
Abstract
Objective:
This is an investigation of minocycline efficacy and safety as an adjuvant to risperidone in management of children with autism.
Methods:
Forty-six children with diagnosis of autistic disorder, according to the Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) criteria and a score of ≥12 on the Aberrant Behavior Checklist-Community (ABC-C) irritability subscale, who were already drug-free for at least 6 months participated in a randomized controlled trial and underwent 10 weeks of treatment with either minocycline (50 mg twice per day) or placebo in addition to risperidone titrated up to 2 mg/day (based on bodyweight). Patients were evaluated using ABC-C at baseline and at weeks 5 and 10.
Results:
General linear model repeated measures showed significant effect for time × treatment interaction on the irritability [F(2, 88) = 3.94, p = 0.02] and hyperactivity/noncompliance [F(1.50, 66.05) = 7.92, p = 0.002], but not for lethargy/social withdrawal [F(1.61, 71.02) = 0.98, p = 0.36], stereotypic behavior [F(1.34, 58.80) = 1.55, p = 0.22], and inappropriate speech subscale scores [F(1.52, 66.88) = 1.15, p = 0.31]. By week 10, 21 (91.3%) patients in the minocycline group and 15 (65.5%) patients in the placebo group achieved at least partial response (p = 0.03). Frequencies of adverse events were not significantly different between groups.
Conclusions:
Minocycline seems to be a safe and effective adjuvant in management of patients with autistic disorder. Future studies with larger sample sizes, longer follow-ups, and inflammatory cytokine measurements are warranted to confirm these findings and provide insight into minocycline mechanism of action in autistic disorder.
Introduction
A
In recent years, a growing number of studies have found evidence implicating dysregulation of immune responses and neuroinflammatory mechanisms in patients with ASD (Chaste and Leboyer 2012). Dysregulation of T helper cells (Gupta et al. 1998), increased plasma levels of proinflammatory cytokines such as interleukin 1, 6, and 8 (Jyonouchi et al. 2001; Ashwood et al. 2011), increased proliferation and activation of B cells and natural killer cells (Ashwood et al. 2011), decreased serum levels of immunoglobulin G and M (Heuer et al. 2008) in the presence of immunoglobulin G autoantibodies against neuron-axon filament and glial fibrillary acidic proteins (Singh et al. 1997), and increased microglial and astrocytic density and activation (Vargas et al. 2005; Morgan et al. 2010) have been documented.
Currently, behavioral therapy is considered to be the method of choice in treatment of patients with ASD even though it is only partially effective in most cases (Towbin 2003). When significant dysfunction exists, despite appropriate behavioral therapy, or when a patient achieves only suboptimal improvements, a trial of pharmacotherapy is recommended, mainly to manage the specific symptoms of ASD (Myers et al. 2007). Even though increase in knowledge of ASD etiopathogenesis has resulted in new opportunities for employment of more effective agents with greater safety, there still are a limited number of double-blind placebo-controlled studies in this field of research (Aman et al. 2008).
Several studies have shown the beneficial neuroprotective effects of minocycline, a broad spectrum tetracycline antibiotic, which easily crosses the blood–brain barrier (Elewa et al. 2006; Stolp et al. 2007; Schildknecht et al. 2011). Minocycline has shown promising results in patients with several psychological disorders such as depression (Miyaoka et al. 2012), schizophrenia (Miyaoka et al. 2008; Khodaie-Ardakani et al. 2014), and Parkinson's disease (NINDS NET-PD Investigators 2006, 2008), as well as animal models of Huntington's disease (Chen et al. 2000) and amyotrophic lateral sclerosis (Zhang et al. 2003). Beneficial effects of minocycline in these disorders seem to be mostly attributed to its anti-inflammatory effects on the central nervous system. Hence, this agent may be a suitable candidate in management of ASD by inhibiting the probable underlying neuroinflammatory mechanisms.
Fragile X syndrome (FXS) is a genetic disorder characterized mainly by intellectual disabilities. FXS shares many neurological and molecular features with ASD, and it has been estimated that about 30% of patients with FXS also suffer from autism (Harris et al. 2008). Thus, it has been suggested that effective pharmacotherapeutic modalities in the management of FXS may also benefit patients with ASD by modulating the overlapping mechanisms involved in the etiopathogenesis of these two disorders (Wang et al. 2010). Interestingly, both animal studies on the FXS rat model (Bilousova et al. 2009) and clinical trials on patients with FXS have shown minocycline to be effective and safe in improving behavioral function (Paribello et al. 2010; Leigh et al. 2013).
Recently, Pardo et al. (2013) investigated the efficacy of minocycline in an open-label trial on 10 children with ASD. Even though the authors observed only minimal improvements in some of their patients, the lack of positive findings may be attributed to their small sample size. Moreover, the Pardo et al. study specifically focused on children with ASD of the regressive subtype. This also may have contributed to their lack of positive findings. To the best of our knowledge, efficacy of minocycline in management of ASD has been previously evaluated only in the aforementioned study (Pardo et al. 2013). Based on the currently available body of evidence, we designed a randomized, double-blind placebo-controlled trial to investigate the safety and efficacy of minocycline as an add-on therapy to risperidone in reducing severity of different categories of ASD symptoms.
Methods
Trial design and study settings
This 10-week, randomized, parallel group, double-blind placebo-controlled trial was carried out at the specialty clinic for autism in the children's outpatient clinic of Roozbeh University Hospital affiliated with Tehran University of Medical Sciences (TUMS), Tehran, Iran, from March 2013 to March 2015. The study protocol was reviewed and approved by the Institutional Review Board (IRB) of TUMS (Code No. 20288). The trial was performed in accordance with the Declaration of Helsinki and its subsequent revisions. Written informed consents were obtained from the parents or the legal guardians of the children before entering the children into this trial and the children provided assent. This trial is registered with the Iranian Clinical Trials Registry (IRCT Registration No. IRCT201302201556N50;
Participants
The study population included children within the age range of 4–12 years who met the criteria for the diagnosis of autism with an Aberrant Behavior Checklist-Community (ABC-C) Irritability subscale score of ≥12. At least six of the DSM-IV-TR criteria were required for making the diagnosis of autism. Before entering the study, each child was assessed for the diagnosis of autism according to the criteria defined by the Diagnostic and Statistical Manual of the American Psychiatric Association. The diagnosis of autism was confirmed by a child psychiatrist through behavioral observations of the child and a semistructured interview with the parents. Further confirmation of the diagnosis was made using the Autism Diagnostic Interview revised by a second experienced child psychiatrist (Lord et al. 1994).
Children with concomitant psychotic disorders, severe intellectual disability that made the diagnosis inconclusive (based on clinical judgment and reviewing prior neurocognitive testing and records), other DSM-IV axis I or II disorders, seizure disorder, a history of alcohol or drug abuse, tardive dyskinesia, administration of antipsychotic medications within the past 6 months, as well as behavior therapy, and the presence of any significant active medical condition were excluded from the study. Since discontinuation of treatment to make the patients drug-free before this study was not possible due to ethical concerns raised by the IRB, we included patients who were already drug-free for at least 6 months due to other reasons (such as discontinuation of the treatment by parents). All screened patients underwent a thorough clinical and laboratory examination to test for liver disease.
Intervention
Eligible participants were randomly assigned to receive either minocycline (Ebixa; Lundbeck A/S) plus risperidone (Risperdal; Janssen Pharmaceuticals) or placebo plus risperidone for 10 weeks. Both drugs (minocycline/placebo and risperidone) were started simultaneously. Risperidone (0.5 mg tablets) was started at a dose of 0.5 mg/day, then increased by 0.5 mg per week in the absence of clinically significant adverse effects. The maximum target dose of risperidone was defined as 1 mg/day for patients weighing less than 20 kg and 2 mg/day for those weighing equal or more than 20 kg. Participants received a 50 mg minocycline capsule twice per day or placebo capsule twice per day. No other medical therapies and no psychosocial therapies were allowed for the participants during the clinical trial.
Outcome
Treatment efficacy was measured by the ABC-C rating scale (Aman et al. 1985). ABC-C is a 58-item tool to evaluate the existence and severity of disruptive behaviors. Five types of behavioral abnormalities are assessed by this tool, three of which address the core deficits of autism, including lethargy/social withdrawal, stereotypic behavior, and inappropriate speech, while the other items evaluate the associated disturbances (irritability and hyperactivity/noncompliance). The ABC-C rating scale has already been used in several studies in the Iranian population (Asadabadi et al. 2013; Ghaleiha et al. 2013a, 2013b; Mohammadi et al. 2013; Ghaleiha et al. 2015; Nikoo et al. 2015).
Each child was rated at baseline and at weeks 5 and 10 (endpoints) by the ABC-C rating scale. Following standardized instructions, an independent rater asked parents to complete the ABC-C rating scale. The mean change in the ABC-C irritability subscale score from baseline to trial end was used as the main outcome measure. Two groups were also compared regarding the partial response (≥25% reduction in irritability subscale score) or complete response (≥50% reduction in irritability subscale score) at the end of the study. The mean changes in the other four ABC subscales were considered as secondary outcomes. Extrapyramidal symptoms were assessed using the Extrapyramidal Symptoms Rating Scale (ESRS) (Chouinard and Margolese 2005), which has been applied in several trials in Iran (Zeinoddini et al. 2014).
Randomization, allocation concealment, and blinding
Patients were randomized to receive either minocycline or placebo in a 1:1 ratio using a computer-generated code. The assignments were kept in sealed opaque envelopes until data analysis. Placebo was identical to the intervention medication (minocycline) in shape, size, color, and taste and was dispensed by the investigational drug pharmacist. Throughout the study, the person who administered the medications, the rater, the patients, and parents were blind to assignments. Independent persons were responsible for treatment allocation and patient interviews.
Adverse events
Parents were asked to immediately inform the research team about any unexpected symptoms in their child following study enrollment. Adverse events were checked by a phone call 1 week after initiation of therapy. Adverse events were also recorded at each visit using open-ended questioning, followed by a complete adverse events checklist (a 25-item checklist covering a broad range of adverse events). In addition, patients were visited at week 2 for evaluation of adverse events (at home). Entries were based on responses from parents. Furthermore, there was a particular concern regarding tooth discoloration at each visit. The behavior appraisals and adverse events were completed by different raters. ESRS was used at each visit to assess extrapyramidal adverse events.
Sample size
A sample size of 46 was calculated (23 in each group) assuming a final difference of 4 on the ABC-C irritability subscale score between the two groups with a standard deviation (SD) of 4, type I error of 0.05, and power of 90%. Considering an attrition rate of 10%, a final sample size of 50 was needed (25 in each group).
Statistical analyses
The mean ± SD of continuous variables and frequency of categorical variable are reported. The mean difference (MD) between the two groups is reported as MD (95% confidence interval [CI]). Baseline continuous variables were compared between groups using the independent t-test. Categorical variables were analyzed using chi square or Fisher's exact test as indicated. Independent t-test and Cohen's d effect size were used to compare score change from the baseline to each time point between treatment groups. General linear model repeated measure was used to compare ABC-C subscale scores and ESRS scores between treatment groups during the study course. Whenever Mauchly's test of sphericity was significant, Greenhouse–Geisser correction was used for degrees of freedom. Kaplan–Meier estimation with log-rank test was used to compare the time needed to partially respond to the treatment between the two groups. All analyses were two-sided, and a p value of less than 0.05 was considered to be significant. Statistical analysis was performed using Statistical Package of Social Science Software (SPSS version 20; IBM Company). Sigma plot (version 12) was used to draw the graphs of repeated measure tests.
Results
Participants and baseline characteristics
A total of 50 children were enrolled into the trial and randomized to receive either minocycline (n = 25) or placebo (n = 25). In each group, two children withdrew their consent before week 5. Twenty-three patients completed the study in each group and participated in all visits (Fig. 1). Baseline characteristics of the patients as well as their ABC-C subscale scores and ESRS scores did not differ significantly between treatment groups, as summarized in Table 1. The mean dose of risperidone administered throughout the study was 1.41 ± 0.55 mg/day in the minocycline group and 1.38 ± 0.58 mg/dL in the placebo group, respectively (p = 0.84).
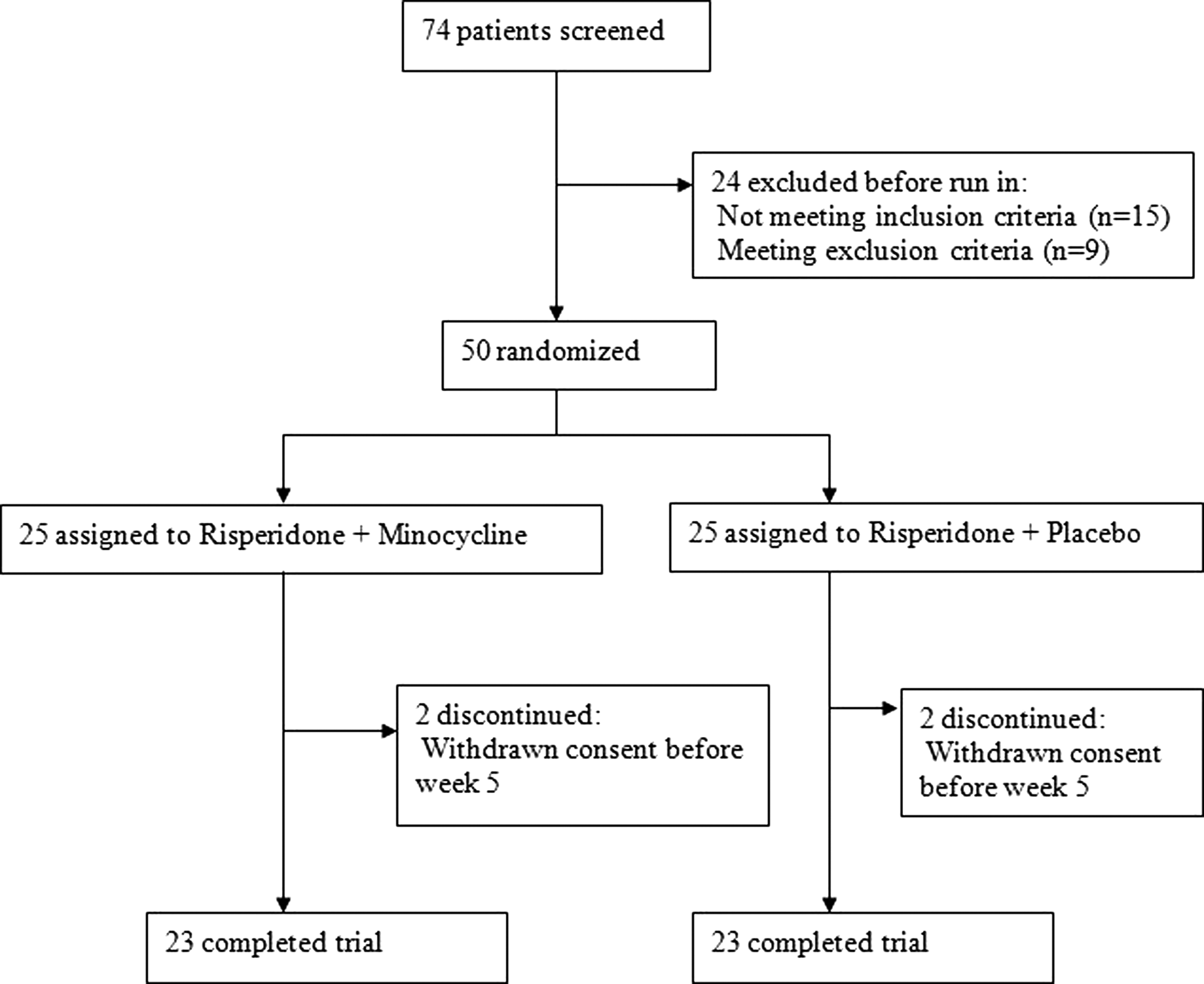
Flow diagram of the study.
SD, standard deviation.
Outcome
Irritability subscale
Baseline irritability subscale scores were not significantly different between the two groups [MD (95% CI) = 1.35 (−2.31 to 5.01), t (38.43) = 0.74, p = 0.46]. General linear model repeated measures demonstrated significant effect for time × treatment interaction on irritability subscale scores [F(2.00, 88.00) = 3.94, p = 0.02] (Fig. 2). Significantly greater score reduction in the irritability subscale occurred in the minocycline group compared with the placebo group at week 10 [MD (95% CI) = 3.30 (1.15–5.46), t (44) = 3.09, p = 0.003] (Table 2). By week 10, 21 (91.3%) patients in the minocycline group and 15 (65.5%) patients in the placebo group achieved at least partial response (p = 0.03). Greater complete response rate (more than twofold) was observed in the minocycline group (n = 7, 30.4%) than the placebo group patients (n = 3, 13.0%). Nevertheless, the difference did not reach statistical significance (p = 0.15), probably due to the small sample size and insufficient power to detect a difference (power = 29.4%). Kaplan–Meier estimation indicated that a shorter time was needed in the minocycline group than the placebo group for partial response to the treatment (p = 0.047).
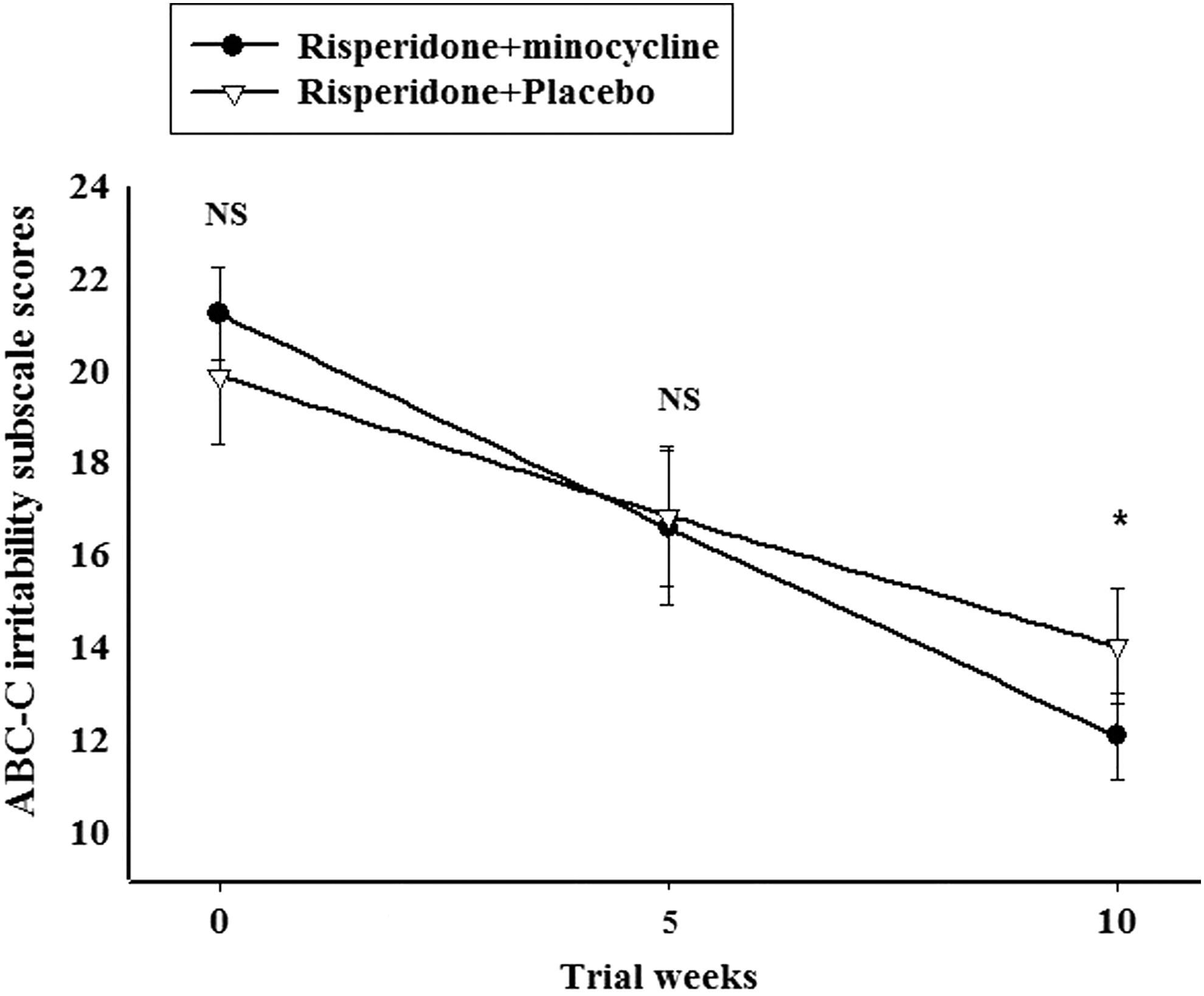
Repeated measure graph for comparison of Aberrant Behavior Checklist-Community (ABC-C) irritability subscale scores (mean ± standard error of the mean [SEM]) over time between the minocycline group and the placebo group, *p < 0.05; nonsignificant (NS) (p ≥ 0.05). p Values represent results of independent t-test for comparison of changes from baseline to each time between the two groups.
The p value and Cohen's d represent results of independent t-test for comparison of changes from baseline to week 10 between the two groups.
ABC-C, Aberrant Behavior Checklist-Community; SD, standard deviation.
Lethargy/social withdrawal subscale
Baseline lethargy/social withdrawal subscale scores were not significantly different between the two groups [MD (95% CI) = 1.09 (−3.52 to 5.69), t (44) = 0.48, p = 0.64]. Using general linear model repeated measures, no significant effect was observed for time × treatment interaction on lethargy/social withdrawal subscale scores [F(1.61, 71.02) = 0.98, p = 0.36]. Score reduction in the lethargy/social withdrawal subscale was not significantly different between the minocycline group and the placebo group by week 10 [MD (95% CI) = 0.91 (−1.57 to 4.00), t (44) = 0.76, p = 0.46] (Table 2).
Stereotypic behavior subscale
Baseline stereotypic behavior subscale scores were not significantly different between the two groups [MD (95% CI) = −0.13 (−3.11 to 2.84), t (44) = −0.09, p = 0.93]. Using general linear model repeated measures, no significant effect was observed for time × treatment interaction on stereotypic behavior subscale scores [F(1.34, 58.80) = 1.55, p = 0.22]. Score reduction in the stereotypic behavior subscale was not significantly different between the minocycline group and the placebo group by week 10 [MD (95% CI) = 1.08 (−0.68 to 2.86), t (44) = 1.23, p = 0.22] (Table 2).
Hyperactivity/noncompliance subscale
Baseline hyperactivity/noncompliance subscale scores were not significantly different between the two groups [MD (95% CI) = 3.17 (−1.40 to 7.75), t (38.12) = 1.40, p = 0.17]. General linear model repeated measures demonstrated significant effect for time × treatment interaction on hyperactivity/noncompliance subscale scores [F(1.50, 66.05) = 7.92, p = 0.002]. Significantly greater score reduction in the hyperactivity/noncompliance subscale occurred in the minocycline group compared with the placebo group at week 10 [MD (95% CI) = 4.78 (1.80–7.70), t (44) = 3.23, p = 0.002] (Table 2).
Inappropriate speech subscale
Baseline inappropriate speech subscale scores were not significantly different between the two groups [MD (95% CI) = 1.13 (−0.83 to 3.09), t (44) = 1.16, p = 0.25]. Using general linear model repeated measures, no significant effect was observed for time × treatment interaction on inappropriate speech subscale scores [F(1.52, 66.88) = 1.15, p = 0.31]. Score reduction in the inappropriate speech subscale was not significantly different between the minocycline group and the placebo group by week 10 [MD (95% CI) = 0.56 (−0.40 to 1.53), t (44) = 1.18, p = 0.24] (Table 2).
Extrapyramidal symptoms rating scale
ESRS scores did not differ significantly between the two groups at baseline [MD (95% CI) = −0.04 (−0.23 to 0.15), t (44) = −0.46, p = 0.64] and at study endpoint [MD (95% CI) = −0.09 (−0.29 to 0.12), t (44) = −0.86, p = 0.08]. No significant effect was observed for time × treatment interaction using general linear model repeated measures [F(1.75, 76.99) = 0.12, p = 0.86]. The difference between treatment groups in the score change from baseline to the endpoint was not significant [MD (95% CI) = 0.04 (−0.19 to 0.28), t (44) = 0.37, p = 0.71].
Adverse events
The frequencies of adverse events observed during the trial period are summarized in Table 3. There was no significant difference between the two treatment groups. No serious adverse events and no deaths were observed.
Discussion
This study provides evidence in support of short-term beneficial effects of minocycline in patients with ASD. Minocycline improved patient symptoms in subscales of irritability and hyperactivity/noncompliance, while no improvements were observed in subscales of lethargy/social withdrawal, stereotypic behavior, and inappropriate speech. Compared with the placebo, minocycline was well tolerated and did not result in significant increase in incidence of side effects. Since personal and clinical characteristics of patients did not differ between the two groups at the study commencement, effects of minocycline cannot be attributed to random differences in subject characteristics. The observed beneficial effects of minocycline on ASD symptoms in the current study could potentially be attributed to its immunomodulatory and anti-inflammatory characteristics. In line with this hypothesis, several studies have investigated the administration of agents with immunomodulatory and anti-inflammatory effects in ASD with promising results. These agents include celecoxib, a cyclooxygenase-2 inhibitor (Asadabadi et al. 2013); pioglitazone, a thiazolidinedione (Boris et al. 2007); piracetam, a nootropic drug with antioxidant and neuroprotective effects (Akhondzadeh et al. 2008); pentoxifylline, a methylxanthine phosphodiesterase inhibitor (Akhondzadeh et al. 2010); ginkgo biloba, a herbal drug with antioxidant and anti-inflammatory characteristics (Hasanzadeh et al. 2012); and topiramate, an antiepileptic agent (Rezaei et al. 2010).
In this study, we hypothesized that immunomodulatory and anti-inflammatory characteristics of minocycline are the main contributing factors to its beneficial effects in ASD. In line with this hypothesis, previous studies have reported such effects for this agent through several pathways. In one study, Carty et al. (2008) reported a significant decline in neuroinflammation following the administration of minocycline in a rat model of brain injury caused by hypoxia–ischemia. In another study, Suk (2004) reported that minocycline inhibits microglia activation in a rodent model of cerebral ischemia. Moreover, Jin et al. (2014) reported that minocycline also inhibits astrocytic activation accompanied by a significant improvement of cognitive symptoms in a murine model. Interestingly, increased microglial and astrocytic activation are both known to be involved in the etiopathogenesis of ASD (Vargas et al. 2005; Morgan et al. 2010).
Another possible minocycline mechanism of action in ASD could be through regulation of matrix metalloproteinase-9 (MMP-9). MMP-9 is a zinc metalloproteinase enzyme that is responsible for extracellular matrix degradation. In the human brain, MMP-9 is known to be involved in synaptic plasticity and learning processes (Ganguly et al. 2013). Increased levels of MMP-9 are known to be associated with neuroinflammation and neurodegeneration (Kaplan et al. 2014). Interestingly, one study showed an increased level of MMP-9 in patients with ASD (Abdallah et al. 2012). Furthermore, minocycline has been shown to decrease MMP-9 levels, particularly in FXS, a disorder with presumed mechanistic similarities with ASD, which was also accompanied by improvements in symptoms of disease in some cases (Dziembowska et al. 2013). Another suspected mechanism in the etiopathogenesis of ASD (Gupta et al. 1998) is based on the fact that a decreased serum level of MMP-9 is also reported to inhibit the activation and migration of T helper cells to the brain (Brundula et al. 2002).
Another possible explanation for the observed beneficial effects of minocycline could be its role in the regulating N-methyl-
In the present study, daily administration of 100 mg minocycline (50 mg BID) appeared to be safe and well tolerated. Moreover, none of the patients withdrew from this study due to adverse effects of minocycline. These findings are in line with a previous study by Grieco et al. (2014) who also reported the safety and tolerability of minocycline in this age group using a similar dosage of minocycline in children aged 4–12 years.
The current study provides a valid evaluation of the beneficial effects of minocycline as an adjuvant therapy to risperidone in the management of patients with ASD. However, some limitations should be addressed to avoid overgeneralization of study results. The first limitation in this study is the relatively short follow-up period. Since ASD is chronic in nature, longer studies should provide more insight into the overall effect of minocycline in the clinical course of these disorders. Second, the lack of improvement in some of the subscales of ASD and significant differences in the incidence of side effects between the two groups could be due to the relatively small sample size of the study. Third, since the observed effects of minocycline on patients with ASD are potentially attributed to its immunomodulatory activity, it would be ideal to measure immune marker levels at baseline and during the follow-up period. Finally, it should be noted that the use of tetracycline antibiotics, including minocycline, could result in tooth discoloration if given during the period of tooth mineralization in childhood and this may limit its application.
Conclusions
Minocycline seems to be a safe and effective agent as an adjuvant in the management of patients with ASD. Future studies with larger sample sizes, longer follow-up durations, and inflammatory cytokine measurements are warranted to confirm these findings and provide insight into minocycline mechanism of action in ASD.
Clinical Significance
This is the first randomized placebo-controlled trial evaluating the beneficial effects of minocycline in children with ASD. Results from this trial indicate that minocycline is a tolerable and effective adjuvant therapy in ASD subjects aged 4–12 years.
Footnotes
Acknowledgments
This study was Dr. Rosa Alikhani's postgraduate thesis toward the Iranian Board of Psychiatry and supported by a grant from Tehran University of Medical Sciences to Prof. Shahin Akhondzadeh (Grant No. 20288). The funding organization had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript and the decision to submit the article for publication.
Disclosures
The authors also affirm that there was no source of funding; none of the authors have direct or indirect commercial/financial incentive associating with publishing the article, and no funding agreement limits their ability to complete and publish the study. In addition, the authors do not have any conflicts of interest.