
Abstract
Objective:
In this study, it was aimed to understand the underlying possible immunopathogenesis of first episode, early onset schizophrenia (EOS) through profiling the T helper 1 (Th1) cell cytokines TNF-α, IFN-γ, and IL-2, Th2 cell cytokines IL-4 and IL-10, Th17 cell cytokine IL-17A, and inflammatory cytokine IL-6.
Methods:
The study included a total of 30 children, admitted to child psychiatry outpatient clinic aged between 10 and 17 years of age, who had not received prior therapy and were diagnosed with psychosis according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) as the patient group, and 26 age- and gender-matched children as the control group. Structured psychiatric interviews (K-SADS-PL and PANSS) were conducted with all participants. The BD Cytokine Bead Array Human Th1/Th2/Th17 Cytokine Kit is used for the measurement of serum cytokines, for example, IL-2, IL-4, IL-6, IL-10, IL-17A, TNF-α, and IFN-γ.
Results:
There was no significant difference between groups in terms of IL-2, IL-4, IL-6, IL-10, IL-17A, TNF-α, and IFN-γ levels (p > 0.05). However, there was a significant correlation between IL-10 and IL-4 with negative symptoms of EOS (r = −0.65, p = 0.02 and r = 0.67, p = 0.02, respectively).
Conclusion:
IL4 and IL-10 levels have a relationship with negative symptoms of disease. Therefore, this study might suggest that immunological processes might have a role in the disease pathophysiology.
Introduction
T
Schizophrenia is reported to be associated with at least three interacting pathophysiological mechanisms:dopaminergic dysregulation, impaired glutamatergic neurotransmission, and increased proinflammatory status (Kahn and Sommer 2015). A study on 180 drug-naive FEP patients has shown that nearly one-third of them have high levels of immune markers (Schwartz et al. 2012). A recent postmortem study on schizophrenia patients has shown that 40% of the patients have inflammation (Fillman et al. 2013).
A number of studies have shown a relationship between schizophrenia and the immune system. For example, a correlation was previously identified between pre- and perinatal infection and the risk of developing schizophrenia (Canetta and Brown 2012). Similarly, infectious agents such as influenza, bornavirus, Chlamydia, and Toxoplasma gondii were associated with the risk of eventual development of schizophrenia (Muller and Schwarz 2010). A family history of autoimmune diseases and a history of severe infections requiring hospitalization also increased the risk of developing schizophrenia (Benros et al. 2014). Furthermore, a correlation was observed between childhood (9 years of age) elevated IL-6 and C-reactive protein levels and development of psychosis in young adulthood (18 years of age) (Khandaker et al. 2014). The increased risk of developing schizophrenia has been also identified for certain allergic diseases, such as asthma (Pedersen et al. 2012).
It was hypothesized that T helper cell imbalance has a role in a subtype of schizophrenia (Schwarz et al. 2001). In addition, T helper 2 dominance was presented in acute exacerbation of schizophrenia (Avgustin et al. 2005). T helper 1 (Th1) effector cells produce IL-2, IFN-γ, and TNF-α (Ruffell et al. 2010), Th2 effector cells produce IL-4, IL-5, IL-10 (Agarwal et al. 2010), and Th17 effector cells produce IL 17 (Harrington et al. 2005). T helper cell function might be modulated by dopaminergic and glutamatergic neurotransmission, related with schizophrenia (Huang et al. 2010; Gao et al. 2011). Th cytokines might have a role in the pathogenesis of schizophrenia by modulating the tryptophan/kynurenine pathway (Müller et al. 2009).
The current study investigated the role of T helper cells by measuring the differences in the levels of major Th1, Th2, Th17, and inflammatory cytokines, such as IL-2, TNF-α, IFN-γ, IL-4, IL-10, IL-17A, and IL-6, between first episode EOS and control groups. In addition, the study aimed to evaluate any association between the symptom severity of EOS and duration of untreated psychosis, and indicated cytokine levels.
Methods
Participants
The study was conducted in the Department of Child Psychiatry at the Dicle University Training and Research Hospital, Diyarbakır, Turkey. The study data were collected between May 2014 and April 2015. A total of 48 adolescents with psychotic disorders were admitted within the data collection period. Of these, 41 cases agreed to be involved in the study; however, 11 cases were excluded based on the exclusion criteria. Finally, 30 adolescent patients admitted to child psychiatry outpatient clinic aged between 10 and 17 years who had not received prior therapy and who were diagnosed with psychosis according to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) (American Psychiatric Association 2013) (acute psychosis, schizophreniform disorder, schizophrenia), and 26 age- and gender-matched healthy adolescent control subjects aged between 10 and 17 years who did not have a medical or neurological disorder were included in the study.
Children who scored below 70 points in an intelligence test, who had chronic systemic diseases such as epilepsy, asthma, and diabetes, who had neurodevelopmental disorders such as autism, attention-deficit/hyperactivity disorder (ADHD) and tic disorder, history of severe head trauma, ≥30 body mass index (BMI), clinically active infection, and history of substance abuse in the last 6 months, and who received oral contraceptives, psychotropics, antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs), previous or current corticosteroid therapy, and vitamins were excluded. Substance levels in urine were screened in suspected cases. Five patients were excluded due to existence of ADHD. The patients were diagnosed with schizophrenia after a 6-month follow-up period.
The parents of the patients provided informed consent for all study participants. Patients were evaluated by two psychiatrists. Inter-rater agreement was 0.80. Ethical approval of the study protocol was obtained from the Non-Interventional Clinical Research Ethics Committee at the Dicle University Faculty of Medicine.
Forms and scales
Sociodemographic data and clinical data form
This form contained questions regarding age, gender, education level, age of the parents, consanguinity between parents, number of siblings, history of psychiatric disorder among family members and relatives, family history of alcohol/substance abuse, height, and weight. Blood samples were collected on the same day that data form and other scales were administered while patients did not take any kind of medication.
Kiddie Schedule for Affective Disorders and Schizophrenia, Present and Lifetime version
The original scale was developed by Kaufman et al. (1997). This scale was adapted to the Turkish language by Gökler et al. (2004). The Kiddie Schedule for Affective Disorders and Schizophrenia, Present and Lifetime version (K-SADS-PL) was administered during an interview with the parents and children, and the final evaluation was performed using input from all data sources. The scale evaluated the presence of psychopathological conditions in children and adolescents.
The Positive and Negative Symptom Scale
This scale was a semistructured interview tool developed by Kay et al. (1987), and the scale was evaluated for its validity and reliability by Kostakoğlu et al. (1999) and Kay et al. (1987). The scale consisted of 30 items evaluating positive and negative symptoms and, providing information about the general psychopathological condition.
The Clinical Global Impressions Scale
The Clinical Global Impressions Scale (CGI) was a standardized evaluation tool used to rate disease severity, disease course over time, and drug effects according to the clinical condition of the patient and the severity of side effects. CGI-I was rated on a seven-point scale from 1 (normal) to 7 (severe disease) (Guy 1976).
Cytokine bead array
Blood samples were obtained in the morning, postprandial, between 10:00 a.m. and 12:00 p.m. The samples were collected in gel tubes. Blood samples were stored at room temperature for 30 minutes for coagulation. Then, blood samples were centrifuged at 1000 g for 10 minutes. The sera were transferred to 1.5-mL polypropylene tubes and stored at −80°C until the analysis. The BD Cytokine Bead Array (CBA) Human Th1/Th2/Th17 Cytokine Kit (Cat. no. 560484; BD Biosciences), FCAP Array v3.0 software (23-13454-00; BD Biosciences), and BD FACSVerse system (23-13453-00; BD Biosciences) were used for the measurement and analysis of cytokines IL-2, -4, -6, -10, -17A, IFN-γ, and TNF-α. Serum was used without dilutions for CBA.
Statistical analysis
The Student's t-test was used to compare normally distributed variables between independent groups, and the Mann–Whitney U-test was used to compare nonnormally distributed categorical variables. Gender, alcohol abuse in the family, consanguineous marriage, history of psychiatric disorder in the family members and relatives, and smoking status were tabulated as categorical values. Differences between the groups were evaluated using the Chi-square test or Fisher test, where appropriate. The Pearson's test was used to evaluate correlation coefficients of normally distributed variables, and the Spearman's test was used to evaluate nonnormally distributed variables. If an association was detected between the variables, including IL-4, IL-10, TNF-α, CGI, and negative symptoms, simple linear regression analysis was performed in the further analysis of them. The values were given as mean ± standard deviation. The p-value below 0.05 was considered statistically significant.
Results
The mean age was 14.7 ± 1.9 years among adolescents in the FEP group (range: 10–17 years; M/F: 13/17) and the mean age was 14.5 ± 1.9 years in the control group (range: 10–17, M/F: 12/14). There was no significant difference between the groups in terms of age and gender. Past medical history of the family members and first-degree relatives of 11 patients in the FEP group was remarkable for psychiatric disorder, whereas there was one patient's history of psychiatric disorder in the control group (p = 0.01). There was no significant difference between the groups in terms of family history of alcohol or substance abuse. The consanguineous marriage rates were similar between groups (p = 0.05). There was no significant difference between the groups in terms of smoking history. The average age of mothers was significantly higher in the FEP group (p = 0.01). The education level of the participants, the age of the parents, height, weight, and BMI values are presented in Table 1.
Bold values are statistically significant.
BMI, body mass index; FEP, first episode psychosis; SD, standard deviation.
The mean CGI score was 4.5 ± 1.0. The mean age at disease onset was 13.6 ± 1.8 years. The mean duration of untreated psychosis was 12.9 ± 13.2 months. The CGI score increased with increasing duration of untreated psychosis (r = 0.43, p = 0.03). The mean Positive and Negative Symptom Scale (PANSS) positive score was 21.5 ± 8.3, the mean PANSS negative score was 26.3 ± 8.2, and the mean PANSS general psychopathology score was 40.0 ± 9.1. Data of the scales are given in Table 2.
CGI, Clinical Global Impressions Scale; DUP, duration of untreated psychosis; PANSS, Positive and Negative Symptom Scale; SD, standard deviation.
There were no significant differences between groups in terms of levels of IL-17A, TNF-α, IFN-γ, IL-10, IL-6, IL-4, and IL-2. The FEP group also showed higher IL-2 levels and lower IL-10 levels, although this was not statistically significant (p = 0.06, p = 0.05, respectively) (Table 3). There was significant correlations between IL-10 and IL-4 with negative symptoms (r = −0.65, p = 0.02; r = 0.67, p = 0.02, respectively) (Figs. 1 and 2). In the regression analysis, the association between IL-10, IL-4, and negative symptoms was statistically significant (r = −0.721, p < 0.001; r = 0.708, p = 0.008, respectively). In the presence of 1 pg/mL increase in the level of IL-10 results in 0.3 score decrease, but 1 pg/mL increase in the level of IL-4 results in 0.9 score rise in the negative symptoms, respectively. There was a correlation between TNF-α and disease severity (r = −0.54, p < 0.01). However, in the regression analysis, no significant association was detected between TNF-α and disease severity (r = −0.163, p = 0.409) (Table 4).
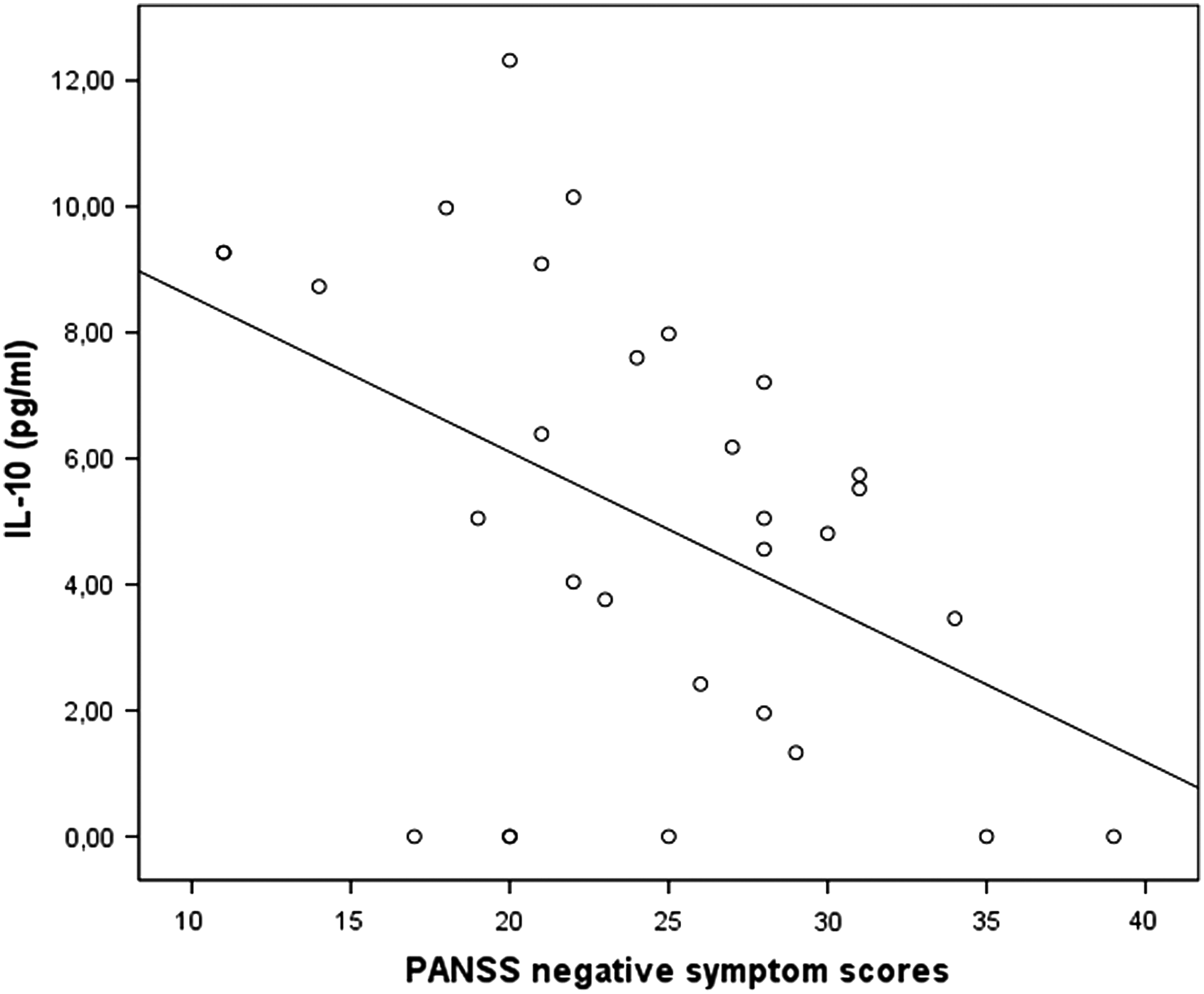
The relationship between IL-10 and PANSS negative symptom scores (r = −0.650, p = 0.020). IL, interleukin; PANSS, Positive and Negative Symptom Scale.
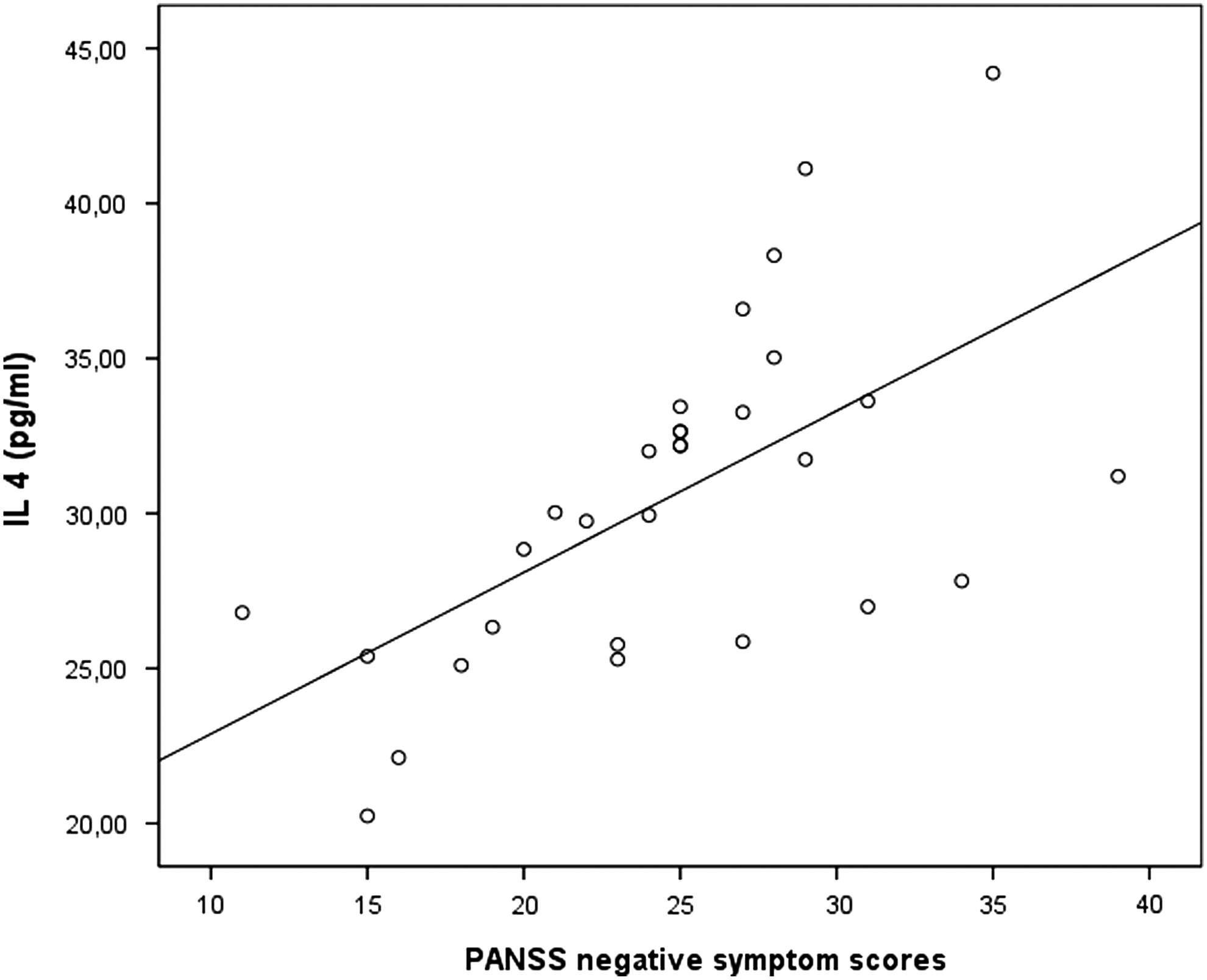
The relationship between IL-4 and PANSS negative symptom scores (r = 0.670, p = 0.020). IL, IL, interleukin; PANSS, Positive and Negative Symptom Scale.
FEP, first episode psychosis; SD, standard deviation.
Bold values are statistically significant.
CGI, Clinical Global Impressions Scale; PANSS, Positive and Negative Symptom Scale.
Discussion
The most important finding of our study was that the patient group showed a negative correlation between negative symptoms and IL-10 levels, and a positive correlation between negative symptoms and IL-4 levels. Nonetheless, there were no significant differences between first episode EOS patients and the control group with respect to their Th1/Th2/Th17 and inflammatory cytokines. What is more, the patient group showed a negative correlation between disease severity and TNF-α level. However, the level of TNF-α was not a predictive factor for the disease severity.
Many studies have found no correlation between the IL-4, IL-6, IL-10, and TNF-α cytokines and the severity of the disease (Naudin et al. 1997; O'Brien et al. 2008; Miller et al. 2011; Borovcanin et al. 2012, 2013; Kubistova et al. 2012). However, in this study it was found that serum levels of IL-4 and IL-10 cytokines were associated with severity of negative symptoms of EOS.
First of all, a negative correlation was found between negative symptoms and IL-10 levels here in parallel to the findings of other studies (Gladkevich et al. 2004; De Witte et al. 2014; Noto et al. 2015a). It was reported that chronic administration of lipopolysaccharide (LPS) decreased the production of IL-10, and the antidepressant effect of fluoxetine was accompanied by elevated IL-10 in the LPS-induced animal depression model (Kubera et al. 2013). Another report presented that kynurenine precipitated anhedonia, and IDO enzyme had a key role in LPS-induced depression in mice (Salazar et al. 2012). Moreover, kynurenine metabolites such as kynurenic acid were claimed to have a significant role in the pathogenesis of schizophrenia (Jayawickrama et al. 2015). In parallel, our findings also showed a correlation between the cytokines and negative symptoms such as anhedonia. These data might suggest that IDO and kynurenine pathway should have a role in the pathogenesis of negative symptoms of schizophrenia.
Second of all, a positive correlation was presented here between IL-4 level and negative symptoms. In addition, it was claimed that not only the serum level of Th2 type cytokine, such as IL-4, was elevated in schizophrenia patients, but also antipsychotics could decrease serum IL-4 (Borovcanin et al. 2012, 2013).
Finally, in the present study, we observed a negative correlation between the severity of the disease and TNF-α level. However, the level of TNF-α was not a predictive factor for the disease severity. According to our findings, there was not a prominent inflammation or indicated T helper cell activity in EOS; nevertheless, subtle level of IL-4 and IL-10 cytokine correlate with the severity of negative symptoms of EOS. It seems that IL-4 and IL-10 show their pathologic effect relaying on different dynamics.
This result suggests that inflammation might have a role in the pathogenesis of EOS. For example, the excessive dopamine in EOS might stimulate macrophages and T helper cells through D2 receptor and result in low-level IL-10, low-level TNF-α, and high-level IL-4 secretion (Huang et al. 2010; Matalka et al. 2011). Another example, excessive Th2 cytokine, IL-4, could inhibit IDO and decrease the synthesis of kynurenic acid, which has neuroprotective effect through the NMDA receptor (Müller et al. 2009).
As far as we know, the only study, which was performed on the same age group, reported that the serum TNF-α levels were similar between children with the diagnosis of childhood-onset schizophrenia and the control subjects (Sporn et al. 2005). In another study, IL-2, IL-4, IL-10, IFN-γ, and TNF-α levels in cerebrospinal fluid were evaluated in children with three different neuropsychiatric diseases (childhood-onset schizophrenia, obsessive-compulsive disorder, and ADHD) (Mittleman et al. 1997). Among these neuropsychiatric diseases, the Th2 cytokine IL-4 was reported to predominate in childhood-onset schizophrenia patients. On the other hand, the study had no healthy subject as a control group. In addition, IL-2, IL-4, IL-6, TNF-α, and IFN-γ levels were not different between suicidal psychotic adolescents and the control group (Falcone et al. 2010). Thus, our findings could give supportive knowledge on the favor of Th2 dominance in the schizophrenia pathogenesis.
In studies on adult FEP and schizophrenia patients, there have been growing evidences that immunological processes play a role in the pathophysiology of the disorder. A meta-analysis on treatment-naive FEP patients has shown no significant differences in IL-2, IL-4, and IFN-γ levels, whereas IL-6 and TNF-α were identified as the most consistently increasing cytokines. These cytokines were reported to have proinflammatory roles in the adaptive immune system (Upthegrove et al. 2014). For instance, it was found that IL-6, IL-10, and TNF-α levels were higher in FEP patients compared with the control group (Noto et al. 2015b). However, another study has failed to identify any significant difference in IL-6 levels between FEP patients and the control group (Graham et al. 2008). Borovcanin et al. (2013) have shown that IL-17 levels were significantly lower in the FEP group compared with the control group.
A postmortem study on schizophrenia patients reported that inflammation was more pronounced in the advanced stages of the disease (Narayan et al. 2008). However, cytokine production in children was different from adults (Lilic et al. 1997). In the light of the reports, it might be suggested that the cytokine profile might be different in pediatric patients than adult patients due to differences in age, method, sample size, and disease stage.
All subgroups of schizophrenia patients might not share the same pathogenetic mechanisms (Kahn and Sommer 2015). In a study on 180 treatment-naive FEP patients, high levels of immunity markers were identified in almost one-third of the patients (Schwartz et al. 2012). Similarly, in another postmortem study on schizophrenia patients, it was found that low-grade inflammation was present in 40% of the patients (Fillman et al. 2013). In a recent review, it was reported that low-grade inflammation in the brain might be associated with cognitive disorders and negative symptoms in first episode schizophrenia patients (Kahn and Sommer 2015).
There were some strengths of our study. In children, the duration of disease was shorter and the allostatic load was lower compared with adults; therefore, children might be the optimum study group to identify the underlying inflammatory mechanism in EOS patients (Kapczinski et al. 2008). Studies performed on children might provide better information on the mechanism of the association between psychiatric disease and inflammation since the number of confounding factors was lower (Mitchell and Goldstein 2014).
The present study had some limitations. First, the cross-sectional design of this study confined the measurement of cytokines at a single time point. Second, the small study sample did not sufficiently represent the first episode of EOS patients due to the fact that the study sample was limited to patients who were admitted to a university hospital clinic. Third, although the patient group was determined randomly, the gender distribution, which was restricted in this study, was different from the literature. Finally, in regression analysis, amount of smoking, and duration of untreated psychosis were not taken into consideration.
Conclusions
In conclusion, we identified no significant differences between the IL-2, TNF-α, IFN-γ, IL-4, IL-10, IL-17A, and IL-6 levels of first episode EOS patients and the control subjects. However, a correlation was observed between certain clinical variables and cytokine levels.
Clinical Significance
These findings might suggest that some immunological processes might have a role in the pathophysiology of the disease. Cytokine levels might also be an indicator for the progress of the disease. However, our findings should be confirmed with further studies.
Footnotes
Acknowledgments
The authors would like to thank Dr. Hüseyin Aktaş and Dr. Rümeysa Alaca, and the patients and their parents for taking part in this study.
Disclosures
No competing financial interests exist.