
Abstract
Introduction:
Although widely used for the treatment of attention-deficit/hyperactivity disorder (ADHD) across the life span, the effects of methylphenidate (MPH) on the brain are not completely understood. Functional neuroimaging techniques may help increase knowledge about the mechanisms of MPH action.
Objective:
To evaluate changes in functional connectivity patterns of the default mode network (DMN) in children with ADHD following long-term treatment with MPH.
Methods:
Twenty-three right-handed treatment-naïve boys with ADHD underwent a protocol of intrinsic functional connectivity before and after 6 months of treatment with MPH. Functional connectivity was analyzed using a region of interest (ROI) approach and independent component analysis (ICA).
Results:
ROI analyses showed no significant changes in connectivity between regions of the DMN following treatment, with a relatively small increase in the anterior–posterior connectivity of the network. ICA revealed a significant increase in connectivity between the left putamen and the DMN (p < 0.001, corrected). There was a correlation between the reduction of symptoms and the increased connectivity between the putamen and the DMN after treatment (rho = −0.65, p = 0.017).
Conclusion:
Dysfunctions in cortical–subcortical circuits have often been associated with the pathophysiology of ADHD. Our findings suggest that effective treatment with MPH in children with ADHD may affect brain functioning by increasing connectivity between the DMN and subcortical nuclei.
Introduction
A
While the exact pathophysiology of ADHD is not completely understood, treatment with stimulants has long been recognized to attenuate symptoms of inattention and hyperactivity in children with the disorder (Taylor et al. 2004, Pliszka et al. 2007) and their efficacy and tolerability have been reported in several studies (Rappley 2005). Stimulants are recommended as first-line pharmacological treatment by major guidelines (Atkinson and Hollis 2010, Subcommittee on Attention-Deficit/Hyperactivity et al. 2011, Bolea-Alamanac et al. 2014) in children with ADHD, with an efficacy of ∼70% in symptom reduction (Swanson et al. 1991, Greenhill et al. 2002). Their action in the brain is believed to occur through the modulation of both norepinephrine (NE) and dopamine (DA). Methylphenidate (MPH) acts primarily by dose-dependent blockage of striatal DA transporter (Volkow et al. 1998), with a lesser effect on the NE transporter (Findling 2008). The dopaminergic and noradrenergic systems are responsible for mediating selective attention (noradrenergic neurons) and motivation (dopaminergic neurons) (Volkow et al. 2005), while DA is also known to decrease background firing of striatal neurons, which increases the signal-to-noise ratio in target neurons (Kiyatkin and Rebec 1996). Therefore, it is speculated that by amplifying striatal DA signal, MPH would improve attention and decrease distractibility in ADHD (Volkow et al. 2005).
In an attempt to elucidate the underlying effects of stimulants in ADHD, the neuroimaging literature is rapidly growing. Initially, positron emission tomography was used to investigate the effects of MPH in the human brain and evidenced increased concentration of DA in the striatum (Volkow et al. 1995, 2001, 2002, 2007, Rosa-Neto et al. 2005). With a different approach, several task-based functional magnetic resonance imaging (fMRI) studies have focused on the acute and chronic effects of stimulants in patients with ADHD, but findings have been inconsistent (Rubia et al. 2014).
Acute treatment with MPH in children with ADHD has been associated with increased task-based activation in the inferior frontal cortex (IFC), parietal regions, cerebellum, and striatum (Rubia et al. 2009a, 2009b, 2011a, 2011b). A systematic review of task-based fMRI studies following a single dose of MPH in children with ADHD showed changes in brain activation within frontal lobes, basal ganglia, and cerebellum (Czerniak et al. 2013). In patients chronically treated with MPH, a study found significant enhancement of bilateral medial frontal activation during an emotional Stroop test (Posner et al. 2011). A recent task-based fMRI meta-analysis of children and adolescents with ADHD treated with MPH found significantly increased activation in right IFC, insula, and bordering superior temporal lobe. These brain regions, involved in cognitive control and salience detection, have been found to be underactivated among patients with ADHD when compared with healthy controls (Rubia et al. 2014).
An alternative approach to task-based studies to investigate the brain relies on measures of functional connectivity obtained from resting-state scans. Whereas task-based approaches provide a strategy to map neuropsychological processes to brain areas activated during performance, resting-state analyses can reveal normal or aberrant interactions between large, distributed brain networks, such as the default mode network (DMN), which includes the posterior cingulated cortex (pCC), the inferior parietal, and the medial prefrontal cortex. Resting-state protocols are particularly agreeable to patients, especially children, as they are relatively easy to perform, require minimal cooperation, and are more easily reproducible, allowing for the aggregation of data across sites. Moreover, the undirected task-independent nature of resting-state protocols has attracted large attention in the fields of psychiatry and neurology, which ultimately led to a conceptual shift in the investigation of neuropsychiatric disorders (Kelly et al. 2012).
One recent study with a small sample of children with ADHD found a failure of synchronization between two large brain networks, the task-positive network and the DMN, which could be involved in the moment-to-moment variability. After treatment with MPH, the variability was reduced and the variability/DMN correlation was abolished (Querne et al. 2014). Another study, a placebo-controlled trial of acute treatment with MPH, based on resting-state fMRI (rs-fMRI), found that all fronto-parieto-cerebellar dysfunctions in boys with ADHD were normalized after treatment with MPH. Furthermore, the neuroimaging response data following a single dose of MPH significantly predicted the clinical response after chronic treatment (An et al. 2013). Nevertheless, resting-state functional connectivity is still a growing field in ADHD and there are not enough data to predict brain connectivity modifications along neurodevelopment or following treatment with MPH. While most studies so far reported an increase in intra-DMN connectivity in typically developing brains when compared with children with the disorder, one trial also found that affected children had increased activity in a DMN connection known to decrease with development (Fair et al. 2010).
Thus, given the paucity of rs-fMRI studies evaluating the DMN after long-term treatment with MPH, we applied complementary strategies to assess intrinsic functional connectivity changes. Seed-based analysis, which relies on a priori based assumptions of dysfunctional brain areas, has inconsistent findings throughout the literature. Thus, we also conducted an independent component analysis (ICA), a data-driven approach, hypothesizing that it would indicate changes in the intra-DMN connectivity following chronic treatment with MPH, especially concerning areas previously shown to be affected by stimulants, such as the frontoparietal cortex, basal ganglia, and cerebellum.
Methods
Participants
Participants were recruited from the community through the local press. Screening for ADHD symptoms was made by telephone. Potential candidates were called to the ADHD outpatient clinic at Hospital de Clínicas de Porto Alegre for a detailed semistructured interview using the Schedule for Affective Disorders and Schizophrenia for School-Aged Children, Kiddie-SADS—Lifetime Version (K-SADS-PL) (Kaufman et al. 1997). Following the clinic standard protocol, parental and teacher reports were obtained using the SNAP (Mattos et al. 2006) as well as the Teacher Report Form from the Child Behavior Checklist (CBCL) (Bordin et al. 2013). The Wechsler Intelligence Scale for Children (WISC-III) (Weschler 1991) was applied, as were the following neuropsychological tests: Stroop Test for Colors and Words (Stroop 1935), Continuous Performance Test (CPT-II) (Conners and Staff 2000), and Trail Making A and B (Reitan 1992). Possible side effects during treatment were assessed through Barkley's Side Effects Rating Scale (SERS) (Barkley et al. 1990). Social and demographic variables were also collected.
Inclusion criteria for this study were the following: (1) male gender; (2) age ranging from 8 to 10 years; (3) right handed; (4) no history of previous use of psychotropic medication; (5) not currently undergoing psychiatric, psychological, or any pharmacological or psychotherapeutic treatment; (6) residing in the metropolitan area; (7) enrolled and attending regular school; and (8) absence of chronic diseases requiring continuous medication. Exclusion criteria were the following: (1) impossibility or nonagreement by the family to attend monthly appointments; (2) impossibility or nonagreement to undergo magnetic resonance imaging; (3) contraindication, impossibility, or nonagreement to receive medication; (4) intellectual disability (IQ <70); and (5) comorbid diagnoses of neurological or psychiatric disorders, with the exception of externalizing disorders (oppositional defiant disorder [ODD] or mild conduct disorder) and anxiety disorders (as long as considered less severe than ADHD by the treating clinician). Learning disorders did not constitute an exclusion criterion per se.
Clinical assessment
After the initial assessments, the study coordinator interviewed the participants and their symptoms were discussed in a clinical committee chaired by L.A.R. to confirm the diagnosis of ADHD. A baseline severity score was determined based on the intensity and number of symptoms in the SNAP; this measure was repeated after 3 and 6 months of treatment as the primary clinical outcome. Besides the aforementioned measures, patients were also reevaluated once a month by the study nurse. Children's Global Assessment Scale (CGAS) and Clinical Global Impressions (CGI) (Shaffer et al. 1983) were recorded at baseline and after 6 months as secondary clinical outcome measures.
Intervention
As recommended by clinical guidelines, all patients received psychoeducation about ADHD and parents were instructed about symptom management strategies. After the first MRI scan, each participant was started on 5 mg dosage of immediate-release MPH; dosages were adjusted individually, on a monthly basis, aiming at a target dosage of 1 mg/kg/day or until there was no room for improvement. Symptoms were reevaluated after 30 days and 3 and 6 months. During follow-up visits, blood pressure, cardiac frequency, and SERS were checked; teacher reports on symptom progression were collected after 90 and 180 days of treatment.
Neuroimaging
MRI scans were performed at the Radiology Service of the Hospital de Clínicas de Porto Alegre at two moments: before study entry (medication-free) and after 6 months of medication use (standard chronic treatment). A 1.5T MRI scanner (Philips Medical System) with an 8-channel head coil was used to acquire the images. Initially, T1-weighted structural images were collected with the following sequence parameters: 170 slices with a matrix size of 232 × 256 with 1 mm3 voxels, TR/TE = 4/8.7 ms. Functional images were collected following structural images. The functional T2* sequence had the following parameters: EPI, 34 interleaved slices, slice thickness 3.5 mm, TE/TR = 30/2500 ms, flip angle = 80o, 150 volumes, with a total time of 6 minutes and 20 seconds. The same protocol was used in both occasions.
Neuroimaging processing
Functional images were processed using a mixture of freeware packages, including the Analysis of Functional NeuroImages (Cox 1996), and FMRI of the Brain Software Library (Smith et al. 2004). Initially, time series images were temporally interpolated to correct for slice-time acquisition differences, motion corrected, spatially blurred using an 8-mm Gaussian full-width half-maximum kernel, and then normalized to a 3 mm3 standard stereotaxic coordinate space (MNI152) using the subjects' T1 anatomical image as a reference. Additionally, the subject's structural images were segmented into maps of white matter, gray matter, and cerebral spinal fluid (CSF), with the resultant CSF and white matter masks used to obtain an average time series for these tissues. The six motion parameters and averaged time series for white matter and CSF were then entered into a linear regression against the extended resting-state time series to remove the variance associated with each of these variables (Fox et al. 2005).
A seed-based functional connectivity analysis was performed, placing regions of interests (ROIs) in locations defined by Fox et al. (2005) and Supekar et al. (2010). The following seed (radius = 6 mm) locations were used: pCC, ventromedial prefrontal cortex (vmPFC), right (rIPL) and left (lIPL) inferior parietal lobe, right frontal eye field (rFEF), right intraparietal sulcus (rIPS), right temporoparietal junction (rTPJ), right ventral frontal cortex (rVFC), right medial frontal gyrus (rMFG), and right inferior frontal gyrus (rIFG). Within these seeds, the average time series of the functional data was extracted and later used for correlation analysis. The resulting correlations were subsequently converted to a z-score to be used in statistical analysis using Fisher's r to z method.
An ICA was also performed by decomposing the data matrix into a set of independent time series with their corresponding spatial maps. Each of these components consecutively accounts for the greatest amount of variance in the data and represents a functionally discrete network (Calhoun et al. 2001, Beckmann 2012).
With MELODIC (3.10), which is a toolbox within FSL (Beckmann et al. 2005), we performed an ICA with these data. Specifically, functional data from both visits were entered into the analysis. The software defined the number of independent components to be generated. Subject-level components were subsequently used for statistical analysis.
For quality control purposes, all images were initially assessed regarding head movement during acquisition. Image data of four pretreatment participants were discarded due to excessive head motion, defined as an average dislocation of >0.20 mm per volume or more than 100 micromovements (Van Dijk et al. 2012).
Statistical analyses
SPSS version 20.0 was used to describe and compare clinical and connectivity scores' means, employing Student's t-test for continuous or Fishers' exact test for categorical variables. Associations between continuous variables were investigated through Spearman's rank correlation coefficient, according to data distribution.
The primary outcome was analyzed using a mixed-effects model. For every analysis, treatment duration (initial vs. 6 months) was established as a factor or fixed effect. In addition, for the multivariate analyses of treatment effect over connectivity, clinical variables regarding treatment response were defined as dependent variables and the connectivity measures as covariables. Group analysis was performed with a linear mixed-effects modeling approach using 3dMLE (Chen et al. 2013). Statistical significance was set at 5% and corrections for multiple comparisons were performed with 3dClustSim (toolbox of AFNI), which estimates the probability of false-positive clusters for different levels of statistical significance.
The ethics committee of Hospital de Clínicas de Porto Alegre approved this study, which is also registered at clinicaltrials.gov under the identifier NCT01228604. The primary caregivers signed consent forms with verbal assent from all the children.
Results
Sample characteristics
A total of 23 treatment-naïve right-handed boys, with ages ranging between 8 and 10 years, were recruited. Baseline characteristics of the final sample are presented in Table 1. All patients presented at least five symptoms of inattention; two patients did not report any symptoms of hyperactivity. There was a significant agreement between family and school reports, with SNAP scores from parents and teachers showing a positive correlation (r = 0.619; p = 0.018), although parents reported more hyperactive symptoms (mean 2.02 vs. 1.52; p = 0.007). Comorbid ODD was diagnosed in part of the sample; other diagnoses are presented in Table 1. Although no formal diagnoses of learning disorders were conducted, 19 patients (82.6%) had no history of grade retention, while three repeated 1 year and one patient had a history of repeating two school years.
CPT, Continuous Performance Test; SNAP-IV, Swanson, Nolan, and Pelham Scale–version IV; pCC, posterior cingulated cortex; vmPFC, ventromedial prefrontal cortex; rIPL, right inferior parietal lobe; lIPL, left inferior parietal lobe; rFEF, right frontal eye field; rIPS, right intraparietal sulcus; rTPJ, right temporoparietal junction; rVFC, right ventral frontal cortex; rMFG, right medial frontal gyrus; rIFG, right inferior frontal gyrus. The coordinates follow pre-established locations based on the existing literature (Fox et al. 2005; Supekar et al. 2010).
Response to intervention
Of the 23 participants, 21 completed 6 months of treatment. Two patients were lost to follow-up (moved out of town). Clinical evaluation was performed at 1, 3, and 6 months of follow-up. Table 1 presents the average symptom reduction during treatment based on SNAP scores. Overall, clinical response was satisfactory, with some patients showing significant symptom reduction, while others had only a minor improvement, according to parental and school reports. By the end of the study, two patients were considered nonresponders for presenting <20% symptom reduction. Group clinical improvement was also confirmed through CGAS (55.55 to 73.72; p < 0.001) and CGI scores (4.90 to 3; p < 0.001). In addition to the symptom-based clinical improvement, neuropsychological assessment showed a positive response in most of the tests. Tests included in the neuropsychological battery are listed in Table 1 with their average scores before and after treatment.
At the end of the study period, patients were taking between 15 and 40 mg/day of MPH, with an average of 28.1 mg/day and a median of 30 mg/day. The most common side effects observed were loss of appetite and apathy. Loss of appetite was accompanied by weight reduction with a mean BMI reduction by the end of 6 months (18.1 kg/m2 vs. 17.2 kg/m2; p = 0.002). Dosages were adjusted individually by the attending physician, following our program's standard protocol. Treatment response and adverse effects were taken into consideration when adjusting the medication. Our average final dose was very close to the expected target dose.
Intrinsic brain connectivity
First, changes in brain connectivity were assessed using specific locations and coordinates previously defined in the literature as ROIs within the DMN (Fox et al. 2005, Supekar et al. 2010). We compared intra-DMN connectivity, before and after the treatment, using a set of seeds within this network (Table 1). Results showed no significant difference, except for a trend of increased connectivity between the pCC and the vmPFC.
Connectivity maps were then built to investigate potential changes in functional connectivity between specific seeds within the DMN and the whole brain. Based on data from the literature and the results of our previous test, we built connectivity maps by placing seeds over the pCC and the vmPFC. Again, we found no significant difference on the connectivity maps before and after treatment from either ROI.
Finally, we employed a more explorative data-driven approach to assess potential changes in functional connectivity. ICA revealed 18 independent components from the functional imaging sets. They were all visually inspected and some represented networks of interest (such as executive control, motor, and DMN), while others were apparently only background noise. The DMN component was visually identified based on previous studies using ICA (Beckmann et al. 2005). We compared the DMN component before and after treatment using a mixed-effects model (3dMLE) that accounts for variations both within and between subjects. Results showed a significantly increased connectivity between the DMN and the left putamen (p < 0.001, corrected) after treatment, as shown in Figure 1. Additionally, Pearson's analysis showed a moderate correlation between patients' individual increase in connectivity in the putamen and their clinical improvement, as measured by the SNAP (rho = −0.646; p = 0.017).
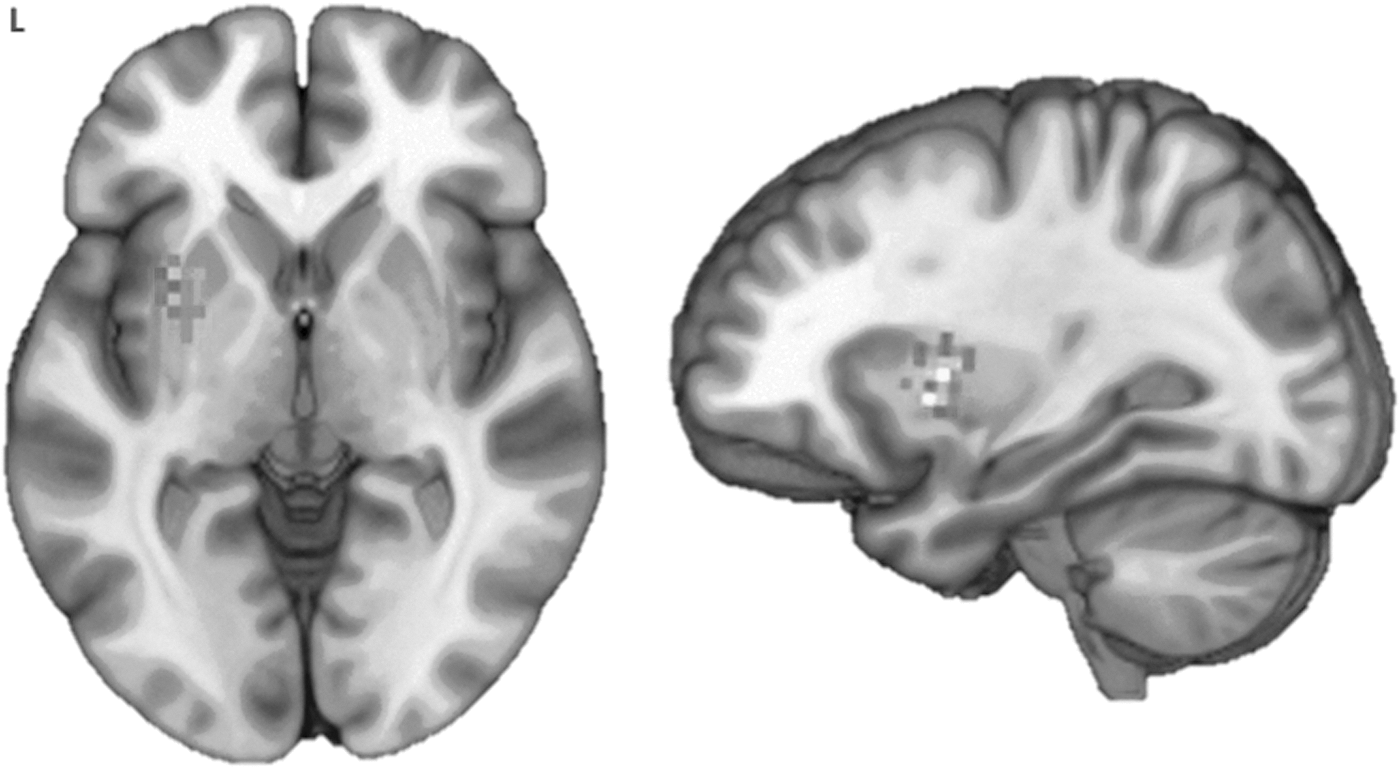
Increase in connectivity between the DMN and the left putamen before and after treatment (p < 0.001, corrected). DMN, default mode network.
Discussion
A comparison of intrinsic brain connectivity in children with ADHD, before and after treatment with MPH, showed an increased functional connectivity between the DMN and the left putamen. Interestingly, this finding was corroborated by a significant positive correlation between clinical improvement ratings and connectivity intensity. No interaction effects between brain connectivity and response to treatment were identified.
These results derive from a very homogeneous sample, exclusively comprising right-handed boys, ranging from 8 to 10 years of age. None of them had a history of previous medical treatment with psychotropic medication. Treatment was carried out for 6 months with no cost for the patients, with compliance monitored by monthly appointments in the research clinic.
In this study, we began by testing specific regions based on the available literature on resting-state functional connectivity in ADHD. None of these theoretical expectations of changes in connectivity was confirmed, and it was only the data-driven approach that yielded positive results. Thus, although our results must be interpreted cautiously, it is clear that such atheoretical approaches to neuroimaging data are relevant for generating new conceptual hypotheses and investigating neurobiological phenomena still not fully understood.
The increase in connectivity between the DMN and the left putamen after treatment with MPH could be related to the dopaminergic effect of the drug (Volkow et al. 2001, 2002, 2005). Even though the precise mechanism of clinical improvement in ADHD is not completely defined, one suggested mechanism points to the role of DA in the reinforcement of active synaptic connections and in the inhibition of inactive ones, altering the signal-to-noise ratio in corticostriatal circuits (Bamford et al. 2004a, 2004b), and thus possibly improving network functioning. However, the clinical significance of our finding in terms of symptom improvement is yet to be elucidated. Due to the lack of previous data, any conclusions about whether treatment modifies the ADHD brain to make it more similar to a healthy one would be highly speculative.
A number of limitations should be considered when interpreting our findings. First, our relatively small sample size might be responsible for negative findings due to type II errors. Second, the absence of a control group without treatment—a problem that affects the majority of long-term treatment studies—limits the significance of our results and we cannot eliminate the potential interference of placebo effects from our results. Third, imaging acquisition was performed in a 1.5 Tesla machine.
Conclusions
In summary, the intrinsic brain connectivity in boys with ADHD revealed a fragmented DMN architecture, with relatively little modification following long-term treatment. This may be a reflection of the specific brain connectivity of the disorder, an age-related transitory nonpathological state, or even the conjunction of both. Long-term treatment with a stimulant drug produced an increase in cortico-subcortical connectivity between the DMN and the left putamen. Of relevance, clinical improvement following treatment was also associated with increased connectivity. These results are in accordance with the propositions of potentially reversible network dysfunctions with treatment and also imply a potential mechanism involved in the pathophysiology of ADHD. Further studies are warranted to confirm the association between clinical improvement and brain connectivity changes in ADHD.
Clinical Significance
Long-term treatment with usual dosages of MPH produces little change in intrinsic functional brain connectivity, particularly in the DMN, a large-scale brain network that is often implicated in resting-state fMRI studies of ADHD and other neuropsychiatric disorders. In our sample of young treatment-naïve boys with ADHD, the anterior and posterior nodes of the DMN were loosely connected before treatment, and this fragmentation was not significantly modified after 6 months of regular treatment. Nevertheless, an increase in the connectivity with the putamen was observed, suggesting that (at least in part) an increase in cortico-subcortical connectivity might underlie the clinical response observed with treatment.
Footnotes
Acknowledgment
Methylphenidate used by patients during this study was kindly offered by Novartis free of charge.
Disclosures
Dr. C. Kieling received authorship royalties from publishers, Artmed and Manole. Dr. L.A. Rohde was on the speakers' bureau/advisory board and/or acted as consultant for Eli-Lilly, Janssen-Cilag, Novartis, and Shire in the last 3 years. He receives authorship royalties from Oxford Press and ArtMed. He also received travel awards for taking part in 2014 APA and 2015 WFADHD meetings from Shire. The ADHD and Juvenile Bipolar Disorder Outpatient Programs chaired by him received unrestricted educational and research support from the following pharmaceutical companies in the last 3 years: Eli-Lilly, Janssen-Cilag, Novartis, and Shire. For all other authors, no conflicts of interest exist.