
Abstract
Objectives:
Adolescents with major depressive disorder (MDD) were found to have deficits in executive function, attention, and memory. Despite the fact that some neurocognitive functions have been shown to be present in acute stage of the illness, but not in remission, longitudinal studies are lacking. The current study aimed to investigate the changes in neurocognitive functioning in adolescents with depression during an acute treatment course with selective serotonin reuptake inhibitor.
Methods:
Twenty-four adolescents with current MDD and 24 healthy controls (HCs) were administered subtests of the Cambridge Neuropsychological Test Automated Battery as well as clinical scales at baseline and were retested at weeks 6 and 12. Those with MDD were started on fluoxetine after the baseline assessment.
Results:
Despite considerable improvement in depressive symptoms in the MDD group, there was a persistent deficit in visual memory in the MDD group over time compared with HCs (p = 0.001). On a task of sustained attention and inhibition, HCs became better at detecting target sequences at week 12 while there were residual sustained attention deficits in MDD (p = 0.01). On an executive function (planning) task, while HCs learned the task and improved substantially in performance over 12 weeks, MDD performance did not significantly change (p = 0.04).
Conclusion:
When treating depressed adolescents, clinicians need to also monitor cognitive symptoms as they appear to lag behind mood symptoms in improvement.
Introduction
M
Adolescents with depression have performed more poorly on the Complex Attention Domain of the Central Nervous System Vital Signs computerized test battery, including sustained attention, shifting, and inhibition (Brooks et al. 2010; Baune et al. 2012), than healthy controls (HCs). These difficulties in switching attention in addition to increased processing speed in adolescents with current depression, as well as possible deficits in selective and sustained attention, were found in some (Wilkinson and Goodyer 2006) but not all studies (Maalouf et al. 2011).
Findings on inhibition and impulsivity in adolescents with depression have been more inconsistent. Some studies have shown that children and adolescents with depression do not show a pronounced deficit in inhibition on neuropsychological testing (Cataldo et al. 2005; van der Meere et al. 2011), despite the fact that they exhibit impulsive behavior (Cataldo et al. 2005). When stimuli have an emotional valence, however, cognitive control seems to be consistently compromised. Ladouceur et al. (2006) showed that children and adolescents with affective disorders showed impaired responses to sad facial expressions on a Go/No-Go task requiring cognitive control. Maalouf et al. (2012) found attention bias to emotionally salient stimuli with negative valence only in adolescents with acute MDD, and not in those in remission, suggesting that this impaired inhibition is a state and not a trait marker of adolescent depression.
There have been many studies, primarily in the adult population, investigating the presence of cognitive dysfunctions in acute versus remitted states of depression (Biringer et al. 2005; Castaneda et al. 2008). Neurocognitive functions that show impairment in the acute stages of MDD but return to normal after remission are state markers of depression and thought to reflect treatment response and good prognosis. In contrast, trait markers are dysfunctions that persist even after depressive symptoms have remitted and thus might suggest vulnerability and lasting effects of the disorder (Maalouf et al. 2011).
In a systematic review and meta-analysis of studies that used the Cambridge Neuropsychological Battery (CANTAB), Rock et al. (2014) found that patients with current depression had deficits in executive functioning, attention, and memory, while patients in remission were also impaired in executive function and attention (Rock et al. 2014). They therefore proposed that the latter two functions are core features of MDD that extend beyond mood symptoms. A recent review and a recent meta-analysis showed that patients with MDD both in the remitted (Hasselbalch et al. 2011) and euthymic (Bora et al. 2013) states experience cognitive difficulties.
Adults remitted from depression after 6 months of treatment have been shown to improve on some cognitive domains such as memory and attention although there were residual deficits in motor and executive functioning, suggesting that the former functions were stable markers and the latter state-dependent markers of MDD (Huang 2009).We have previously shown that executive dysfunction and impulsivity are state markers of adolescents with MDD and not present in remission (Maalouf et al. 2011).
It has been suggested that the treatment of depressive symptoms significantly improves cognitive dysfunctions associated with them (Baune and Renger 2014). Many studies have investigated the role of serotonin and antidepressant treatment in cognitive functioning (Cowen and Sherwood 2013). A recent systematic review showed that selective serotonin reuptake inhibitors (SSRIs) and other antidepressants may improve functional and cognitive outcomes in adult MDD (Baune and Renger 2014). Conversely, some evidence, mostly in healthy populations, suggested that SSRIs such as citalopram and fluoxetine may reduce sustained attention and memory consolidation (Cowen and Sherwood 2013). A prospective follow-up case–control study in adult patients with MDD found that remitted patients had significant improvement in memory and attention, while executive and motor functioning remained impaired even after symptom remission (Huang 2009).
Patients treated over 24 weeks with an SSRI or a dual serotonergic–noradrenergic reuptake inhibitor (SNRI) were shown to have improved episodic verbal and visual memory and mental processing speed, with better memory improvement in the SNRI group (Herrera-Guzmán et al. 2010b). Herrera-Guzmán et al. (2009) noted that the cognitive improvements they found were independent from clinical improvement. In another study, patients with MDD who responded but did not achieve remission after 12 weeks of citalopram treatment had residual deficits in concentration and decision-making (McClintock et al. 2011).
Herrera-Guzmán et al. also investigated the neuropsychological functioning in patients with MDD in remission, previously treated with either SSRI or SNRI, and followed up in their medication-free recovery phase (Herrera-Guzmán et al. 2010a). Some improvement in planning was seen in recovery regardless of antidepressant type, whereas those treated with the SSRI showed worse outcomes in memory performance (Herrera-Guzmán et al. 2010a). Other longitudinal studies looking into changes in neurocognitive functioning in MDD mostly involved geriatric populations with and without dementia. For example, Diaconescu et al. (2011) found that geriatric patients with MDD showed significant improvement in immediate verbal memory and verbal fluency after 8 weeks of citalopram treatment.
There are, however, no studies investigating the longitudinal course of cognitive deficits in major depression in children and adolescents. The current study aims at investigating changes in neurocognitive functioning in adolescents with MDD as they are receiving an SSRI. We specifically aimed to investigate changes in sustained attention, impulsivity, planning, and visual memory in adolescent patients with MDD during a 12-week fluoxetine treatment.
We hypothesized that participants with MDD would show deficits in these measures at baseline compared with HCs and improve across the course of treatment in planning and inhibition. Specifically, they will, over time, use fewer steps in completing a multistep pattern copying task and commit fewer errors in inhibiting a nondesired response while also performing more accurately and rapidly on a sustained attention and behavior inhibition task. Most studies that have found a persistent cognitive deficit in remitted MDD were conducted with adult samples, while our previous work with the tasks used in this study has shown that planning deficit and impulsivity were present in patients with MDD in the acute phase, but not in those in the remitted phase (Maalouf et al. 2011). Our hypotheses for the current study are driven by our previous findings. This is, to our knowledge, the first study to examine cognitive changes longitudinally, following up the same patients in the acute stage of MDD during their course of treatment.
Methods
Participants
Twenty-four adolescents aged 12–18 years who met criteria for MDD, currently according to the Development and Well-Being Assessment (DAWBA), and obtained a score higher than 40 on the Childhood Depression Rating Scale-Revised (CDRS-R) participated in this study. In addition, 24 HCs with no psychiatric or neurological history and no previous psychiatric disorders in first-degree relatives were recruited. MDD participants were recruited from the outpatient Child and Adolescent Psychiatry clinic at the American University of Beirut Medical Center (AUBMC) and HCs were recruited through advertisements placed in the Family Medicine clinic at AUBMC. Participants were excluded if they obtained a Prorated Full Scale IQ of less than 80, had any history of psychotic symptoms, substance abuse or dependence, bipolar disorder, untreated attention-deficit/hyperactivity disorder (ADHD), head trauma or other neurological disease, had been on an antidepressant other than fluoxetine in the last 2 weeks, or if they had been on fluoxetine in the last 6 weeks.
Participants in the MDD group were started on fluoxetine according to the following protocol: fluoxetine 20 mg for the first 4 weeks with the option of increasing to 40 mg at week 5 and to 60 mg at week 8 if the score on the Clinical Global Impressions (CGI)—Improvement scale was greater than or equal to 3. Participants received psychoeducation during their assessment session, and no formal form of psychotherapy (cognitive behavior therapy or other) was provided during the course of this study.
Measures
Wechsler Nonverbal Scale of Ability
The Wechsler Nonverbal Scale of Ability (WNV) is a test of general cognitive ability for individuals of ages 4–21 years and 11 months (Wechsler and Naglieri 2006). It can be administered without any verbal instructions, making it suitable for testing of individuals from culturally and linguistically diverse groups and from different educational and socioeconomic backgrounds. It has the advantage of pictorial directions that make administration independent of native language. The WNV has demonstrated good validity and reliability, is well normed in the United States and Canada, and may be used with different populations to aid in clinical assessments (Wechsler and Naglieri 2006). The brief version of the WNV was administered in this study as a screening for nonverbal IQ. This version included two subtests, Matrices and Spatial Span that yield a single ability score. Individuals with a score below 80 were excluded from the study.
The Development and Well-Being Assessment
The DAWBA is a structured multi-informant interview that generates psychiatric diagnoses according to the Diagnostic and Statistical Manual of Mental Disorders 4th edition, text revised (DSM-IV-TR) (American Psychiatric Association 2000) and the International Classification of Diseases 10th edition (ICD-10) criteria (Frigerio et al. 2009). The DAWBA has excellent discriminant validity (Goodman et al. 2000) and has been adapted into various languages and used in numerous epidemiological and clinical studies worldwide (Fleitlich-Bilyk and Goodman 2004; Mullick and Goodman 2005; Pillai et al. 2008; Goodman et al. 2012). In this study, participants completed the online self-report Arabic version of the DAWBA. The Arabic DAWBA has demonstrated good diagnostic validity, sensitivity, and specificity in a child and adolescent clinical sample (Zeinoun et al. 2013). Psychiatric diagnoses were confirmed by FM, a child and adolescent psychiatrist.
The Children's Depression Rating Scale-Revised
The CDRS-R is a semi-structured interview administered to children and adolescents and one parent by a trained clinician to assess the severity of the child's or adolescent's depressive symptoms. The CDRS-R has demonstrated strong internal consistency (α = 0.85), test–retest reliability (r = 0.81), and inter-rater reliability (r = 0.86) in a pediatric population (Poznanski et al. 1984; Wood et al. 2007), and similarly good psychometric properties in an adolescent population, with internal consistency α as high as 0.92. An Arabic version of the CDRS-R was used in the current study. The original English version was translated to Standard Modern Arabic by a Master's level graduate in Public Health and back-translated by a Master's level psychologist who was not exposed to the original English scale. The back-translated version was then compared with the original English version for discrepancies, and the Arabic version was revised and finalized accordingly. The Arabic CDRS-R was found to have high internal consistency, Cronbach's α = 0.94. In our study, a CDRS score of 28 or below was used to define remission.
The Beck Depression Inventory-II
The Beck Depression Inventory-II (BDI-II) is a self-report questionnaire comprising 21 questions assessing symptoms of depression, each rated by the patient on a scale of 0–3. It has high internal consistency (Cronbach's α = 0.91) (Beck et al. 1996a, 1996b) and was found to have good reliability and discriminant and convergent validity in adolescent populations (Kumar et al. 2002; Osman et al. 2004). Participants completed the Arabic version of the BDI-II, which has demonstrated good reliability and validity, and a factor structure similar to that of the original BDI-II (Al-Musawi 2001).
Computerized tasks from the CANTAB; Cambridge Cognition, United Kingdom, 2006
Delayed matching to sample
This task measures immediate and delayed visual memory using a four-choice simultaneous and delayed recognition memory paradigm. Participants are presented with a complex visual pattern and instructed to choose the one identical to it from a display of four different patterns presented either simultaneously or with a delay of 0, 4, or 12 seconds after the target pattern disappears. The primary outcome variable is the percentage of total correct responses.
Rapid visual processing
This is a test of sustained attention, inhibition, and impulsivity, and speed of information processing. Participants are presented with a white box at the center of the screen, where digits from 2 to 9 are displayed randomly at the rate of 100 digits/minute. Participants are instructed to press the touch pad as soon as they detect specific target sequences: 2-4-6, 3-5-7, and 4-6-8. The duration of this task is 7 minutes and the main outcome measures are total hits, total false alarms, as well as measures of target sensitivity (A′) and response bias (B″). Rapid visual processing (RVP) A′ is the signal detection measure of sensitivity to the target, which indicates how well the participant can detect the target ranging from 0.00 to 1.00 and is therefore a measure of sustained attention. RVP B″ is the signal detection measure of the strength of visual trace required to elicit a response, which indicates the tendency to respond regardless of the presence of the target. It ranges from −1.00 to 1.00 and tests for inhibition and impulsivity.
Stockings of Cambridge
This task is a measure of planning and problem solving, and is suggestive of executive functioning. Participants are presented with two displays of colored balls presented as stacks of colored balls held in socks suspended from a beam. Participants are instructed to use the lower display to copy the pattern presented in the upper one using a specified number of moves. The balls may be moved one at a time by touching the ball to be moved and then touching the place in the display where the participant wishes to move it. The primary outcome measures are the mean number of moves in the problems requiring 2, 3, 4, and 5 moves.
Procedure
Participants who met criteria for an MDD and whose parents consented to a trial of fluoxetine were referred by their psychiatrist to potentially enroll in this study. Those who agreed to participate were administered at the initial assessment the WNV and the computerized version of the Arabic DAWBA to ascertain the diagnoses, as well as baseline CDRS-R and BDI. Clinician-rated CGI scores were also recorded. CDRS-R, BDI, and CGI were repeated at week 6 and 12. HCs completed the same scales at baseline and after 6 and 12 weeks. All participants were also administered the neurocognitive tasks at baseline and at weeks 6 and 12 with the CANTAB tasks administered in the same order in each session and for all groups and individuals.
The study protocol was approved by the local institutional review board (IRB). The primary investigator or members of the research team explained and discussed the study procedures with both the adolescents and one of their parents, at the same time. All adolescent participants signed an assent and their parents signed an informed consent. Over the course of the study, a total of 53 participants were recruited. Five of those were later excluded: one participant from the HC group for having evidence of depression on the DAWBA, another participant from the HC group for not completing the first assessment, one participant from the MDD group due to a change in diagnosis upon reassessment, one participant from the MDD group due to an adverse event related to SSRI use (acute aggression, suicidality, and hospitalization), and one participant in the MDD group for not completing the baseline assessment.
Statistical analyses
All analyses were conducted using IBM SPSS Statistics version 22.0 (2013) and R statistical software. Pearson correlations were conducted to test for bivariate associations between variables. Multilevel linear models fit by maximum likelihood estimate were used to investigate the differences between the MDD and HC groups across time in their performance on the different CANTAB tasks. Fixed effects were defined as participant ID and random effects were defined as MDD and HC groups and assessment times, with the different task measures as outcome variables. Different models were built for the differences between baseline and week 6 on one hand, and between baseline and week 12 on the other. Two-tailed tests were used, and threshold for statistical significance was set at α = 0.05.
Results
Demographics
MDD and HCs did not differ in age (t(46) = 1.25, p = 0.22); 58% of HCs and 67% of MDD were females, with no statistically significant difference (χ 2 (1) = 0.36, p = 0.55) (Table 1).
Data are presented as mean (standard deviation) or n (%).
BDI, Beck Depression Inventory; CDRS, Child Depression Rating Scale; HC, healthy control; MDD, major depressive disorder.
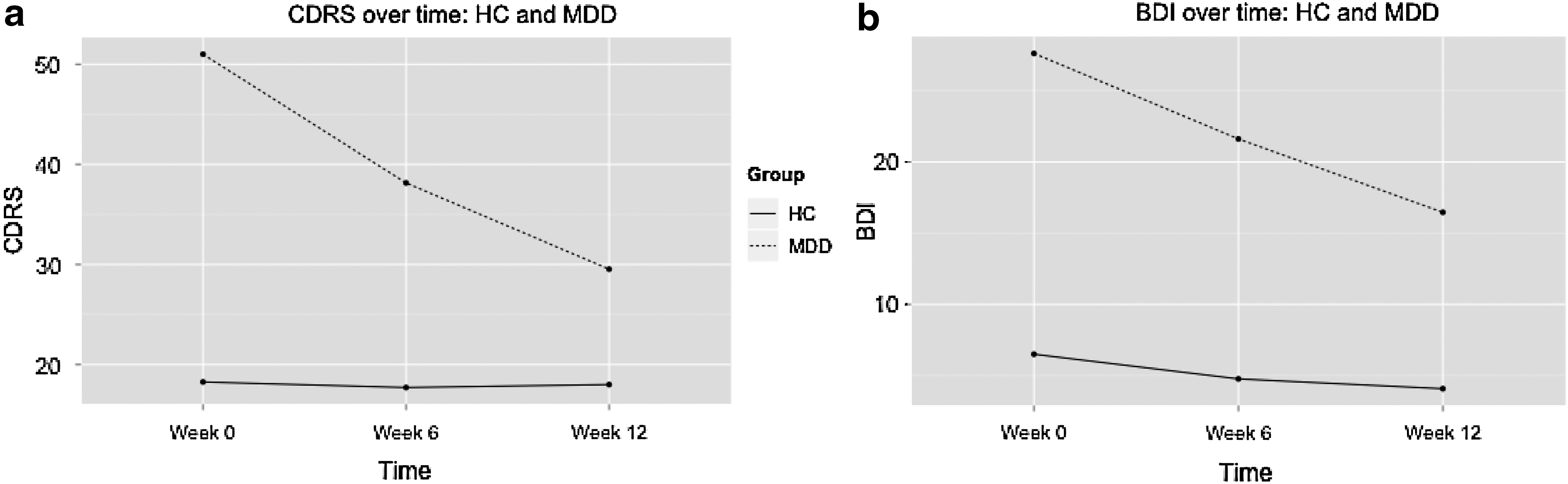
The two groups showed a significant difference in CDRS scores at baseline (t(26) = −20.59, p < 0.001), week 6 (t(23) = −6.7, p < 0.001), and week 12 (t(14) = −3.54, p = 0.003), and in BDI scores at baseline (t(46) = −8.58, p < 0.001), week 6 (t(28) = −5.39, p < 0.001), and week 12 (t(16) = −3.28, p = 0.005). MDD had significantly higher scores on all occasions (Table 1 and Fig. 1). The clinical characteristics of the MDD group are presented in Table 2. Two participants had comorbid treated ADHD, one participant had comorbid oppositional defiant disorder, and 12 participants had a comorbid anxiety disorder. All patients were instructed to take their medications as prescribed on the day of testing.
CDRS
DMS, delayed matching to sample; HC, healthy control; RVP, rapid visual information processing; SOC, stockings of Cambridge; W0, week 0; W6, week 6; W12, week 12.
Delayed matching to sample
This task showed a significant group main effect across sessions for Percent Correct measure in all delays, between baseline and week 6 (b = −9.82, t(46) = −3.01, p = 0.004), and between baseline and week 12 (b = −11.46, t(46) = −3.5, p = 0.001). MDD performed more poorly than HCs, having less percent correct across all assessment times (Table 2).
A main effect of group was found specifically in Percent Correct in 0 and 12,000 mseconds delay tasks at both week 6 (b = −8.67, t(46) = −2.12, p = 0.04 for 0 mseconds; b = −8.82, t(46) = −2.14, p = 0.04 for 12,000 mseconds) and week 12 (b = −10.84, t(46) = −2.81, p = 0.007 for 0 mseconds; b = −10.81, t(46) = −2.26, p = 0.03 for 12,000 mseconds), and 4000 mseconds delay only at week 12 (b = −9.11, t(46) = −2.22, p = 0.03), but was not found in the simultaneous condition.
Rapid visual processing
Between week 0 and week 12, there was a significant interaction effect of group and time for RVP A′, b = −0.04, t(25) = −2.42, p = 0.02; HCs had a higher increase in A′ scores from baseline to week 12 than did MDD. This suggests that on this measure of sustained attention, HCs improved much more than MDD did from week 0 to 12. There was only a time main effect between baseline and week 6, b = 0.02, t(37) = 2.18, p = 0.04, with higher A′ scores at week 6 for both HCs and MDD (Table 2).
There was also a significant group main effect for weeks (0–12) in the RVP B″ measure, through which HCs had higher B″ scores across testing times (b = −0.06, t(46) = −2.34, p = 0.02). This suggests that MDD showed more impulsivity on this measure compared with HCs across time. There were no significant effects at week 6 (p ≥ 0.05) (Table 2).
RVP total hits showed a significant interaction of group and time for weeks (0–12), b = −4.06, t(25) = −2.65, p = 0.01; HCs had a larger increase in total hits than MDD, suggesting that HCs improved significantly more on this task than did MDD. Post hoc t-tests showed that there was a significant difference in total hits between HCs and MDD at week 12, t(25) = 2.89, p = 0.008, but this difference was not significant at baseline (p ≥ 0.05) (Table 2).
Stockings of Cambridge
Between week 0 and week 12, there was an interaction effect of group and time for mean moves in the 5-move problems, b = 1.22, t(23) = 2.14, p = 0.04; mean moves decreased in HCs across time but remained high for MDD (Table 2). There were no significant effects at week 6 (p ≥ 0.05). There were also no significant interaction effects in stockings of Cambridge (SOC) mean moves for problems requiring less than 5 moves at week 6 or week 12 (p ≥ 0.05).
Exploratory analyses
Exploratory subanalyses were conducted to compare participants in the MDD group who remitted at week 12 (REMIT, n = 10) to HCs. The results replicate those found in the full MDD sample. There was a significant group main effect for delayed matching to sample (DMS) percent correct on all delays, b = −11.45, t(46) = −3.38, p = 0.002; REMIT had less percent correct than HCs across time. There was also a significant interaction effect of group and time for RVP A′, b = −0.04, t(20) = −2.52, p = 0.02, and for RVP total hits, b = −4.31, t(20) = −2.86, p = 0.01, and a significant group main effect or RVP B″, b = −0.06, t(46) = −2.31, p = 0.03. HCs had a larger increase in RVP A′ and RVP total hits over time, and had higher RVP B″ at both baseline and week 12.
For SOC, there was a significant group (b = −1.44, t(45) = −2.42, p = 0.02) and time (b = 1.2, t(21) = 3.37, p = 0.003) main effects for problems solved in minimum moves; HCs had more problems solved across testing times. There was also a significant time main effect for mean moves in the 3-move condition, b = −0.19, t(21) = −2.23, p = 0.04, with both groups having decreased mean moves in this condition at week 12; and a significant group main effect for mean moves in the 4-move condition, b = 0.73, t(45) = 2.69, p = 0.01; REMIT had more mean moves in this condition across time. The finding of a significant interaction effect for mean moves in the 5-move condition did not hold for the REMIT group as it did for the full MDD group. When this interaction effect was included in the model for REMIT, there was a significant time main effect, b = −1.21, t(18) = 1.73, p = 0.01, suggesting that both HCs and REMIT improved on this condition (mean moves decreased for both) over 12 weeks.
Additional analyses were also conducted to investigate the correlation between changes in cognitive measures and in CDRS scores across time in the MDD group. There were no significant correlations between change scores in CDRS and any of the cognitive changes.
In the MDD group, CDRS and BDI scores significantly improved over time, F(2, 34) = 23.17, p < 0.001 for CDRS and F(2, 34) = 4.84, p = 0.01 for BDI.
Discussion
This study investigated changes in neurocognitive functions in adolescents with MDD compared with HCs during SSRI treatment. Our results showed a deficit in visual memory in adolescents with MDD compared with HCs that remained present 12 weeks after SSRI treatment. In addition, on a task of sustained attention and inhibition, HCs became better at detecting target sequences at week 12, while there were residual sustained attention deficits in adolescents who also remained more impulsive compared with HCs on this task throughout the 12 weeks. These results suggest that HCs improved on this task, most likely due to a practice effect, at a rate that was faster than MDD.
Finally, adolescents with MDD differed in their performance on a planning task compared with HCs. Our results specifically showed that while HCs improved substantially in their performance on the most demanding condition of this planning task after three assessments over 12 weeks, the performance of adolescents with MDD did not significantly change. Our hypothesis of improvement in impulsivity, planning, sustained attention, and memory in participants with MDD was, therefore, not confirmed.
A recent systematic review and meta-analysis of studies using the CANTAB to assess cognitive functioning in patients with current or remitted depression found significant deficits in currently depressed patients on tasks of executive function, visual memory, and sustained attention (Rock et al. 2014). Remitted patients also showed deficits in executive function and attention, whereas they only had a tendency toward a deficit in memory (Rock et al. 2014). The current study goes in line with these findings, with medicated MDD patients showing deficits in visual memory 12 weeks into treatment.
Other studies have found visual memory not to be impaired in children, adolescents (Brooks et al. 2010), and young individuals with MDD (Baune et al. 2012). Worse performance on a computerized delayed visual memory test in children and adolescents with depression was not found to be statistically significant compared with HCs, although impairment on the memory domain had a small-to-medium effect size (Brooks et al. 2010). Brooks et al. argued that these results might be due to low statistical power and heterogeneous scores in children, as they found a medium effect size for delayed verbal memory and a small effect size for delayed visual memory.
The current findings in an adolescent-only group might suggest that this deficit is prominent in adolescents but not children. Baune et al., however, found no impairment in visuospatial ability in 13–25-year olds with a lifetime history of nonpsychotic MDD in a case–control study. Their visual task, the Tower of London, did not involve visual memory but only visual planning and problem solving, making it different from the DMS task used in this study. A previous study comparing adolescents with MDD in an acute episode, those in remission, and HCs on the same task of visual memory found no difference between the groups in visual short-term memory (Maalouf et al. 2011). The contrasting current results are likely due to the fact that not all of our patients were in remission by week 12.
Our findings on sustained attention showed that there was no difference at baseline between HCs and MDD, but HC became better at detecting target sequences at week 12 while MDD did not improve at the same rate. A recent meta-analysis showed that children and adolescents with MDD had deficits in sustained attention and inhibition (Wagner et al. 2015). Specifically, on computerized tasks of continuous performance, children and adolescents with depression committed more errors and omissions, suggesting problems with sustained attention, inhibition, and impulsivity (Brooks et al. 2010). Indeed, in a previous study where adults with unipolar depression were compared with those with bipolar depression and those with bipolar in a euthymic episode, sustained attention deficits were found in the bipolar groups only and were not present in depression (Maalouf et al. 2010).
In addition, Favre et al. (2009) compared children and adolescents with MDD to HCs and found that most neurocognitive functions were not impaired in the MDD group, including distractibility. Other studies have found that adolescents with acute MDD but not those in remission were impaired on inhibition but not on sustained attention measured by target sensitivity (Maalouf et al. 2011). It may be that, however, the most consistent positive findings of impairment in the domain of attention in individuals with depression come from studies investigating emotionally valenced stimuli rather than neutral tasks. Results from tasks such as the dot-probe, the emotional n-back, and the affective go/no go have shown that children and adolescents with depression have an attentional bias toward negative stimuli (Clark et al. 2009; Maalouf et al. 2012; Vilgis et al. 2015).
The improvement seen in HCs on this attention task in our study was most likely due to practice effect, which has been shown in HCs to occur over the first 3 months of repetitive testing (Bartels et al. 2010). Reduced anxiety, familiarity with the testing environment, recall effect, and procedural learning, have been postulated to explain practice-induced performance improvement in cognitive testing (Bartels et al. 2010). This practice effect seen in HCs on the RVP was observed to a much lesser degree in MDD, who failed to show the same improvement on the task.
Whereas sustained attention and inhibition constitute core components of executive functioning, the current study additionally investigated executive function through a planning and problem-solving task. In this study, although there was significant improvement in the performance of HC group from baseline to week 12, no improvement was detected in the MDD group. While HCs were able to learn the task over time, MDD did not, suggesting a practice effect in the HC group. It is possible that depression reduces the ability of the participants to use their cognitive resources to learn the task, or that functioning of brain areas associated with learning executive tasks is altered (Ho et al. 2014). It is worth noting that our finding was only evident in the most difficult part of the task suggesting that difficulty in learning to solve challenging multi-step problems is evident in participants with MDD.
Studies investigating planning performance in adolescent depression have yielded various results. One study found minimal evidence for executive functioning deficit, regardless of some evidence for planning difficulties (Vilgis et al. 2015), and another study found that adolescents with an acute MDD episode performed worse than both HCs and those with remitted MDD on the same planning task used in this study (Maalouf et al. 2011). Similarly, while impairments were observed in most complex tasks of neuropsychological functioning, planning ability was intact in a case–control study of adolescents and young adults (Baune et al. 2012). As executive functioning is a multidimensional construct and each component can be argued to still be developing throughout adolescence, it would be valuable to conduct more specific assessment of a variety of planning tasks to isolate the specific deficits found in depression.
A number of limitations need to be considered in the interpretation of the current findings. It is important to note that although the adolescent participants with MDD were on SSRI treatment for the 12-week period, many did not reach remission at week 6 or week 12. In fact, five MDD participants out of 21 at week 6 and 10 out of 15 at week 12 were considered to be in remission. This may have negatively affected the results, as improvement in cognitive functions may be related to improvement of depressive symptomatology and not only a direct effect of medication treatment. An exploratory analysis of the remitter subgroup, however, yielded results that are similar to our current findings suggesting that our findings are independent of clinical improvement. The number of remitters versus nonremitters at each assessment point also hindered the possibility of analyzing these groups separately or comparing remitters to nonremitters to determine whether the participants showing depressive symptoms were driving the negative findings. One of the main limitations of the current study is the sample size, and as participants drop out at the second and third assessments, it could be argued that there does not remain enough power to detect small but significant changes in the performance of the MDD group. Related to this is the likelihood that those who dropped out were in fact those who were remitted and therefore were not motivated to complete the assessments. If this was true, the improvement in neurocognitive performance in the MDD group would be underestimated.
Conclusions
To sum up, this is the first study that investigated changes in neurocognitive functioning during a course of SSRI treatment in adolescent depression. We showed that adolescents with depression remained impaired on measures of visual memory throughout the course of treatment compared with controls. In addition, while HCs improved on measures of sustained attention and planning, most likely due to practice effect, adolescents with depression did not.
Future studies following the longitudinal design need to be conducted to elucidate more clearly the relationship between depression, neurocognitive functioning, and medication treatment in adolescents. These studies should aim at having larger sample sizes and differentiate between outcomes of responders and nonresponders to treatment. The replication of the current findings can have implications for the identification of cognitive difficulties that depressed adolescents might face during the course of their illness and its treatment.
Clinical Significance
Despite treatment with SSRIs, depressed adolescents remained impaired on measures of visual memory and did not improve on measures of sustained attention and planning. Further studies are needed to confirm these findings and to investigate CBT-based or pharmacological interventions that improve these measures. Clinicians need to be aware that improvement in cognitive functions may lag behind improvement in depressive symptoms in this age group.
Footnotes
Acknowledgments
We would like to thank Ms. Mia Atwi, Ms. Lucy Tavitian, and Dr. Nayla Hariz for their efforts in data collection.
Disclosures
Ms. Al Amira Safa Shehab has nothing to disclose in relation to this study. Dr. David Brent receives royalties from Guildford Press, ERT Inc., and HealthWise. He receives consulting fees from Lundbeck and UptoDate. Dr. Fadi Maalouf receives grants support from the Medical Practice Plan – Faculty of Medicine at the American University of Beirut and is on the speaker Bureau of Eli Lilly and Company.