundholm 2012). AHA scores are presented individually over time.
Participant-reported outcomes used the Canadian Occupational Performance Measure (COPM) and TMS Tolerance Survey (adapted from Garvey et al. [2001]) to examine functional status and participant satisfaction. The COPM is a structured 10 point Likert rating scale to measure self-perception of current performance and satisfaction related to goals in the original trial (Galvin et al. 2010). Open-ended interview questions were coded by theme and supplemented numerical scales.
Functional status and safety was examined through use of the TMS Subject Report of Symptoms Questionnaire guided interview questions to investigate potential adverse events that may have occurred since participation in the original trial (Garvey et al. 2001). All caregivers interviewed were parents and legal guardians of participants. Medical records were reviewed (when added consent from legal caregivers was provided) if a new onset-diagnosis was reported.
Statistical analysis
Given the sample size, descriptive statistics were used to characterize the real and sham groups. Comparisons were made using frequency counts to quantify upper extremity specific interventions since the original trial participation, because they can impact current functional status (spasticity management, therapy, or surgery). Because of the time delay in follow-up testing and influence of maturation on hand skill development, between-group differences were not assessed.
Results
Medical interventions for upper extremity function (e.g. surgery, spasticity injections) occurring after participation in the trial were reported at a higher frequency for the sham rTMS group than for the real rTMS group (Table 1). Table 1 reflects between- group differences in medical interventions that were congruent with baseline differences (Manual Abilities Classification System [MACS] levels, motor performance on the AHA) previously reported in the original trial (Gillick et al. 2014b).
Motor performance of each individual on the AHA is displayed by group (Fig. 3). Across both groups, 86% maintained or improved scores on the AHA (seven of eight individuals received real rTMS and five of six individuals received sham rTMS. Improvement on AHA and COPM (performance and satisfaction) behavioral measures was noted in 50% of participants from both groups (real rTMS group n = 4, sham rTMS group n = 3).
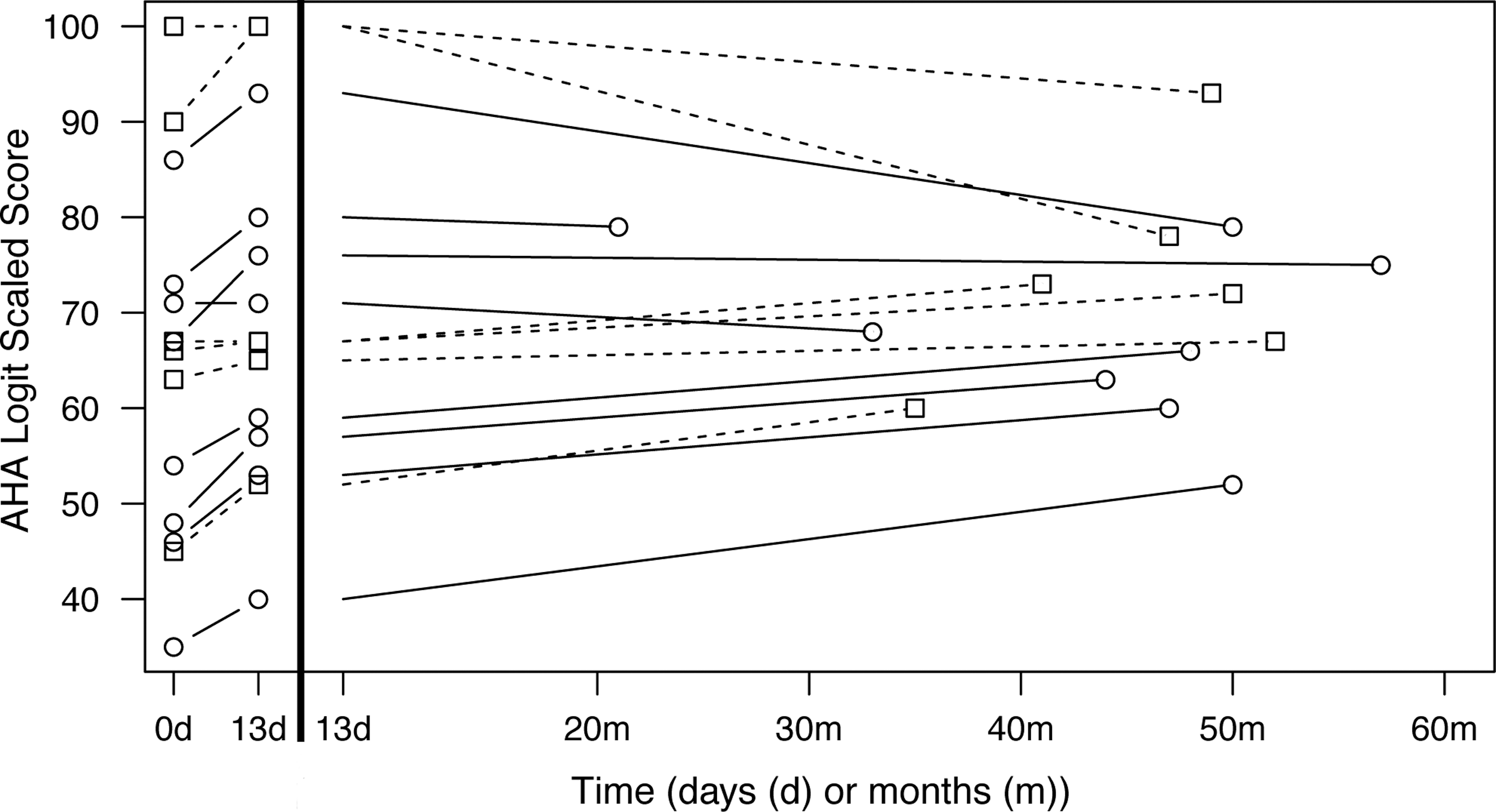
Change in bimanual performance at three testing points (pretrial, posttrial, and long-term follow up) using the Assisting Hand Assessment (AHA) and logit-based 0-100 AHA-units. Solid lines with circles denoting testing points represent individuals in the real rTMS+CIMT group (n = 8) and dashed lines with squares denoting testing points represent individuals in the sham rTMS+CIMT group (n = 6). Time in days (d) or months (m) at each testing point is reflected with pretrial = 0d, posttrial = 13d, and long-term follow-up as indicated by month (range 21–57 months). CIMT, constraint-induced movement therapy; rTMS, repetitive transcranial magnetic stimulation.
Interrater reliability of ± 3 raw points has been determined on the AHA (Holmefur et al. 2007). In this sample, scores outside of that range were considered to reflect real change. The median score at follow-up on the AHA was 68 logit-based AHA units (range 52–93). Two individuals demonstrated decreased logit scores (one individual in thereal rTMS group [100 to 78] and one individual in the sham rTMS group [93 to 79]). Neither of the individuals with decreased AHA scores reported adverse events during the open interview or demonstrated decreases on the COPM. One of the individuals with the decreased scores reported onset of an unspecified mental health condition.
Original COPM ratings were reviewed with the participants and caregivers prior to conducting the current rating. In the event that the participant was not the original rater, both participant and previous proxy ratings were elicited. Of the COPM goals originally reported across intervention groups, 95% were bimanual. Five of 13 individuals reported that the goal areas were no longer relevant (e.g., previous typing goals not applicable given one-handed use of tablets, or the person's leisure interests had changed). An increase in satisfaction with present level of performance was noted despite no reported gain in actual performance, as several participants reflected that goal areas had been reprioritized in their lives.
A TMS Tolerance Survey revealed that 12 of 14 (86%) participants were willing to participate in a clinical trial again and would recommend rTMS intervention to others. One participant reported a “maybe” and one participant reported a “no” for participating again. Eleven of 14 (78%) participants recalled the sensation of the rTMS intervention using words such as “tapping,” “clicking,” or “weird” to describe the sensation of the TMS coil discharging. All caregivers (100%) reported they would recommend rTMS intervention to others.
Family-centered, developmentally appropriate questions incorporated open-ended feedback. Recall deficits were identified in several participants with varying times since trial participation. One participant with the shortest time since participating (21 months) reported limited to no recollection of the trial.
Caregivers and participants reported multiple themes related to self-awareness, study retention, and challenges associated with the cast. The first theme centered on self- awareness of their disability in peer settings outside the trial given the non-removable cast placed on the less-affected upper extremity for the 13 day duration. Several adolescents and caregivers attributed success with peer support outside the trial to early self-advocacy and education of peers at young ages. Immediate and extended family support was most frequently cited, as well as pediatric trial personnel support. Individual perspectives on the cast-wearing schedule varied with reports of significant impacts on both academic and daily living. Samples of individual responses are reported in the Appendix.
Report of co-occurring conditions
Medical records verified that 2 of 14 participants (both real rTMS group) reported seizures after participation in the original trial, with subsequent medication management. One participant originally participated at age 8 and seizures commenced ∼6 months later. The participant's caregiver had orally reported a seizure at 18 months during the original rTMS/CIMT recruitment but this was not reflected in the medical record. The second participant participated at age 8 and seizures commenced 55 months later. This participant had no history of seizures. Five of the 14 participants reported new onset of medical treatment for mental health issues following trial participation, including depression, anxiety, obsessive-compulsive disorder, and undiagnosed inattentiveness (three individuals in the real rTMS group, two individuals in the sham rTMS group). All diagnosed mental health issues were managed with medication per caregiver report. The onset of co-occurring conditions ranged from 6 to 55 months (median: 47.5 months) following original trial participation.
Discussion
Achievement differences were noted in all measures regardless of intervention group. One rater, blinded to original group assignment, completed all AHA scorings. Variable performance noted on the AHA is inconsistent with long-term AHA reports of scores remaining stable or improving (Eliasson and Holmefur 2015) Subjectively, the two individuals with decreased AHA scores demonstrated a high level of efficiency and speed in their use of compensatory movements. Selective use of the more affected hand during performance-based testing may reveal increased self-awareness of hand limitations and prioritized use for testing. A potential decrease in AHA performance has been noted subjectively during periods of gross motor skill development, growth spurts, and transition periods with peers (i.e., entrance to middle school or high school).
In order to compare to original measures, the AHA was selected despite several participants exceeding the age limits. Not all participants who demonstrated decreased scores on the AHA reported a change in medical status or the COPM. Reliable, long-term measures that transcend school ages to young adulthood are critically needed. A performance-based measure that reflects time/efficiency, an individual's satisfaction, and self-efficacy may provide insight on the shifting priorities of adolescent populations for the development of future interventions. Tool development focusing on stability of behavioral testing measures and reliability as the child develops is indicated for an understanding of the long-term impact of our interventions.
Long-term use of the COPM over time in children is reported in pediatric hemiplegia intervention studies (Olesch et al. 2010). This tool provides a measure of the individuals' perception of their performance and associated satisfaction level. Although the COPM goals were often no longer salient, the use of the COPM at follow-up provided a deeper understanding of how some children prioritize goals related to daily functioning. The appropriate reassessment interval for a child has not been determined. Even participants who were reassessed at the shortest intervals reported goals that were no longer relevant in their lives. Child-rated reassessment using this tool beyond 6–9 months does not appear to be valid given the amount of development and social awareness that occurs with maturation. The addition of systematically measuring whether the achievement of goals was within the time frame desired would provide additional depth of knowledge to the interpretation of goal attainment.
Open-ended interviewing regarding safety and satisfaction complemented performance-based testing to explore satisfaction with the participant and family's experience in this 2 week study. The participants provided varying input related to trial design and recommendations for preparing participants of future NIBS studies (see Appendix). Recommendations included strategies to alleviate anticipatory anxiety through preparation and child-friendly communication. Further, participants suggested providing guidance for peer interactions, given the vulnerability of being required to use the more affected hand for all hand function in the case of having a full-time cast for CIMT. Future studies may benefit from incorporating psychological support to aid in preparing for peer interactions outside of trial participation. Several caregivers reflected feelings of stress in not knowing if their child was receiving the real rTMS intervention. Caregivers noted that clear communication prior to enrollment helped to alleviate trial participation anxiety.
Safety was assessed through the self-reporting of symptoms, updated medical record, and physician review. In this sample of 14 subjects (real rTMS, n = 8; sham rTMS, n = 6), there is preliminary long-term safety evidence. Six participants (43%) reported the onset of co-occurring conditions (both diagnosed and those not resulting in a formal diagnosis) following participation in the original intervention. Children with cerebral palsy are at higher risk of developmental or intellectual disability and epilepsy than same-age peers (Blackman and Conaway 2014). Berg et al. recently reported complete remission of seizures in only 26.6% of children with epilepsy who have a relevant abnormality noted on neuroimaging in a large sample 21 year longitudinal study (Berg et al. 2014). Given the risks of co-occurring conditions and seizure development as the child ages, a medical monitor independent of the original trial physician investigators reviewed each case and did not attribute symptoms to rTMS intervention. The real rTMS group also exhibited greater impairments impacting function at baseline, which may indicate a greater level of neurological involvement. Further investigation of rTMS safety with larger sample sizes is warranted. To effectively pool safety data across clinical trials, uniform safety measures will be essential.
Studies with larger participant numbers are needed, as this study describes a small sample, thus limiting the generalizability of the findings. The original trial did not include an a priori long-term follow-up analysis. Because of our significant findings reflecting short-term safety, feasibility, and improved motor outcomes, long-term safety was investigated. Consequently, the length of time to follow-up was impacted by this additional recruitment, limiting a uniform follow-up testing time frame. Because of the wide range of long-term follow up, recall bias may have influenced participant-reported measures and interviews. Future long-term studies should consider pairing neuromodulatory or cortical excitability testing and neuroimaging with follow-up behavioral testing to provide investigation into sustained neuroplastic changes over time.
Conclusions
This study investigated long-term outcomes for the combined intervention of rTMS/CIMT in children with hemiparesis. Behavioral outcomes exhibited variability in gains across ages. Of the outcome measures, the AHA revealed the greatest improvement. Overall satisfaction levels were high for both participants and caregivers. No report of symptom was attributed to the intervention in the original trial. Sample size and time to long-term follow-up variability limit conclusions on the impact of rTMS on long-term outcomes from these data. Further long-term investigation of safety, performance, and satisfaction in pediatric NIBS trials is warranted, with potentially pooling uniform safety measure data across clinical trials to increase pediatric diagnostic-specific sample sizes.
Clinical Significance
The priorities in these early phases of investigating synergistic neuromodulatory and rehabilitation interventions include evaluating the efficacy, perceived benefits by the caregivers and child participants, and study safety. Long-term safety with the pairing of neuromodulation and pediatric therapy techniques is supported in a small clinical trial. After completion of this study, we found that the satisfaction and participant-reported outcomes provided a critical lens to interpret outcomes that would benefit future studies. Combined analysis (safety, cortical excitability, performance, and participant perceptions) strengthens the validity and potential clinical translation of neuromodulation interventions.
Footnotes
Acknowledgments
We thank Jan Keprios for the scoring of participant videos. We are grateful for the children and families who participated in this study.
Disclosures
No competing financial interests exist.
Appendix
Open-ended questions were constructed using a storytelling structure to elicit greater detail (e.g. “Tell me about a time during the study that you liked”). Children were interviewed at the conclusion of the behavioral testing to aid in familiarizing the children with the previous study procedures. All children were interviewed first and caregiver interviews followed. This appendix includes a sample of child and caregiver responses.