
Abstract
Objective:
Children with autism spectrum disorder (ASD) have been reported to have reduced ability to methylate DNA and elevated markers of oxidative stress. We sought to determine if methyl B12, a key metabolic cofactor for cellular methylation reactions and antioxidant defense, could improve symptoms of ASD.
Methods:
A total of 57 children with ASD were randomly assigned to 8 weeks of treatment with methyl B12 (75 μg/kg) or saline placebo every 3 days in a subcutaneous injection. The primary outcome measure was overall improvement in symptoms of ASD as measured by the Clinical Global Impressions-Improvement (CGI-I) score. Secondary outcome measures included changes in the Aberrant Behavior Checklist (ABC) and the Social Responsiveness Scale (SRS). Laboratory measures of methionine methylation and antioxidant glutathione metabolism were assessed at baseline and 8 weeks.
Results:
A total of 50 children (mean age 5.3 years, 79% male) completed the study. The primary outcome measure – the clinician rated CGI-I score – was statistically significantly better (lower) in the methyl B12 group (2.4) than in the placebo group (3.1) (0.7 greater improvement in the methyl B12 group, 95% CI 1.2–0.2, p = 0.005). Clinical improvement among children treated with methyl B12 was positively correlated with increases in plasma methionine (p = 0.05), decreases in S-adenosyl-
Conclusions:
Methyl B12 treatment improved clinician-rated symptoms of ASD that were correlated with improvements in measures of methionine metabolism and cellular methylation capacity.
Clinical Trial Registry:
Efficacy Study of Subcutaneous Methyl B12 in Children with Autism: NCT01039792 (
Introduction
A
Many metabolic processes have shown specific deficits in children with ASD, including both cellular methylation and glutathione-mediated antioxidant defense (Rossignol and Frye 2012). In 2004, James et al. reported findings of a small study of 20 children with autism compared with 33 healthy controls, and found that children with autism had significantly lower plasma methionine, S-adenosylmethionine (SAM), homocysteine, cystathionine, cysteine, and total glutathione as well as significantly higher levels of S-adenosyl-
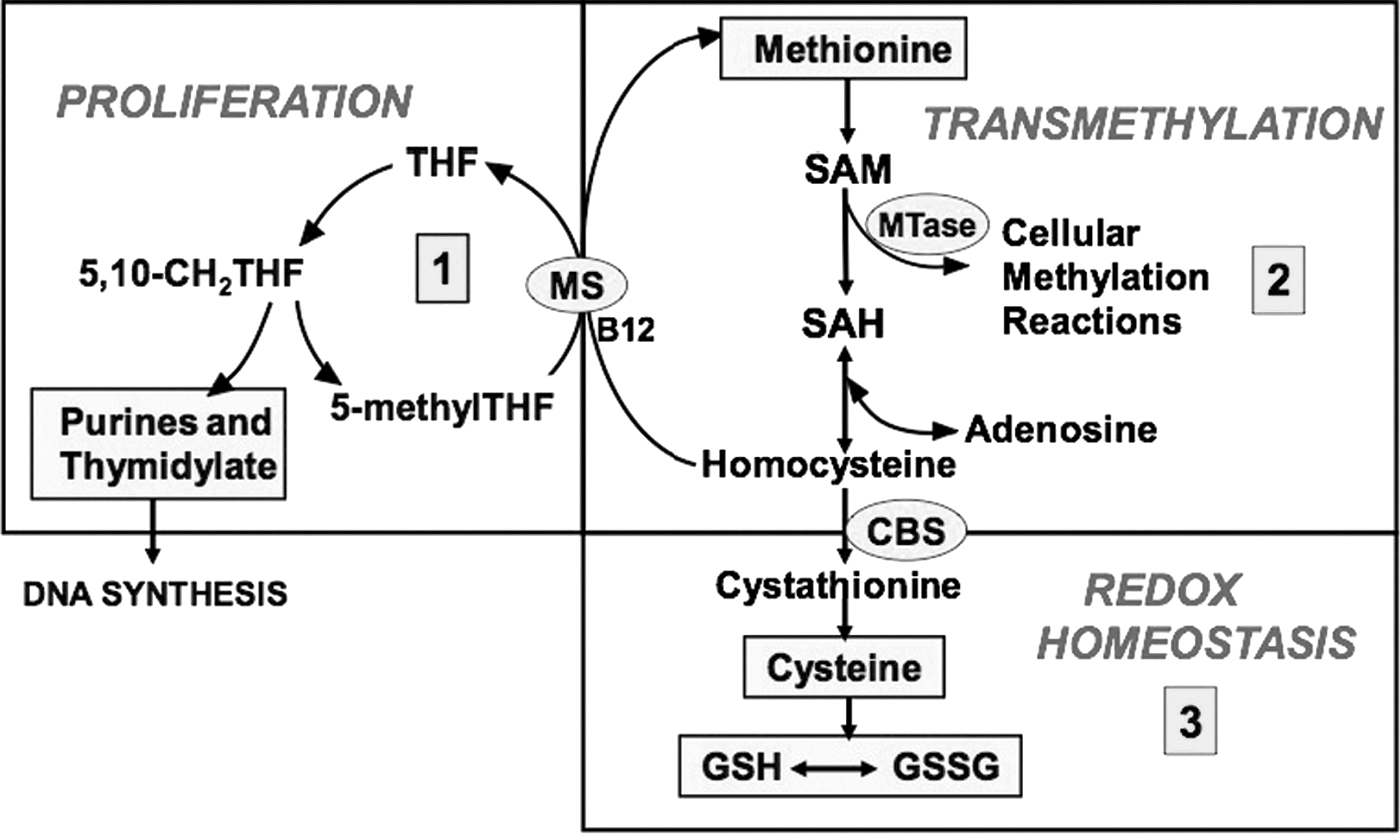
Folate (tetrahydrofolate [THF])-dependent methionine transmethylation/transsulfuration metabolism.
A second study in 2006 of 80 children with ASD and 73 controls again demonstrated the same pattern of methylation deficit and oxidative stress (James et al. 2006). A more recent study in 2012 examined 68 children with ASD, 40 unaffected siblings, and 54 age-matched unaffected, unrelated control children. Reduced methylation capacity was associated with DNA hypomethylation and reduced glutathione antioxidant defense in the children with ASD but not in their unaffected siblings or control children (Melnyk et al. 2012). Markers of protein and DNA oxidative damage were also found in the children with autism, suggesting that the reduced methylation and antioxidant capacity may have had a functional consequence. It is important to note that these metabolic and molecular indicators of methylation deficit and oxidative stress/damage were unique to the autism cohort and not present in their paired siblings with shared genes and environmental exposures.
Vitamin B12 is a key cofactor in methionine transmethylation/transsulfuration metabolism, and it has therefore been used empirically by many clinicians in attempt to improve methylation capacity (SAM/SAH) and the “redox status” of children with ASD, expressed as the ratio of reduced glutathione (GSH) to the oxidized disulfide form of glutathione (GSH/GSSG). As can be seen in Figure 1, supplementation with B12 has the potential to “drive” the cycle forward, increasing flux through the methylation cycle, which improves downstream glutathione levels (antioxidant capacity) and restores methionine and SAM/SAH (methylation capacity). The interdependence among folate, B12, and SAM and the importance of normal levels for optimal brain functioning has been discussed previously (Bottiglieri 2013). A 3 month open-label trial of injectable methyl B12 combined with folinic acid in 2009 in 40 children with ASD partially confirmed this hypothesis (James et al. 2009). Children supplemented with methyl B12 and folinic acid demonstrated significant increases in cysteine and glutathione (GSH) while reducing the oxidized inactive form of glutathione (GSSG), both consistent with improved antioxidant capacity. However, in this study, methionine and SAM/SAH did not improve, indicating no improvement in methylation capacity. Notably, 78% of parents expressed a desire to continue the supplementation after the 3 month study period, suggesting parental perception of a beneficial effect. In a description of the behavioral changes in 37 children with ASD out of this cohort, children showed improvements in all of the subscales of the Vineland Adaptive Behavior Scale and an average improvement in the overall age-equivalent score of 7.7 months during the 3 month study. In this analysis, improvements in plasma glutathione levels were significantly correlated with improvements in expressive communication, personal and domestic daily living skills, and interpersonal, play-leisure, and coping social skills as measured by the Vineland Adaptive Behavior Scale (Frye et al. 2013).
One prior small randomized, placebo-controlled trial of methyl B12 in 30 children with ASD did not find statistically significant improvements in the overall Clinical Global Impressions (CGI) score; however, a subset of children (9/30) showed clinically significant improvements in the CGI and improvements in glutathione levels, again suggesting that improvements in the antioxidant defense might lead to improvements in symptoms (Bertoglio et al. 2010).
In summary, prior studies suggest that some children with ASD have abnormal transmethylation/transsulfuration metabolism, consistent with an impaired cellular methylation and antioxidant defense. We therefore conducted a larger randomized controlled trial with greater power to determine if injectable methyl B12 improves behavior compared with placebo in children with ASD, and to determine if observed improvements are associated with improvements in transmethylation/transsulfuration metabolism.
Methods
Participants
The study protocol was approved by the Committee on Human Research at the University of California, San Francisco (UCSF) and the trial was registered prior to enrolling patients at
Children between the ages of 3 and 7 with a diagnosis of ASD were recruited from the Autism Clinic at UCSF through flyers, letters to families that had been seen previously, and advertisements on web sites. This age range was selected to be consistent with prior intervention studies of autism and because children at this relatively young age were felt to be likely to improve if given effective treatments. Informed consent was obtained from the parent/caregiver of all individual participants included in the study. The diagnosis of ASD was established with the Autism Diagnostic Interview-Revised (ADI-R) and the Autism Diagnostic Observation Scale (ADOS) (if the diagnosis was unclear from ADI-R) as well as through a clinical review by a child and adolescent psychiatrist experienced in autism diagnosis and treatment (R.L.H.). Parents of potentially eligible children participated in an informed consent process and children were then assessed for eligibility. Children were required to have an intelligence quotient (IQ)
Intervention
Eligible children were randomly assigned to 8 weeks of treatment with methylcobalamin (methyl B12) at a dosage of 75 μg/kg or a saline placebo of identical volume given through a subcutaneous injection every 3 days. The dose of 75 μg/kg was chosen based on discussions with practitioners who commonly use methyl B12 in large practices of children with ASD, and the subcutaneous route is believed to provide more sustained levels than oral, intramuscular, or nasal administration. We decided not to include folinic acid because we sought to examine the unique effects of methyl B12. Methyl B12 and normal saline injections were obtained from Wellness Health & Pharmacy (Birmingham, AL) in prepared syringes. Syringes were tightly taped with opaque material to hide the color of the liquid, as methyl B12 is deep red and a matching and safe red dye for the injectable placebo could not be identified. Families were given instructions on injection technique and practiced using saline injections into an orange before giving an injection to their child. All injections were performed at home by the parents. Parents were advised that some of the injection material was colored, and they should not worry if they saw red, which was just color and not blood. Parents were provided a sharps container where they placed the syringes after home use. Study staff did not view the used syringes or the sharps container. Compliance was measured by questioning the parents at each study visit.
Objectives and outcomes
The primary outcome measure was defined a priori as a comparison of the CGI-Improvement (CGI-I) scale between the methyl B12 and placebo groups after the 8 week study period. The CGI-I is a measure of improvement in the overall symptom burden of ASD and has the following scoring: 1-very much improved; 2-much improved; 3-minimal improvement; 4-no change; 5-minimally worse; 6-much worse; 7-very much worse. The CGI-I was rated by a single expert clinician observer (R.L.H.) for all participants for the duration of the study based on observation of the child in the office and at blood draws as well as discussion with the family and the study coordinators who performed study procedures. Rating scales were not reviewed prior to the CGI-I rating, because they were viewed as separate measures. We also assessed the percentage of children in each group who responded to treatment, which was defined as a GCI-I rating of “much improved” or “very much improved,” a common metric of improvement in prior clinical trials of ASD.
Secondary outcomes of the study included changes in behavior as measured by the Aberrant Behavior Checklist (ABC) and changes in social functioning as measured by the Social Responsiveness Scale (SRS). Both instruments were completed by the parent/caregiver, and are well validated and commonly used to assess changes in symptoms in children with ASD. Study staff and the study clinician asked parents at each study visit whether their child had experienced any adverse medical events.
Laboratory evaluation
Laboratory assessments were conducted at baseline and 8 weeks, and the primary goals were to: 1. Determine if any baseline laboratory values could predict which children would respond to methyl B12 2. Determine if any changes in laboratory values were correlated with changes in overall symptom burden, as measured by the CGI-I
Children were asked to fast for at least 12 hours prior to a morning (8:00 a.m.) laboratory draw to assess measures of antioxidant function. Fasting was verified by direct inquiry of parents prior to the laboratory draw. Laboratory assessments were performed within the same week as the outcome assessments, but on a different day, so that fasting status would not affect child behavior. The methodological details for high performance liquid chromatography (HPLC) elution and electrochemical detection have been described previously (Melnyk et al. 1999, 2000).
Randomization and blinding
Eligible participants were randomized in equal proportions to methyl B12 or placebo. The compounding pharmacy held the computer-generated randomization list, which was prepared prior to the initiation of the study. Each new participant was assigned to the next position on the randomization list, and the pharmacy express-mailed the study medication to the study families directly. All participants, families, and study personnel were blinded to group assignment and the randomized sequence list for the entire study.
Statistical methods
The primary outcome measure, the mean CGI-I, was compared between the active and placebo groups at the end of the 8 week study period using an independent group t test. Prior to the study, we determined that 50 subjects would be required to obtain a power of 93% to detect a two point change in the CGI-I using a two sided α of 0.05. The independent group t test was used for the comparison of change of the secondary outcome measures, which are continuous variables. Laboratory tests were compared using a nonparametric Mann–Whitney test. Categorical variables (responder vs. nonresponder) were compared using Fisher's exact test. Correlations between baseline values or change in laboratory values and clinical improvement (CGI-I) were computed using nonparametric Spearman correlations. The proportion of children experiencing an adverse event in each treatment group was compared using the χ2 test. All analyses were completed with SAS, version 9.3. All reported p values are two sided, and not adjusted for multiple testing as recommended by Rothman to reduce the likelihood of missing important associations and to allow the evaluation of each association in the context of other factors (Rothman 1990). If patients discontinued study medication, they were asked to complete all outcome assessments at the regularly scheduled 8 week follow-up visit, and they were analyzed in their assigned treatment group.
Results
During the 2 year recruitment period, 61 patients were identified and screened. Fifty-seven participants met all inclusion criteria and were randomly assigned to methyl B12 or placebo. Reasons for exclusion are shown in Figure 2.
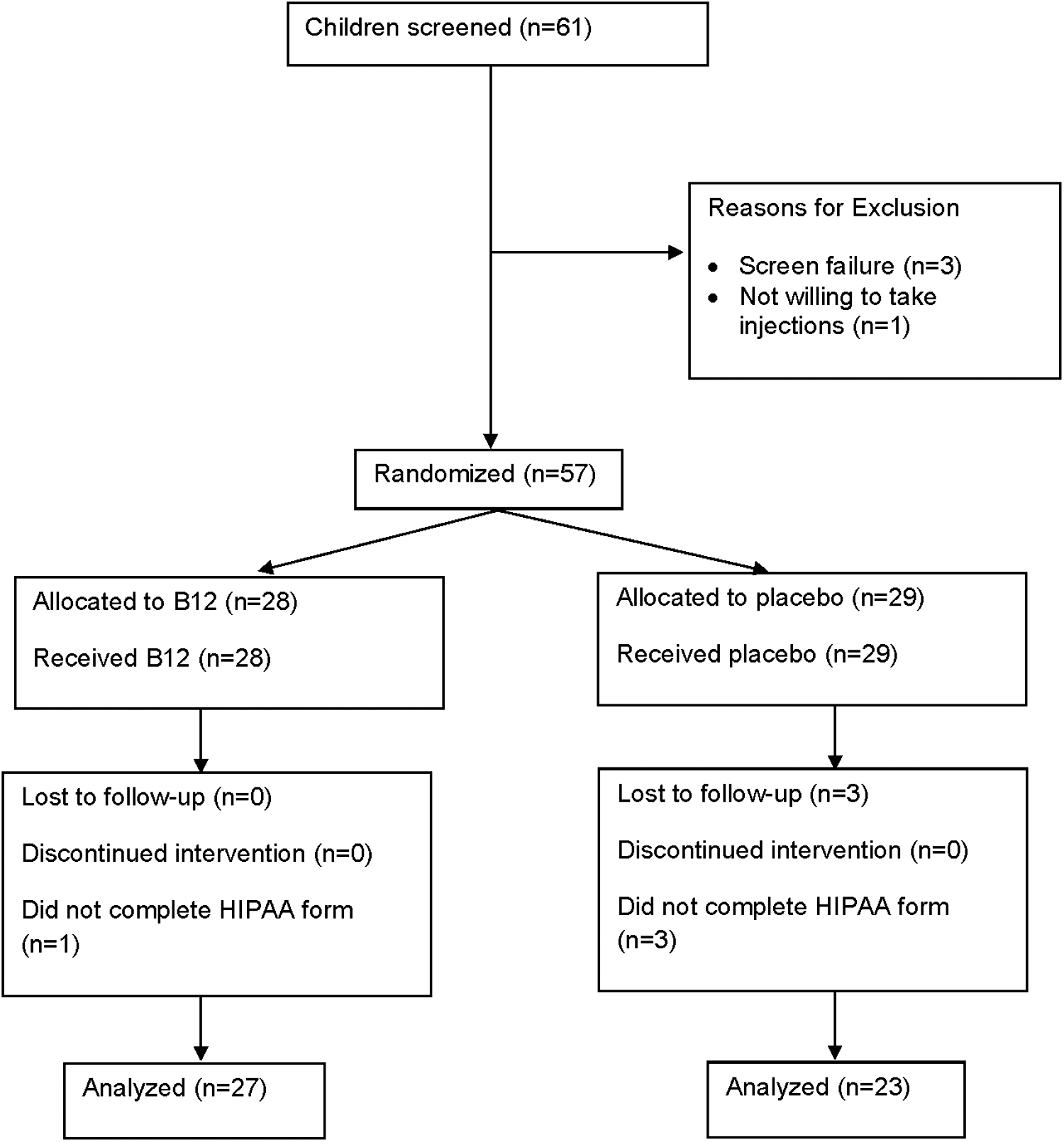
Flow diagram showing distribution of participants at each stage.
Four participants were excluded from analyses because they were given the incorrect Health Insurance Portability and Accountability Act (HIPAA) form at the outset of the study and were not able to be reached to complete the correct form; therefore, their data could not be used. Three participants in the placebo group were lost to follow-up and did not complete the primary outcome measure at any point post-randomization; therefore, they could not be included in the analyses. All participating families reported compliance with all scheduled methyl B12 injections.
Baseline characteristics of the treatment groups were similar. Children in the study had a mean age of 63 months (5.3 years) and 45 out of 57 were male (79 %) (Table 1).
IQ, intelligence quotient; ABC, Aberrant Behavior Checklist; SRS, Social Responsiveness Scale.
Both groups had a similar baseline severity of ASD, with a CGI-Severity (CGI-S) score of 5.1 (CGI-S scores range from 1 to 7, and 5 indicates markedly ill). Baseline scores were also similar for the total score and subscales of the ABC and the SRS.
The primary outcome measure – the mean CGI-I score at 8 weeks – was statistically significantly better (lower) in the methyl B12 group (2.4) than in the placebo group (3.1) (0.7 greater improvement in the methyl B12 group, 95% CI 1.2–0.2, p = 0.005), indicating a greater overall improvement in patients treated with methyl B12 (Table 2).
p < 0.05.
CGI, Clinical Global Impressions; ABC, Aberrant Behavior Checklist; SRS, Social Responsiveness Scale.
We also assessed the percentage of patients in each group who were rated as “much improved” or “very much improved” (the responder group), a common metric of improvement in prior clinical trials of ASD. In the B12 group, 14/27 children (52%) were responders compared with 6/23 (26%) in the placebo group (p = 0.086).
Secondary outcome measures
None of the secondary outcome measures showed changes that indicated statistically significant improvements favoring the B12 over the placebo group. In one subscale of the SRS (motivation subscale), there was a statistically significantly greater improvement in the placebo group (6.3 point greater improvement in the placebo group, p = 0.02), and in the ABC irritability subscale, there was a borderline greater improvement in the placebo group (p = 0.08). There were no statistically significant differences in the changes in the overall scores or the other subscales of the ABC or the SRS.
Laboratory analyses
The mean values at baseline and week 8, and the change in mean values for each of the metabolites in the methylation pathway are shown in Table 3 for all participants with fasting laboratory values in the B12 (n = 17) and placebo (n = 12) groups. There were no statistically significant differences in the changes in the laboratory values over the course of the study in the B12 versus the placebo group.
Methion., methionine; SAM, S-adenosylmethionine; SAH, S-adenosyl-
We sought to determine if changes in specific metabolites were associated with clinical improvements in children in the B12 group (Table 4).
p values reflect the statistical significance of the correlation between changes in the laboratory value and CGI-I at 8 weeks.
Corr indicates the correlation between the change in laboratory value and change in CGI-I score at 8 weeks (where negative correlations indicate that increases in the laboratory values are correlated with improvements, or decreases, in CGI-I score, and positive correlations indicate that decreases in the laboratory values are correlated with improvements, or decreases, in GGI-I score).
CGI-I, Clinical Global Impressions – Improvement; Methion., methionine; SAM, S-adenosylmethionine; SAH, S-adenosyl-
Clinical improvement as measured by the CGI-I scale was statistically significantly correlated with increases in methionine (p = 0.05), decreases in SAH (p = 0.007), and improvements in the SAM/SAH ratio (p = 0.007). For these three laboratory tests that showed statistically significant correlations with clinical improvement, we compared changes in laboratory values and changes in clinical status (CGI-I) between the B12 and placebo groups using scatterplots (Fig. 3). In each case, the regression lines for the B12 group visually demonstrate the correlation between change in laboratory value and improvement in CGI-I, whereas no correlation between change in laboratory value and change in CGI-I is seen in the placebo group. The differences in the slope of these regression lines did not reach statistical significance (p = 0.051 for SAH, p = 0.42 for methionine, and p = 0.091 for SAM/SAH).
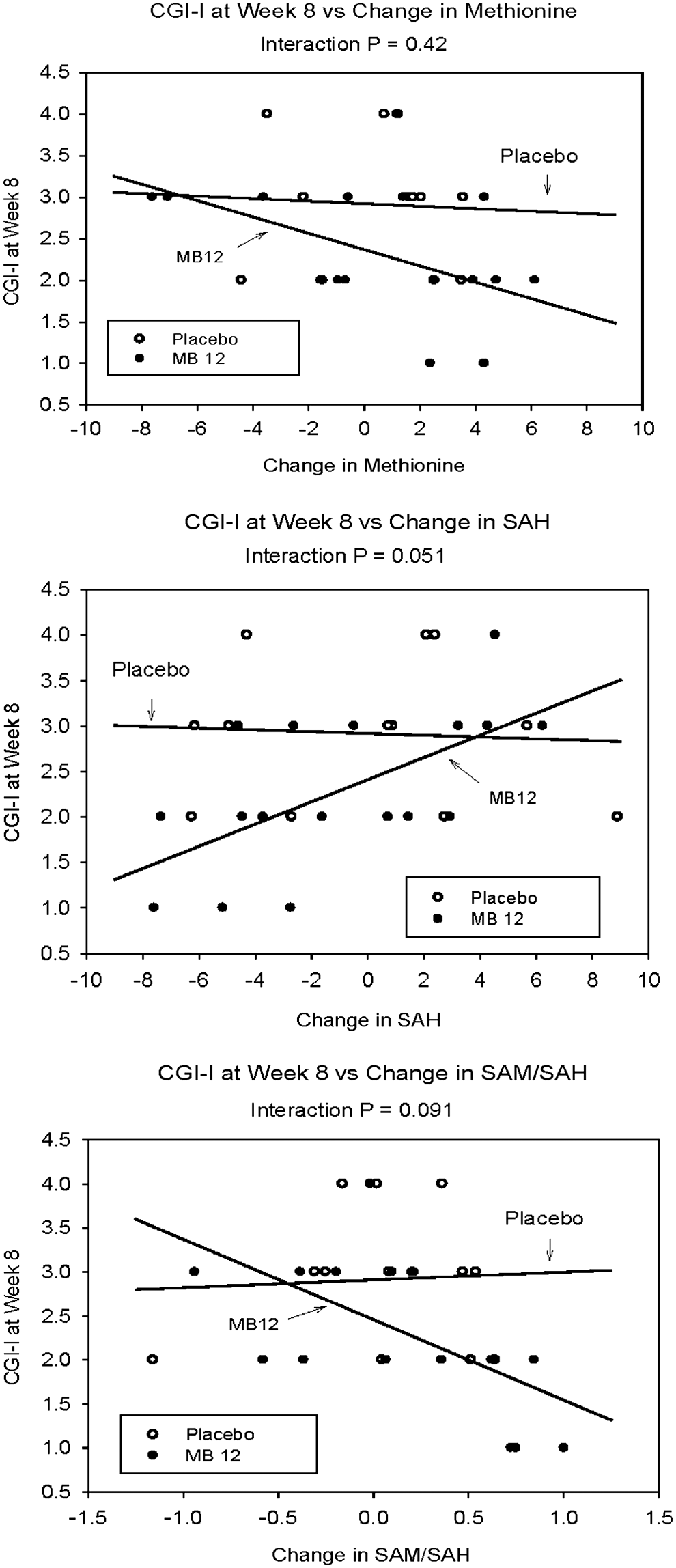
Scatterplot of changes in laboratory value versus Clinical Global Impressions-Improvement (CGI-I) at 8 weeks in B12 group.
We also sought to determine if values of baseline laboratory tests would predict which patients would be more likely to have a clinical response to methyl B12. Among patients in the methyl B12 group, those who responded to methyl B12 had a statistically significantly lower baseline value of methionine (p = 0.006), suggesting that those with the most impaired methylation capacity (lowest methionine) are most likely to achieve a clinical benefit from vitamin B12 (Table 5).
Adverse events
There were no serious adverse events in either group during the course of the study, and the number of adverse events was similar in each group (21 in the methyl B12 group versus 24 in the placebo group – Table 6). No adverse events were statistically significantly increased among methyl B12 treated children.
Discussion
In this study, children with ASD who were treated with injectable methyl B12 had a statistically significant improvement in overall clinician-rated symptoms compared with children treated with placebo injections. The magnitude of this change, 0.7 points of the CGI-I scale when treated as a continuous variable, indicates a large effect size of 0.84. Treating the CGI-I as a continuous variable is a more sensitive method for detecting differences between treatment groups, because it includes patients who had “minimal improvement,” and the inclusion of this category in the continuous measure likely explains why it was statistically significant, whereas the analysis examining the percentage of responders in each group (defined as “much improved or very improved”) did not show statistical significance (p = 0.086). Methyl B12 was well tolerated and did not produce side effects at a greater rate than placebo in this 8 week study.
The rationale for this study was based on prior studies demonstrating that children with ASD have metabolic markers indicating methylation deficit and oxidative stress, as described in the Introduction. We hypothesized that improvements in transmethylation/transsulfuration metabolites would be associated with improvements in symptoms, and we found this to be partially correct. Clinical improvement in symptoms as measured by the CGI-I were statistically significantly correlated with changes in three metabolites – methionine, SAH, and the SAM/SAH ratio – and all of those changes indicate improvements in methylation capacity. Further, we found that children who responded to methyl B12 had statistically significantly lower baseline levels of methionine, suggesting that children with more severe methylation deficit at baseline were more likely to respond to treatment. Methionine is one of eight essential amino acids required for the synthesis of body proteins as well as a number of crucial functions, including the ribosomal initiation of protein synthesis, and is a modulator of metabolic flux and catalytic activities (Ingenbleek and Kimura 2013). The finding that treatment with B12 both improves clinical symptoms and is more likely to produce a clinical response in patients with a low baseline level of methionine adds strength to these findings, and suggests that methyl B12 may be a valuable treatment for a defined subset of children with ASD.
Interestingly, we did not find that methyl B12 improved measures of oxidative stress (GSH/GSSG), which was seen in a previous open-label trial of 40 children with ASD (James et al. 2009). In the previous study, James et al. screened children for metabolic evidence of reduced methylation capacity (SAM/SAH) and reduced antioxidant capacity (GSH/GSSG) as an inclusion criterion to increase sensitivity, and included folinic acid as a combined treatment with the methyl B12. Because we did not screen for low antioxidant capacity in the current study, we may have lacked the power to detect any changes in the subset of children with baseline reduced antioxidant capacity. However, even though the current study did not prescreen for abnormal baseline methylation capacity, we still observed a statistically significant correlation between changes in methionine, SAH, and SAM/SAH and improvements in clinical behavior. The fact that a correlation between changes in laboratory values was observed without a statistically significant change in the mean laboratory values over the course of the study suggests that only a subset of patients (those with impaired methylation capacity) may respond to treatment with methyl B12.
Limitations
This study has a number of important limitations. The most significant are the relatively small sample size and the fact that many children were not able to adequately adhere to the laboratory instructions to fast prior to laboratory draws; therefore, only a subset (17 of 27 or 63%) had valid laboratory information. The laboratory analyses were also performed at a site remote from the clinical site, and it is possible that overnight shipping of laboratory samples (on dry ice) affected the levels of the reported tests, although samples were shipped in batches from all subjects. This limited laboratory assessment limits the power of our analyses to detect differences in laboratory values between groups. Although it is possible that this could significantly affect the overall laboratory results, we do not think it would produce the statistically significant associations observed in the three metabolites. Second, although we observed an improvement in the primary outcome measure – the CGI-I – we did not find improvements in the secondary outcome measures (ABC and SRS). This may be because of a lack of sensitivity of these outcome measures, improvements in other symptom areas that are not captured by these surveys, or improvements that were noted only by the clinician assessment and not by the parents (who completed the ABC and SRS). Inclusion of other measures, such as the Vineland Adaptive Behavior Scale, would have allowed an assessment of changes in adaptive behavior and may have provided an explanation for the observed improvement in the CGI-I. We did find statistically significant improvement in the motivation subscale of the SRS in the placebo group, and given the lack of other improvements, we believe that this is most likely a chance finding that is not clinically significant. Third, we were unable to identify a safe red dye to match the placebo color to the color of injectable methyl B12, and although we masked the syringes with opaque material, it is possible that some families were able to perceive that their injected material was colored (although it is not clear that this would hold any meaning for the families). Also, the clinician assessing the primary outcome (CGI-I) was blinded to group assignment and did not see the injection liquid or the syringes. Finally, although this study is the largest randomized, placebo-controlled trial of methyl B12 in autism, it still involves a relatively small sample size, was of short duration, included only children with an IQ >50, and did not assess for other psychiatric comorbidities, all of which make the findings provocative but in need of corroboration by future investigations.
Conclusions
In summary, this study demonstrated that treatment with methyl B12 led to improvements in clinician-rated symptoms of autism that were correlated with improvements in transmethylation metabolism. Although the findings are preliminary, this is an exciting finding that suggests that treating a known metabolic abnormality – impaired methylation capacity – holds the potential to improve symptoms. A larger randomized controlled trial with greater power and greater control over laboratory assessments should be a high priority.
Clinical Significance
It may eventually be possible to screen children with ASD for impaired methylation capacity (low methionine) or low glutathione antioxidant capacity, and predict which children are most likely to respond to treatment. If future investigations confirm these findings, methyl B12 may be a useful treatment option for children with autism and impaired methylation capacity.
Footnotes
Acknowledgments
We gratefully acknowledge the families and children who participated in this study to help advance scientific research in autism. A poster of the results of this study was presented at the annual meeting of the American Academy of Child and Adolescent Psychiatry (San Diego, CA, October 24, 2014).
Disclosures
In the past year, Dr. Robert Hendren has received research grants from Autism Speaks, BioMarin Pharmaceutical, Curemark, Forest Pharmaceuticals, Inc., Roche, Shire, Sunovion, and the Vitamin D Council. He is on Advisory Boards for BioMarin, Forest, Janssen, and Neuren, and has been a reviewer for Autism Speaks, Brain Canada, and the Simons Foundation. This study was supported by a grant from Autism Speaks (grant #3031, to Dr. Hendren). The funding agency and the manufacturer of methyl B12 (which was purchased and not donated) had no role in the design of the study; the collection, management, analysis, and interpretation of the data; or the preparation, review, and approval of the manuscript. The other authors have nothing to disclose.