
Abstract
Objective:
To explore predictors of 8-year school-based behavioral outcomes in attention-deficit/hyperactivity disorder (ADHD).
Methods:
We examined potential baseline predictors of school-based behavioral outcomes in children who completed the 8-year follow-up in the multimodal treatment study of children with ADHD. Stepwise logistic regression and receiver operating characteristic (ROC) analysis identified baseline predictors that were associated with a higher risk of truancy, school discipline, and in-school fights.
Results:
Stepwise regression analysis explained between 8.1% (in-school fights) and 12.0% (school discipline) of the total variance in school-based behavioral outcomes. Logistic regression identified several baseline characteristics that were associated with school-based behavioral difficulties 8 years later, including being male (associated with truancy and school discipline), African American (school discipline, in-school fights), increased conduct disorder (CD) symptoms (truancy), decreased affection from parents (school discipline), ADHD severity (in-school fights), and study site (truancy and school discipline). ROC analyses identified the most discriminative predictors of truancy, school discipline, and in-school fights, which were Aggression and Conduct Problem Scale Total score, family income, and race, respectively.
Conclusions:
A modest, but nontrivial portion of school-based behavioral outcomes, was predicted by baseline childhood characteristics. Exploratory analyses identified modifiable (lack of paternal involvement, lower parental knowledge of behavioral principles, and parental use of physical punishment), somewhat modifiable (income and having comorbid CD), and nonmodifiable (African American and male) factors that were associated with school-based behavioral difficulties. Future research should confirm that the associations between earlier specific parenting behaviors and poor subsequent school-based behavioral outcomes are, indeed, causally related and independent cooccurring childhood psychopathology. Future research might target increasing paternal involvement and parental knowledge of behavioral principles and reducing use of physical punishment to improve school-based behavioral outcomes in children with ADHD.
Introduction
C
There have been some studies that review school-based outcome findings of the multimodal treatment study of children with ADHD (MTA). They have particularly demonstrated that improvements in negative/ineffective parental discipline were associated with decreased disruptive behavior at school and that the behavioral intervention in MTA was the most effective in reducing homework problems over the 12 months of the randomized trial (Hinshaw 2007; Langberg et al. 2010). Although the school-based impairments associated with ADHD are well described, little research has examined predictors or risk factors associated with later school-based behavioral difficulties (i.e., truancy, school discipline, and in-school fights).
The MTA was a 14-month study that assessed the effectiveness of behavioral treatment, medication management, and combined treatments, which were evaluated with community treatment (MTA 1999). The MTA was beneficial in providing the foundation for existing evidence about the comparative effectiveness of different treatments for childhood ADHD. The MTA established that children with ADHD who received community treatment suffered poorer outcomes throughout the 14 months when compared with children who obtained medication management. Furthermore, pharmacological treatment, primarily with stimulant medications, provided better overall results than the behavioral treatment for the first 14 months (MTA 1999).
Additional secondary analyses of the MTA recommended that an added behavioral intervention with ideal medication management enhanced the treatment of children with ADHD, in comparison to treatment solely with medication (Swanson et al. 2001). The MTA collected a plethora of baseline demographic, clinical, environmental, social, neuropsychological, and relationship data on each subject enrolled and continued to follow the participants for more than a decade to observe the long-term outcomes associated with ADHD (Molina et al. 2009). To our knowledge, no research has examined adverse school behavioral outcomes in children with ADHD in the MTA cohort.
Our goal is to conduct a secondary analysis of 8-year follow-up data from the MTA to examine frequency and predictors of adverse school behavioral outcomes in children with ADHD. Specifically, we will examine (1) truancy, (2) school discipline, and (3) in-school fights as our primary outcomes. We will examine baseline predictors of 8-year adverse school-based outcomes in the MTA by using stepwise regression techniques and receiver operating characteristic (ROC) analysis.
Methods
Study overview
The goals, rationale, and methods of the MTA have been previously described (Richters et al. 1995; Arnold et al. 1997; MTA 1999). Participants and their respective guardians gave informed consent and assent. The National Institutes of Health and the Institutional Review Boards at each site approved the research protocol.
Subjects
Children 7–9 years of age were recruited from 6 sites across the United States and Canada. Subjects were required to meet the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) standards for ADHD combined type, as diagnosed by the Diagnostic Interview Schedule for Children (DISC) with a paper-and-pencil version of the new DISC 4 (Shaffer et al. 2000). Exclusion criteria included: physical restrictions that prohibited participation in any portion of the study (i.e., intolerance to MTA medications in the past, non-English speaking guardian, and hospitalization) or having a condition or partaking in other treatments that were incompatible with any of the possible MTA treatment assignments (i.e., Tourette syndrome, neuroleptic medications in the past six months, and bipolar disorder).
Parents of children included in the initial MTA study were additionally asked to participate in the 8-year follow-up interview, which included the Services for Children and Adolescents-Parent Interview (SCA-PI) Summary Misbehaviors and Justice Contact Variables in Yearly Increments Questionnaire (Eaton Hoagwood et al. 2004; Jensen et al. 2004). Parents were required to complete this assessment at 8-year follow-up for subjects to be included in the current sample for data analysis.
Assessment
As part of the MTA, participants were assessed at baseline and at other time points over eight years. All outcome variables were assessed at the 8-year follow-up for presence during the previous year, as reported by the parent.
Truancy was considered present if the following question was answered with “yes” (otherwise not): “Did the child skip school or was the child truant during this interval (previous year)?” School discipline was considered present if any of the following six questions were answered with “yes” (otherwise not): “Did the child receive a detention from school during this interval?,” “Did the child receive an in-school suspension during this interval?,” “Did the child receive an out-of-school suspension during this interval?,” “Was the child expelled from school during this interval?,” “Was the child sent home early from school during this interval?,” “Was the child given any other school punishment during this interval?” In-school fights were considered present if either of the following questions was answered with “yes” (otherwise not): “Did the child have fights with other children in school during this interval?,” “Did the child have fights with teachers during this interval?”
All outcome variables were preselected before conducting predictor analyses. These outcomes were chosen based on consultation between the included authors as potentially clinically meaningful, practical long-term outcomes in terms of school-based behavioral difficulties. Truancy, in-school fights, and school discipline are associated with school drop-out, future arrests, vocational difficulties, and so on (Fergusson and Horwood 1998; Woodward and Fergusson 2000; Yen and Wang 2009; Dembo et al. 2014; Doria et al. 2015).
Several additional measures were collected at baseline and utilized in predictor analysis. A demographic questionnaire was used to assess sex, race, age, pre- and post-term birth, parental education level, and size of city that was most lived in by the participant. Neuropsychological testing of the child included the Continuous Performance Task (CPT)—measuring dyscontrol, impulsivity, and inattention scores (Mani et al. 2005) and the Wechsler Intelligence Scale for Children (WISC III) measuring performance, verbal, and full scale IQ (Kaufman 1994).
ADHD symptoms and oppositional/aggressive symptoms were measured with the respective subscales of the parent-and-teacher-completed Swanson, Nolan and Pelham Questionnaire (SNAP) (Swanson 1992). The Multidimensional Anxiety Scale for Children (MASC) administered to the child was utilized to rate anxiety symptoms at baseline (March et al. 1997). A child self-report scale was utilized to evaluate the total number of antisocial behavior and subscale scores (physical aggression, stealing, and property destruction) (Loeber et al. 1989). Axis I comorbidities were determined by using the parent version of the DISC 3.0 (Shaffer et al. 2000).
The Child Behavior Checklist (CBCL) completed by the parent was utilized to assess social problems and internalizing and externalizing scores (Achenbach and Edelbrock 1983). Assertiveness, cooperation, externalizing and internalizing behavior, hyperactivity, responsibility, and social conduct in the child were measured by using parental ratings on the Social Skills Rating System (SSRS) (Gresham and Elliott 1990). Aggression and conduct disorder (CD) symptoms were assessed by using parental ratings on the Aggression and Conduct Problems Scale (ACPS) (parent version) (American Psychiatric Association 2000).
The Alabama Parenting Questionnaire (APQ) evaluated parental involvement and discipline subscales (Essau 2006). Characteristics of the parent-child relationship (i.e., admiration by parent, deprivation of privileges, dominance, guilt induction, intimacy, praise, pro-social behavior, quarreling, rationale, similarity, verbal, and physical punishment) were rated by the parent by using the Parent-Child Relationship Questionnaire (PRQ) (Furman and Gierson 1995). A questionnaire was administered to the parent to measure parental knowledge of behavioral principles (O'Dell et al. 1979). The Parental Stress Index (PSI) was administered to parents to assess parental stress and child difficulty (Abidin 1990). The Beck Depression Inventory (BDI) measured parental depression symptoms (Beck 1961). The Structured Clinical Interview for DSM-IV (SCID-II) was utilized to determine parental psychopathology and parental history of antisocial personality disorder or CD (First et al. 1997). For further details on the assessments included in the MTA, please refer the original MTA publications (Hinshaw et al. 1997).
Intervention
Participants were randomized to 1 of 4 treatment groups (behavioral treatment, medication management, medication management plus behavioral intervention, and community care) over 14 months. The treatments were accommodating to each respective patient's clinical needs over the course of the treatment period. Treatment management of each of the randomized treatment groups has been previously described (Greenhill et al. 1996; MTA 1999; Wells et al. 2000). From 14 months after randomization to 8-year follow-up, participants were treated in an uncontrolled manner in the community, but had semiregular assessments from study staff.
Data analysis
The Statistical Analysis System (SAS version 9.2) and Microsoft Excel were used to perform data preparation and analysis. SAS was used for stepwise regression models, whereas the ROC analysis was completed by using free software available online from Ruth O'Hara at Stanford University (
Logistic regression models measured the relationship of the clinical, demographic, and social characteristics with long-term outcome at 8-year follow-up. Three outcome variables were calculated: (1) truancy, (2) school discipline, and (3) in-school fights. The presence of truancy, school discipline, and in-school fights was based on whether parents responded affirmatively to any of the specific questions in that category as described earlier in the Assessment section. To make better use of the available data, we used two complementary statistical techniques: stepwise regression and ROC analysis.
Our regression technique, which followed an approach developed by Fournier et al. (2009), has been applied to logistic regression in previous studies (Powers et al. 2014). We selected this method not only to allow for an exploratory examination of a large number of potential predictor variables, but also to reduce the likelihood of false-positive error and to limit problems with colinearity (since limited variables are included from each domain).
Before the analysis, predictor variables were rationally divided into seven domains (demographic, trial factors, cognitive functioning, comorbid psychopathology, family history, parent-child relationship, and parental variables). The following steps were carried out in each individual domain separately: Step 1 tested a full model, including all variables and their interactions with treatment. Step 2 repeated the analysis while retaining predictors with p < 0.20 from step 1. Step 3 repeated the analysis while retaining predictors with p < 0.10 from step 2. Step 4 repeated the analysis while keeping predictors with p < 0.05 from step 3. Step 4 was repeated until all predictors in the model were significant at p < 0.05. Significant predictors across each domain were then included into a combined model. The same four-step procedure was then repeated for the variables that were included in the combined model. Continuous predictors were centered at the grand mean, and dichotomous predictors were coded as −0.5 and 0.5 (Kraemer et al. 2002).
A total of three models were performed while examining truancy, school discipline, and in-school fights. Our primary outcome measure for logistic regression was risk ratio. For continuous or ordinal variables, the odds ratio represents a one-unit increase on the scale.
ROC analysis was used as an alternative prediction model. ROC analysis is a nonparametric method that operates via recursive partitioning. It aims at identifying subgroups of individuals who have a higher or lower probability of achieving a particular binary outcome (Kraemer 1992). Truancy, school discipline, and in-school fights were utilized as the binary outcome for ROC analysis.
For each measured potential predictor, cut-off points were generated at all values observed in the variable. The quality of a cut-off point was defined by its ability to divide the sample into two subsamples, which were maximally distinct in the specified binary outcome. The cut-off point that yields the best prediction was identified across all values of all variables. That cut-off point was then used to divide the total sample in two subsamples. The same procedure was repeated systematically in each of the two subsamples.
This iterative process continues until a stopping criterion is reached. The stopping criteria for ROC analysis are either a subgroup size of less than 10 individuals or a failure to reach a significant group difference at p < 0.05 for any candidate cut-off value. After the last step of the ROC analysis was reached, we calculated the probability of worsening and emergence and presented results as hierarchical decision tree diagrams. The models were calculated by using the same predictors as those used in previous regression models.
The following baseline characteristics were entered as predictor variables into both models (by domain for regression analysis):
The demographic domain included sex, race, age, size of city that was most lived in by the participant, parental welfare, and income status. Material about medical history, such as neonatal history (pregnancy length, birth weight, and nicotine exposure), was also incorporated. Randomized treatment assignment was also included as a predictor.
The trial factors domain included (1) study site, (2) randomized treatment assignment, and (3) the interaction between site and treatment assignment.
The cognitive domain contained CPT (dyscontrol, impulsivity, and inattention) (Riccio 2004) and WISC III (performance, verbal, and full scale IQ) (Kaufman 1994).
The comorbid psychopathology domain contained DISC 3.0 [anxiety (separation and generalized), phobia (simple and social), panic disorder, tics (chronic and transient), depression] (Shaffer et al. 2000), MASC (March et al. 1997), total number of self-reported antisocial behaviors and subscales (physical aggression, property destruction, and stealing behaviors) (Loeber et al. 1989), CBCL total score and subscales (social problems and internalizing and externalizing symptoms) (Achenbach and Edelbrock 1983), SSRS total score and subscales (cooperativeness, externalizing and internalizing, hyperactivity, responsibility, and social conduct) (Gresham and Elliott 1990), and the ACPS total score and subscales (aggression and CD symptoms) (American Psychiatric Association 2000). Mean SNAP ADHD total score at baseline was an average of the first 18 items on the SNAP parent ratings.
The family history domain included a family history of a first-degree relative with ADHD, substance abuse, anxiety, depression, obsessive-compulsive disorder (OCD), previous incarceration, psychiatric hospitalization, Tourette syndrome, or tics (Shaffer et al. 2000).
The parent-child relationship domain included the APQ parent-rated parental involvement, discipline (inconsistent, harsh, and appropriate), positive parenting and supervision subscales (Essau 2006), and the parent and child ratings from the PRQ subscales (admiration [of and for parent/child], affection, companionship, deprivation of privileges, dominance, guilt induction, intimacy, praise, pro-social behaviors, protectiveness, quarreling, rationale, shared decision making, similarity, and verbal and physical punishment) (Furman and Gierson 1995).
The parental variables domain included parental knowledge about behavioral principles (O'Dell et al. 1979), PSI total score and subscales (defensive responding, parent distress, parent-child dysfunction, and difficulty of child) (Abidin 1990), BDI (Beck 1961), APS for the SCID (parental history of CD) (First et al. 1997), and information on parental marital status, education level, and employment status. Due to colinearity issues, both the PSI total score and its subscales were entered into separate regression models of the parent-child relationship domain. The model with the higher R2 value was retained and entered into the combined model (if each model had any factors that remained significant).
For an additional sensitivity analysis, all variables related to CD (i.e., self-reported antisocial behaviors and ACPS as well as associated subscales) were removed from the model to determine how much of the predictive power of the model was attributable to CD symptoms that partially overlapped with the school-based behavioral outcomes.
Results
Subjects
Depending on the outcome, 425–437 participants from 579 eligible subjects completed the 8-year follow-up assessments (73%–75% of eligible subjects). Twenty-seven percent of participants reported truancy during the previous year, 18% reported being in a fight at school, and 47% reported school discipline.
Table 1 compares participants and nonparticipants in the follow-up analysis on baseline characteristics. Nonparticipants at 8-year follow-up were more likely to have the following characteristics at baseline assessment: be older (t = 1.99, p = 0.05), not Caucasian (χ2 = 5.91, p = 0.02), have a lower full-scale IQ (t = −2.85, p = 0.005), lower household income (t = −2.06, p = 0.04), lower family educational level [maternal (t = −3.55, p < 0.001), lower paternal involvement (t = −2.14, p = 0.03)], higher CPT impulsivity score (t = 3.18, p = 0.002), higher likelihood of a family history of anxiety (χ2 = 8.33, p = 0.004) and OCD (χ2 = 11.65, p < 0.001), a lower likelihood of a family history of depression (χ2 = 6.50, p = 0.01) and psychiatric hospitalization (χ2 = 5.92, p = 0.02), and a lower parental knowledge of behavioral principles (t = −2.30, p = 0.02).
The bold font in this table emphasizes the differences between participants and non-participants at follow-up. The variables in bold represent characteristics that were present significantly more in participants as compared to non-participants.
Displays baseline clinical characteristics of participants and nonparticipants in the 8-year MTA follow-up for academic behavioral outcomes. t-Tests and chi-square tests were conducted to examine differences between groups and are displayed.
ADHD, attention-deficit/hyperactivity disorder; CPT, Continuous Performance Task; GAD, generalized anxiety disorder; IQ, intelligence quotient; MTA, Multimodal Treatment Study of Children with ADHD; OCD, obsessive-compulsive disorder; SD, standard deviation.
Agreement between school-based behavioral outcomes
The level of agreement between the three school-based behavioral outcome variables was low. The kappa between in-school fights and school discipline was 0.25, the kappa between truancy and school discipline was 0.23, and the kappa between truancy and in-school fights was 0.08.
Truancy
Significant predictor variables were identified in five domains (demographic, trial factors, comorbid psychopathology, parent-child relationship, and parental variables). In the final model, being male [RR = 1.15, 95% confidence interval (95% CI) (1.02–1.29), p = 0.02], older [RR = 1.11, 95% CI (1.03–1.19), p = 0.006], and having a higher ACPS CD sub-score [RR = 1.03, 95% CI (1.01–1.05), p = 0.01] in childhood predicted a greater likelihood of a history of truancy at 8-year follow-up. Family income [RR = 0.95, 95% CI (0.93–0.98), p < 0.001] and being at site 2 [RR = 0.81, 95% CI (0.72–0.91), p < 0.001] in childhood predicted a lower likelihood of a history of truancy at 8-year follow-up.
The final combined model explained 11% of variance in truancy at 8-year follow-up. Table 2 depicts the results of the regression analysis. The sensitivity analysis, which additionally excluded CD-related variables at baseline (ACPS CD sub-score), explained 9.2% of the variance at 8-year follow-up.
Displays the significant baseline predictors of ADHD at 8-year follow-up through (1) truancy, (2) school punishment, and (3) in-school punishment. Stepwise logistic regression models are displayed.
Sites were not identified in NIMH limited-access datasets.
95% CI, 95% confidence interval; ACPS, Aggression and Conduct Problems Scale; ADHD, attention-deficit/hyperactivity disorder; APQ, Alabama Parenting Questionnaire; CBCL, Child Behavior Checklist; CD, conduct disorder; CPT, Continuous Performance Task; GAD, generalized anxiety disorder; PRQ, Parent/Child Relationship Questionniare; RR, risk ratio; SNAP, Swanson, Nolan and Pelham Questionnaire.
Figure 1 depicts the empirically derived hierarchal prognostic subgroups for truancy at 8-year follow-up. The overall truancy rate was 26.8%. The most discriminative predictor of truancy was the ACPS total score, with higher childhood scores being associated with an increased likelihood of truancy. An ROC analysis excluding CD variables is provided in Supplementary Data (Supplementary Data are available online at
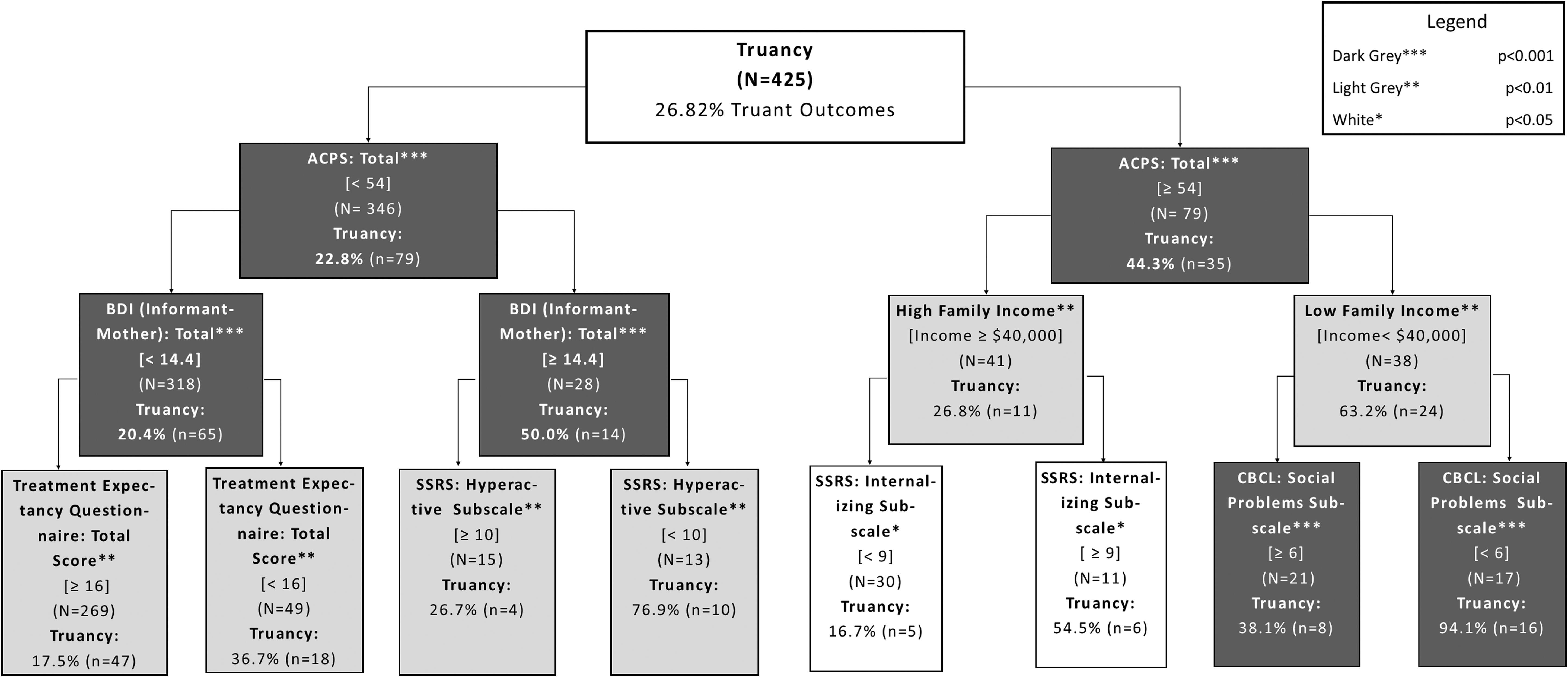
Empirically derived prognostic subgroups for truancy at 8-year follow-up in children with ADHD. This figure depicts hierarchical prognostic subgroups for the presence of truancy at 8-year follow-up in children with ADHD from the MTA cohort. Subjects were considered truant if their parents answered “yes” to “Did the child skip school or was the child truant during this interval (previous year)?” on the summary misbehaviors and justice contact variables in the yearly increments questionnaire. Boxes are shaded based on the p-value of discriminator in the analysis (dark gray/***p < 0.001; light gray/**p < 0.01; white/*p < 0.05). ACPS, Aggression and Conduct Problems Scale; ADHD, attention-deficit/hyperactivity disorder; BDI, Beck Depression Inventory of caregiver (typically mother); CBCL, Child Behavior Checklist; MTA, Multimodal Treatment Study of Children with ADHD; SSRS, Social Skills Rating System.
School discipline
Significant predictor variables in childhood that were associated with a history of school discipline eight years later were identified in five domains (demographic, trial factors, cognitive, comorbid psychotherapy, and parent-child relationship). In the final model, being male [RR = 1.25, 95% CI (1.04–1.50), p = 0.02], being African American [RR = 1.62, 95% CI (1.19–2.20), p = 0.002], and a higher PRQ parent-rated affection sub-score [RR = 1.18, 95% CI (1.03–1.35), p = 0.01] in childhood predicted a higher likelihood of a history of school discipline at 8-year follow-up. Family income [RR = 0.95, 95% CI (0.92–0.99), p = 0.008], being from site 1 [RR = 0.72, 95% CI (0.54–0.96), p = 0.02], site 2 [RR = 0.66, 95% CI (0.51–0.87), p = 0.003], site 3 [RR = 0.53, 95% CI (0.41–0.69), p = 0.001], or site 5 [RR = 0.69, 95% CI (0.53–0.89), p = 0.005] in childhood predicted a lower likelihood of a history of school discipline at 8-year follow-up.
Table 2 depicts the results of the regression analysis. The final combined model explained 12% of variance in-school discipline at 8-year follow-up. The results were unchanged in sensitivity analysis.
Figure 2 depicts the empirically derived hierarchal prognostic subgroups for school discipline at 8-year follow-up. The overall school discipline rate was 43.4%. Baseline clinical characteristics were able to identify subgroups with as low as a 22.9% likelihood of school discipline (family income ≥$50,000, parental knowledge of behavioral principles [50% correct] subscale of 0.5 or greater, and PRQ parent-rated deprivation of privileges subscale of 2.5 or greater) to as high as a 76.3% chance of discipline in school (family income <$50,000, APQ paternal involvement sub-score of <26.7, and SSRS social conduct sub-score <10). The most discriminative predictor of school discipline was family income. The results of ROC analysis were unchanged in sensitivity analysis.
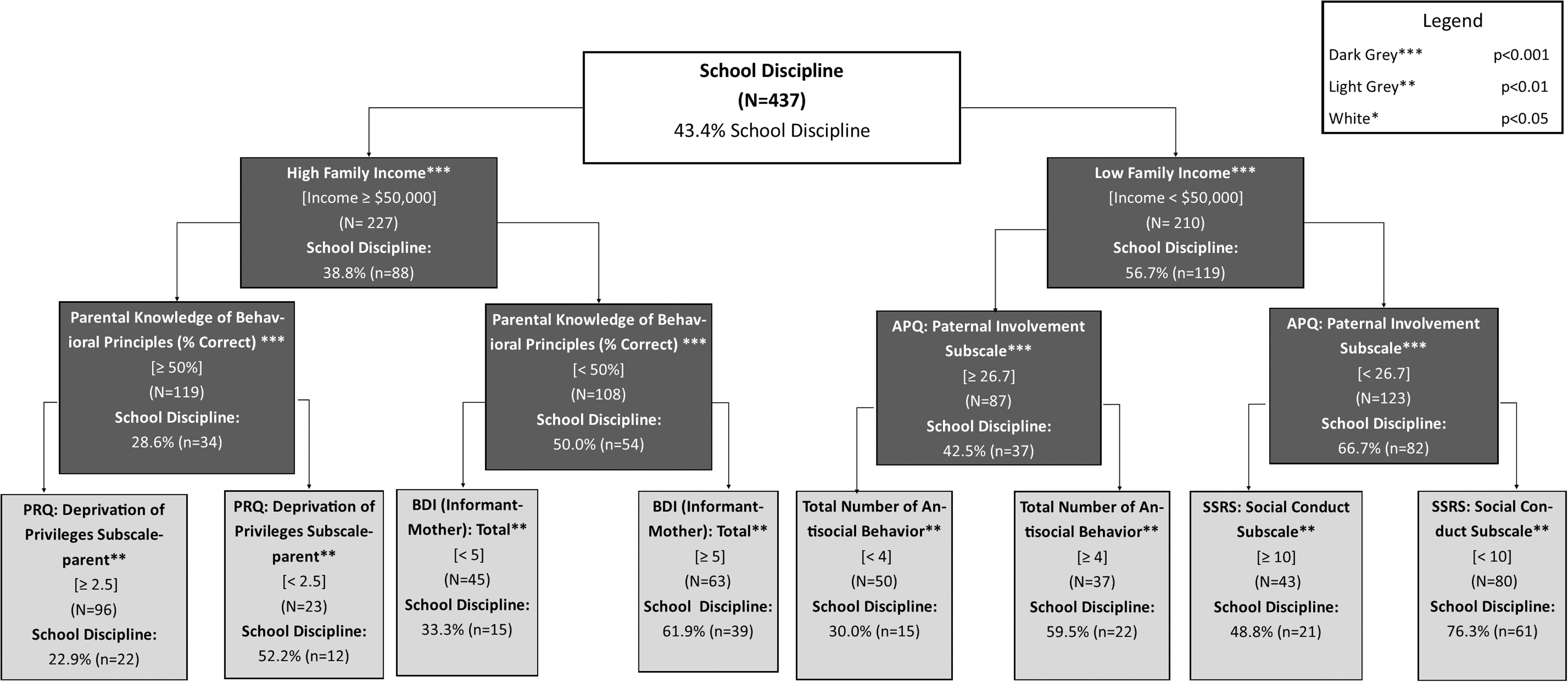
Empirically derived prognostic subgroups for school punishment at 8-year follow-up in children with ADHD. This figure depicts hierarchical prognostic subgroups for the presence of school punishment at 8-year follow-up in children with ADHD from the MTA cohort. Subjects were considered to have received punishment from school if their parents indicated that their child had received any of the following or if any of the following had occurred during the previous year: detention, suspension, expulsion, being sent home early for disciplinary reasons, or other school punishment on the summary misbehaviors and justice contact variables in the yearly increments questionnaire. Boxes are shaded based on the p-value of the discriminator in the analysis (dark gray/***p < 0.001; light gray/**p < 0.01; white/*p < 0.05). APQ, Alabama Parenting Questionnaire; ADHD, attention-deficit/hyperactivity disorder; BDI, Beck Depression Inventory of Caregiver (typically mother); MTA, Multimodal Treatment Study of Children with ADHD; PRQ, Parent/Child Relationship Questionnaire; SSRS, Social Skills Rating System.
In-school fights
Significant predictor variables in childhood that were associated with a history of in-school fights 8 years later were identified in 5 domains (demographic, family history, parental variables, parenting, and comorbid psychopathology). In the final model, being African American [RR = 1.41, 95% CI (1.18–1.69), p < 0.001] and having a higher SNAP ADHD subscale score [RR = 1.14, 95% CI (1.04–1.25), p = 0.005] predicted more in-school fights at 8-year follow-up. Table 2 depicts the results of regression analysis. The final combined model explained 8.1% of variance in in-school fights at 8-year follow-up. These results were unchanged in sensitivity analysis.
Figure 3 depicts the empirically derived hierarchal prognostic subgroups for in-school fights at 8-year follow-up. The overall prevalence of a history of in-school fights was 18.2%. Baseline clinical characteristics were able to identify subgroups with as low as a 9.5% likelihood of fights in school (not African American, MASC total <157 [less than high level of anxiety], and ACPS total of <24 [less than rarely]) to as high as a 69.7% chance of fights in school (African American, PRQ parent-rated physical punishment sub-score of 1.5 [not too much or more] or greater, and CBCL total of 48 [sometimes or more] or greater). The most discriminative predictor of in-school discipline was race. The most discriminative variable did not change in ROC sensitivity analysis. An ROC analysis excluding CD variables is provided in Supplementary Data.
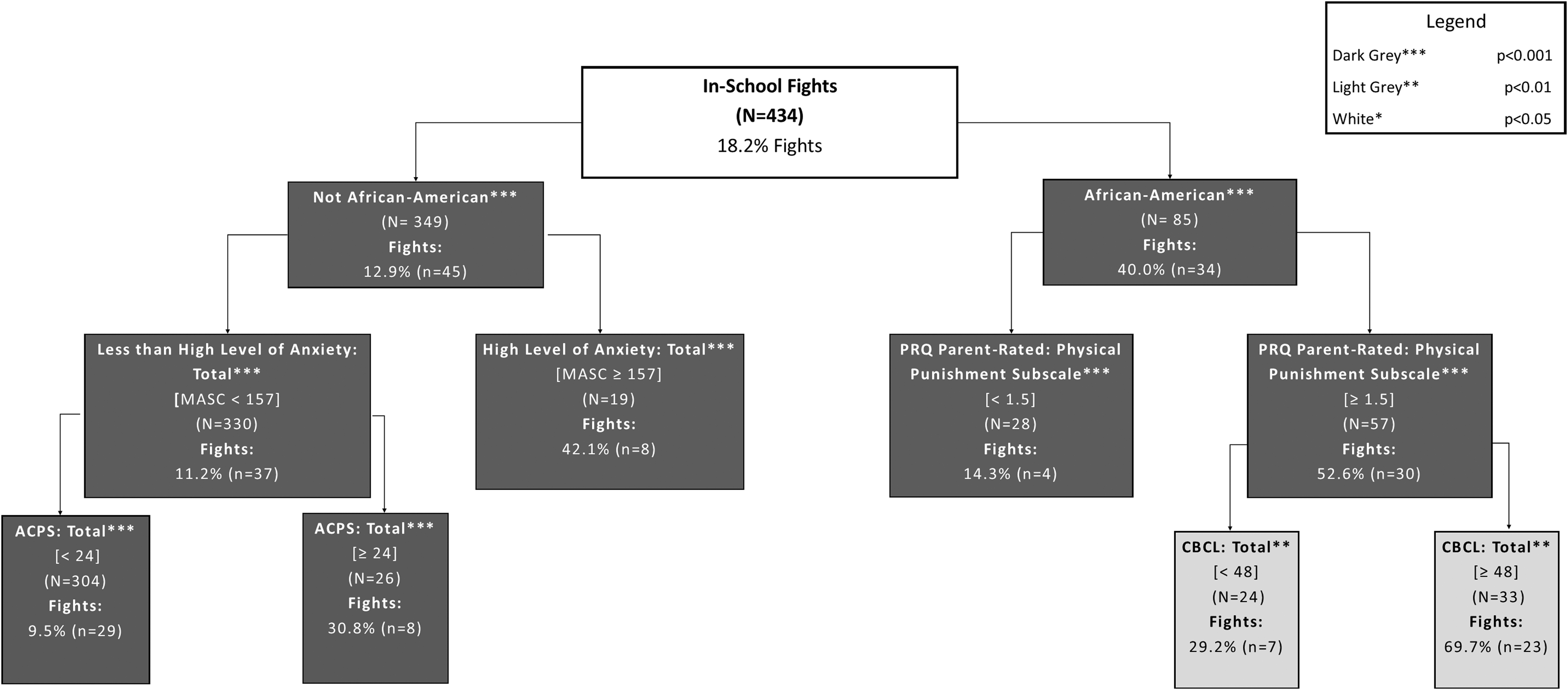
Empirically derived prognostic subgroups for in-school fights at 8-year follow-up in children with ADHD. This figure depicts hierarchical prognostic subgroups for the presence of in-school fights at 8-year follow-up in children with ADHD from the MTA cohort. Subjects were considered to have engaged in in-school fights if their parents indicated that their child had fought with either peers or teachers during the previous year on the summary misbehaviors and justice contact variables in the yearly increments questionnaire. Boxes are shaded based on the p-value of the discriminator in the analysis (dark gray/***p < 0.001; light gray/**p < 0.01; white/*p < 0.05). ACPS, Aggression and Conduct Problems Scale; ADHD, attention-deficit/hyperactivity disorder; CBCL, Child Behavior Checklist; MTA, Multimodal Treatment Study of Children with ADHD.
Discussion
A meaningful portion of school-based discipline outcomes during adolescence was predicted by baseline childhood characteristics. Exploratory regression analysis was able to explain 8.1%–12% of the variance in behavioral outcomes in school 8 years later. ROC analysis was able to identify empirically derived subgroups with 17%–94% chance of being truant, 23%–76% chance of receiving school discipline, and 10%–70% of engaging in a fight at school based on characteristics in childhood measured 8 years earlier. Exploratory analysis was able to identify modifiable (parental knowledge of behavioral principles, paternal involvement, and parental use of physical punishment), somewhat modifiable (having comorbid CD and family income), and nonmodifiable risk factors (sex and race) for future behavioral problems in school.
Nonmodifiable risk factors associated with school-based behavioral difficulties included being male and African American. Previous studies of children, in general, have shown that being male and African American is associated with a stronger likelihood of being suspended or expelled (Taylor and Foster 1986; Wallace et al. 2008; Aud et al. 2011). The agreement between the nonmodifiable risk factors associated with school-based behavioral difficulties identified within our current analysis in children with ADHD as compared with previous studies conducted in the general population suggests that the nonmodifiable risk factors identified may not be unique for children with ADHD.
Although race is considered a nonmodifiable risk factor, it remains quite possible that effective interventions could reduce the association between race and poor school-based behavioral outcomes. Past research has clearly demonstrated that race is not associated with antisocial behavior when socioeconomic status is controlled for in analysis (Loeber 1998). Skin color res ipse certainly has nothing to do with the association; this association is most likely related to bias toward African American students in distributing punishment or differing underlying characteristics of the school systems in general. In particular, interventions aimed toward desegregating neighborhoods and schools (poor African Americans are more than threefold times more likely to live in high poverty neighborhoods and failing school districts than poor whites), reducing income inequality, and reducing social biases might be effective in reducing race as a risk factor for school-related behavioral problems (Desimone 1999; Neblett et al. 2006; Jargowsky 2013).
Family income and having comorbid CD were recognized as somewhat modifiable risk factors. Previous studies suggest that children from low-income communities are more likely to receive disciplinary action at school (Atkins et al. 2002). The cause for the association between low family income and increased disciplinary action at school in this and other studies remains unclear. Some of the increased risk of school discipline may be related to problematic behavior on the part of the child. On the other hand, social bias may also be contributing to this association (e.g., children with ADHD from wealthy families may not be as likely to be punished or receive as severe punishments for given misbehavior as compared with children with ADHD from poorer families) (Kazdin 1995; Scott 2012; NCCMH et al., 2013).
In addition, increased psychosocial stressors related to poverty or structural barriers preventing improved school behavior (e.g., longer travel times to school, increased household responsibility, and concerns about safety) may also contribute to this association. Regardless of the underlying cause, formal studies are underway to examine the long-term effects of improving income (i.e., giving public housing vouchers to families in need) on childhood psychopathology and behavior (Feins et al. 1995, 1996; Orr et al. 2003). Although initial research has made clear that such interventions improve overall psychological distress and can effectively cause children to move to neighborhoods with lower poverty and crime rates and increased social ties with more affluent people, it remains unclear whether children of families benefiting from these programs experience improved long-term psychiatric outcomes or improved educational performance (Leventhal and Dupere 2011; Osypuk et al. 2012; Kessler et al. 2014).
CD in childhood was also associated with poorer school-based outcomes eight years later (particularly truancy and school fights). Truancy and participation in physical fights represent two criteria for the diagnosis of CD. Our results suggest that initial CD problems in children with ADHD are associated with continued truancy and school fights even eight years later during adolescence. Research has demonstrated that there are several system-based or family-based inventions that are effective in reducing symptoms of CD, including multisystemic therapy, functional family therapy, multidimensional treatment foster care, and parent-training programs (Brestan and Eyberg 1998; Henggeler and Sheidow 2012). Targeting children with ADHD and CD problems may be particularly important in reducing adverse school-based behavioral outcomes.
We further provide sensitivity analysis in the Supplementary Data if these childhood CD symptoms are excluded as predictor variables in analysis (as including ratings of CD symptoms to predict CD-related outcomes such as truancy, school fights may appear somewhat circular). Excluding CD variables in sensitivity analysis resulted in a slight reduction in the percent of variance explained for 1 out of 3 logistic regression models related to truancy (from 11% to 9.2%) and predictably led to a significant change in an ROC model of truancy where parental knowledge of behavioral principles (replaced ACPS total score) is the most discriminative predictor of outcome. However, the stability of childhood CD symptoms for predicting adverse school-related behavioral outcomes associated with CD symptoms is clinically relevant for identifying at-risk children for these behaviors in adolescence.
Exploratory analysis also identified several modifiable risk factors for future school behavioral problems. These modifiable risk factors at childhood baseline assessment include lower paternal involvement, parental knowledge of behavioral principles, and higher parental use of physical punishment. Our findings complement a prior study exhibiting the correlation of high paternal involvement and low discipline problems in school (Hinshaw et al. 2000; Pettit et al. 2001). Our study expands on this previous research by demonstrating that low paternal involvement is associated with a high risk of school discipline, specifically for students with ADHD.
Similarly, a previous study demonstrated that an increase in parental knowledge of behavioral principles is associated with less discipline at school of children with ADHD (Long et al. 1993). Previous studies have also established that children without ADHD who receive physical punishment at home, such as spanking, were more likely to engage in fights at school, even as early as kindergarten (Strassberg et al. 1994).
In addition, ROC analysis demonstrated potentially important interactions between modifiable and unmodifiable risk factors. That is, the ROC analysis for school discipline identified greater parental knowledge of behavioral principles as a protective factor in high-income families (≥$50,000). By contrast, greater paternal involvement was a protective factor in low-income families (<$50,000) for the same outcome. These results suggest that interventions increasing parental knowledge of behavioral principles in middle-class families may be an effective intervention; whereas in lower-income families, interventions designed to increase paternal involvement in a child's life may be most effective. Of course, any intervention targeting increased paternal involvement in low-income families must also target structural economic barriers to increase parent-child interaction.
Increased implementation of physical punishment by parents was associated with a twofold greater likelihood of engaging in fights at school. Similarly, ROC analysis demonstrated that use of any physical punishment by parents was associated with a 3.5-fold higher risk of children engaging in fights at school 8 years later. In addition, prior studies have demonstrated that children who experienced physical punishment from their parents had a greater chance of participating in fights at school (Larzelere 2000). It should be noted that our study cannot definitively demonstrate causality, as it remains possible that increased parental physical punishment in childhood may represent a reaction to increased antisocial psychopathology of the child rather than directly causing these later outcomes.
This analysis is limited in that results were obtained empirically and were not hypothesis driven. We conducted a large number of statistical tests without statistical correction for multiple hypothesis testing. However, we used exploratory analysis approaches, such as ROC analysis and Fournier regression techniques, that at least minimize the problems with multiple hypothesis testing. Nonetheless, given the exploratory nature of our analysis, significant findings in our article need replication in future studies. The original MTA was powered to detect clinically significant differences between treatment groups (an effect size of 0.4 with 80% power at α = 0.05) and not to detect predictors of long-term school behavioral outcomes. Therefore, there is a possibility that some strong predictors of the long-term school behavioral outcome were not identified.
In addition, the outcomes utilized for school-based behavioral outcomes, although clinically meaningful, have never been assessed for validity, reliability, or consistency in reporting. All outcomes were based on parent reporting of adolescents' behavior, rather than on actual data from schools regarding truancy, in-school discipline, or altercations, which would be more accurate. Data of school-based behavioral outcomes were unavailable for some participants in the initial MTA, and participants and nonparticipants at 8-year follow-up differed in several characteristics at baseline. Several of these differences in baseline were actually identified as strong predictors of school-based behavioral outcomes.
In general, the follow-up cohort in the MTA is likely not representative of the baseline MTA cohort, and the participants lost to follow-up likely had a worse prognosis in terms of school-based behavioral outcomes. This limitation should not affect the internal validity of the results, but it may affect the generalizability of the results to a representative sample.
A modest, but nontrivial proportion of school behavioral outcomes can be predicted by baseline childhood characteristics eight years earlier in children with ADHD. Several nonmodifiable risk factors, such as race and sex, and somewhat modifiable risk factors, such as income, were associated with school behavioral outcomes. In addition, several potentially modifiable risk factors such as paternal involvement, parental knowledge of behavioral principles, and parental use of physical punishment were identified. These potentially modifiable risk factors could serve as a basis for interventions that are designed to improve in-school behavioral outcomes for high-risk children.
Clinical Significance
Children with ADHD experience higher rates of truancy, school discipline, and in-school fights compared with the general population. Identifying predictors of school-based behavioral outcomes may help to detect children who are at a high risk of experiencing difficulties in school. Using exploratory analysis techniques (i.e., not hypothesis driven), we were able to identify modifiable (lack of paternal involvement, lower parental knowledge of behavioral principles, and parental use of physical punishment), somewhat modifiable (family income and having comorbid CD), and nonmodifiable (African American and male) risk factors associated with school-based behavioral outcomes.
Footnotes
Acknowledgments
Data used in the preparation of this article were obtained from the limited access datasets distributed from the National Institute of Health (NIH) supported “Multimodal Treatment Study of Children with Attention-Deficit/Hyperactivity Disorder” (MTA). This is a multisite, clinical trial and a long-term follow-up study of children with attention-deficit/hyperactivity disorder who were randomly assigned to one of four treatment modalities. The study was conducted by the MTA Cooperative Group and supported by the National Institute of Mental Health (NIMH), with funds also contributed by the National Institute on Drug Abuse (NIDA), the Department of Justice, and the Department of Education. The MTA study has been supported by the following grant numbers: U01MH50440, U01MH50447, U01MH50453, U01MH50454, U01MH50461, and U01MH50467; and the following contract numbers: N01MH12004, N01MH12007, N01MH12008, N01MH12009, N01MH12010, N01MH12011, N01MH12012; HHSN271200800003-C, HHSN271200800004-C, HHSN271200800005-C HHSN271200800006-C, HHSN271200800007-C, HHSN271200800008-C, and HHSN271200800009-C. The
Disclosures
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.