
Abstract
Objective:
To explore the potential benefits of varenicline (CHANTIX®), a highly specific partial agonist of neuronal α4β2 nicotinic acetylcholine receptors (nAChR), for autistic symptoms, and present resulting biochemical changes in light of dopamine-related genotype.
Methods:
The clinical and biochemical changes exhibited by a 19-year-old severely autistic man following the use of low-dose varenicline in an ABA experiment of nature, and his genotype, were extracted from chart review. Clinical outcome was measured by the Ohio Autism Clinical Impression Scale and 12 relevant urine and saliva metabolites were measured by Neuroscience Laboratory.
Results:
With varenicline, this patient improved clinically and autonomic biochemical indicators in saliva and urine normalized, including dopamine, 3,4-dihydroxyphenylacetic acid (DOPAC), epinephrine, norepinephrine, taurine, and histamine levels. In addition, with varenicline, the dopamine D1 receptor (DRD1) antibody titer as well as the percent of baseline calmodulin-dependent protein kinase II (CaM KII) activity dropped significantly. When varenicline stopped, he deteriorated; when it was resumed, he again improved. Doses of 0.5, 1, and 2 mg daily were tried before settling on a dose of 1.5 mg daily. He has remained on varenicline for over a year with no noticeable side effects.
Conclusion:
This report is, to the best of our knowledge, only the second to demonstrate positive effects of varenicline in autism, the first to show it in a severe case, and the first to show normalization of biochemical parameters related to genotype. As with the previous report, these encouraging results warrant further controlled research before clinical recommendations can be made.
Introduction: Theory
A
Recent efforts have attempted to identify alterations in neuronal nicotinic acetylcholine receptors (nAChRs), ion channels responsible for regulating the release of acetylcholine, dopamine, γ-aminobutyric acid (GABA), glutamate, and serotonin in the central nervous system, as biomarkers for ASD (Anand et al. 2011). Neuronal nAChRs exist typically as heteropentamers with alpha (α2–α10) and beta (β2–β4) subunits. These channels have been implicated in a broad range of neurophysiological processes, including reward, analgesia, anxiety, affect, locomotion, attention, mood, learning, memory, and executive function (Miwa et al. 2011). In particular, the α4β2 nAChR subtype, important for neuroprotection and synaptic plasticity (McGehee 2002), has been hypothesized to be a useful therapeutic target, based on extensive loss of these channels in the postmortem cortex and cerebellum of individuals with autism (Perry et al. 2001).
Varenicline (CHANTIX®) is a drug approved by the Food and Drug Administration (FDA) for smoking cessation. It acts as a full agonist of the α7 nAChR (Mihalak et al. 2006); however, when administered at the lower doses recommended for antismoking therapy, varenicline displays a higher specificity for the α4β2 subtype as a partial agonist (Niaura et al. 2006). Few sympathetic and parasympathetic complications result from the cross activation of ganglionic α3α5β4 nAChRs (Coe et al. 2005). As a partial agonist, varenicline provides chronic nondesensitizing low-level channel activation of α4β2 nAChRs (Papke et al. 2011), making it a potential treatment for ASD. An FDA public health advisory warned of a potential increase in suicidal thoughts and actions with the use of varenicline; however, this increase might be due to the overlap of excessive smoking with neuropsychiatric conditions, including schizophrenia (Adler et al. 1993; Dalack et al. 1999), which have high suicide rates. Kotz et al. (2015) reviewed 106,759 smokers who were prescribed nicotine replacement, 6,557 prescribed bupropion, and 51,450 prescribed varenicline and found considerably lower rates of cardiovascular events, depression, and self-harm with varenicline. The prevalence of smoking in ASD is very low (Bejerot and Nylander 2003), possibly because the loss of α4β2 nAChRs occurs early in development.
A case report of a 9-year-old boy with high-functioning autistic disorder (Arnold et al. 2013) found clinically significant improvement from varenicline 0.5 mg/day in an ABA experiment of nature. We report, in this study, another case suggesting that varenicline or drugs with related properties that target α4β2 nAChRs should be investigated for treating core deficits of ASD. In particular, this report is to the best of our knowledge, the first to show normalization of biochemical parameters related to genotype.
Catechol-O-methyltransferase (COMT, EC 2.1.1.6) is one of several enzymes that degrade catecholamines. In regulating both dopamine and norepinephrine, COMT aids in the efficient functioning of the prefrontal cortex, a region of the brain involved in personality, planning, inhibition of behaviors, emotion, and abstract thinking. A functional single-nucleotide polymorphism (SNP) of the gene for COMT, referred to as rs4680, reflects a valine (Val) versus methionine (Met) mutation at position 158 (Val158Met). It has been postulated that people with the Val alleles have an increased COMT activity and thus lower prefrontal extracellular dopamine compared to individuals with the Met substitution (Stein et al. 2006). Met homozygosity catalyzes dopamine degradation at approximately one-fourth the rate of its Val counterpart. In the warrior/worrier hypothesis, individuals with Val alleles may have an advantage processing negative stimuli (warrior strategy), whereas those with Met alleles may have an advantage in memory and attention (worrier strategy) (Stein et al. 2006). Those heterozygous for rs4680 may have a more balanced personality. Interestingly, a meta-analysis of 51 studies comprising 13,894 schizophrenic patients and 16,087 controls revealed a small, but significant protective effect of heterozygosity (Costas et al. 2011).
Another variant in the COMT gene, referred to as rs4633, occurs at codon 62 and does not result in a change in the amino acid sequence. Recent work has identified rs4633 as a determining factor in the efficiency of COMT translation (Tsao et al. 2011). In rs4633, the substitution of 166C to 166T resulted in overall higher levels of COMT expression. This is the result of an increase in the number of favorable isoenergetic conformational states in the messenger RNA (mRNA) transcript.
Dopamine receptor D2 (DRD2) is a G-protein coupled receptor located on postsynaptic dopaminergic neurons responsible for the inhibition of adenylyl cyclase. Due to its importance in reward-mediating mesocorticolimbic pathways, DRD2 is the target of many antipsychotics. An isoform of DRD2, termed D2-short (D2S), acts as a dopamine autoreceptor located on the presynaptic membrane where it modulates both dopamine synthesis and release (Beaulieu and Gainetdinov 2011). The DRD2 gene and the ankyrin repeat, and kinase domain containing 1 gene (ANKK1, EC 2.7.11.1) are closely linked, both located on chromosome band 11q23.1, and thus are often coinherited (Neville et al. 2004). One such variant, the rs1800497 SNP, is located in the ANKK1 gene, but is responsible for altering the expression of the DRD2 gene and thus the DRD2 protein. Unfortunately, the complexity behind the rs1800497 location and effects extends into the nomenclature surrounding it. The DRD2 gene has the allelic designations A1 and A2. Based on the direction of the reference strand of DNA, the A1 allele is equivalent to the A or T nucleotide, whereas the A2 allele is equivalent to the G or C nucleotide. Presence of the A1 allele in rs1800497 has been associated with a reduction in the number of dopamine binding sites in the striatum (Pohjalainen et al. 1998). In addition, A1 carriers were found to have a 30%–40% reduction in DRD2 density when compared to A2 homozygotes (Ritchie and Noble 2003).
Case Report
A 19-year-old man with autistic disorder diagnosed at age 2 had an uneventful gestation and an elective Caesarean section birth. He is a middle child with two neurotypical sisters. At age 2, he manifested delayed language, stereotyped movements and play, sensory intolerances, poor eye contact, poor social skills, head banging, lining up objects, and poor imitation skills. After a 2-day evaluation at Boston Children's Hospital, he received the diagnosis of autism. Shortly after, he started intensive behavior modification therapy. Due to his severe behavioral symptomology and limited communication ability, no IQ testing has been able to evaluate his cognitive level. He underwent multiple biomedical interventions, many of which were based on the recommendations of Defeat Autism Now (DAN) doctors. These included gluten-free/casein-free diet, carbohydrate-specific diet, intravenous (IV) secretin, IV Glutathione, IV N-acetyl cysteine, intranasal oxytocin, chelation therapy with transdermal 2,3-dimercaptopropane-1-sulfonate (DMPS), and hyperbaric oxygen therapy. Despite these interventions, his progress was very slow, and more importantly, his aggressive behavior and self-injury significantly worsened over time.
He started the following psychiatric medications primarily to control his severe anxiety, aggressive behavior, and obsessive-compulsive disorder (OCD): risperidone, ziprasidone, diazepam, lorazepam, clonazepam, alprazolam, haloperidol, lamotrigine, loxapine, gabapentin, lithium, memantine, and prednisone, all with little success. He finally showed some improvement with a combination of sertraline, lurasidone, clonidine, guanfacine XR, baclofen, and quetiapine, continued to the present.
Methods
The patient's parents had read the first case report (Arnold et al. 2013) about the use of varenicline and in desperation they decided they wanted a trial. They discussed it with his psychiatrist, who agreed to try it cautiously. He started varenicline 0.5 mg daily for 1 week before increasing the dose to 1 mg daily. After another week, it was increased to 1 mg twice daily. The patient's parents noted improvement in aggressive behavior and anxiety after only 3 days on the lowest dose. The second daily dose was decreased from 1 to 0.5 mg after the patient demonstrated gestures of headache by hitting his forehead while taking 1 mg twice daily.
Despite his overall improvements, his psychiatrist decided to stop varenicline because of concerns about the unknown potential long-term effects. After only 2 days off varenicline, the aggressive behaviors returned. Therefore varenicline was resumed. Since then, he has remained on varenicline 1 mg in the AM and 0.5 mg in the PM with continued improvements and no side effects. Throughout this trial with varenicline, all other medications for anxiety, aggression, and OCD remained unchanged as well as the behavioral programming. His scores on the Ohio Autism Clinical Impressions Scale (OACIS; Butter and Mulick 2006), are shown in Table 1 for before varenicline and at each dose (0.5, 1, 2, 1.5 mg/day), after stopping varenicline, and after resuming varenicline 1.5 mg/day. It should be noted that the OACIS is intended to be a clinician-rate scale and there is no precedent for caregiver ratings. The OACIS form had been supplied to the parents as a convenient way to track the child's progress. OACIS-I, in contrast to a CGI-I, is an 8-point scale in which 5 is no change and 3 is definite improvement.
The OACIS is intended to be a clinician-rate scale and there is no precedent for caregiver ratings. The OACIS form had been supplied to the parents as a convenient way to track the child's progress. Note that the OACIS-I, in contrast to a CGI-I, is an 8-point scale in which 5 is no change and 3 is definite improvement.
OACIS, Ohio Autism Clinical Impressions Scale.
Biochemical and genetic analyses
The patient reported in this study is heterozygous for both the COMT SNPs, rs4680 and rs4633, as well as the ANKK1/DRD2 SNP, rs1800497 (Table 2). This suggests that he has some, but not severe, difficulty in the regulation of dopamine. In particular, it appears that he has difficulty with the reuptake and breakdown of dopamine, resulting in elevated levels of dopamine in the synaptic cleft. Throughout the years, the patient has had multiple neurotransmitter evaluations using urine samples through Neuroscience laboratory (Table 3). Values shown in bold demonstrate values higher than the optimal range, while those shown in italics demonstrate values lower than the optimal range. It is important to note that the reference range changed significantly between 2011 and 2014. The dopamine imbalance predicted from the genetic studies is apparent: He experienced chronic elevated levels of dopamine and irregular levels of 3,4-dihydroxyphenylacetic acid (DOPAC), a metabolite of dopamine, as well as elevated levels of both epinephrine and norepinephrine before commencing varenicline, suggesting a chronic elevation in the sympathetic tone.
Bold represents above normal range; italics represents under normal range.
He incurred neurologic Lyme disease in 2010 and has been treated with standard antibiotics, including Zithromax and Doxycycline, with limited benefits. In November 2013, a Cunningham panel by Moleculera laboratory found significant abnormalities as shown in Figure 1. This panel includes four enzyme-linked immunosorbent assays used to measure antibody titers against four neuronal antigens present in the brain: Dopamine D1 Receptor (DRD1), Dopamine D2L Receptor (DRD2L), Lysoganglioside-GM1 (LYSO-GM1), and Tubulin (TUB). A fifth assay in the Cunningham panel provides a numeric score reflecting the percent of baseline calmodulin-dependent protein kinase II (CaM KII) activity in a human neuronal cell line. The same test repeated in June 2014, while taking varenicline, found a significant reduction in the production of antibodies, supporting a role of varenicline in stabilizing the immune system (Fig. 1). Unfortunately, the test for DRD2L was no longer available for comparison at retest.
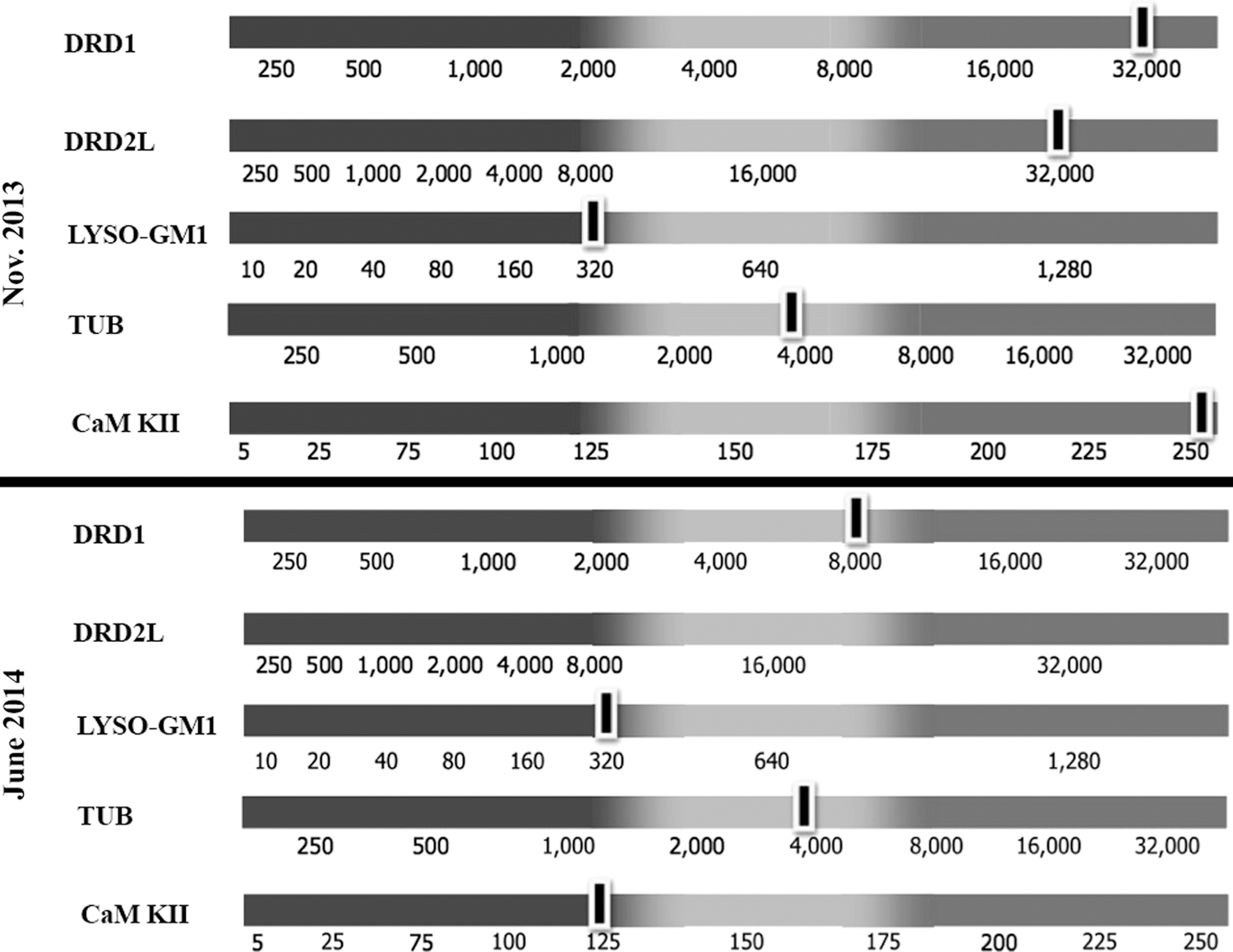
Cunningham panel by Moleculera laboratory completed before varenicline (November 13, 2013) and after varenicline (June 1, 2014).
Discussion
To the best of our knowledge, this is only the second report of an individual with autism treated with varenicline. The first report was of a high-functioning 9-year old and this one was of a severely impaired 19-year old. In both cases, there was an ABA experiment of nature in which after initial improvement, varenicline was stopped because of concerns about potential long-term effects, then after deterioration, varenicline was resumed with resumption of improvement. In both cases, the parents elected to continue varenicline as they were impressed with the results and noticed a drastic worsening of symptoms to prevarenicline levels after stopping the medication. This patient has remained on varenicline for over a year with no noticeable side effects. This case advances the knowledge base by demonstrating the biochemical effects and expected interaction with genome, particularly the dopamine effects. Dopamine is of particular interest, as prolonged elevated levels have been known to result in neurotoxicity.
As a partial agonist of α4β2 nAChRs, varenicline may aid in reestablishing balance in the dopamine pathway through chronic channel activation at low levels. In an animal model, use of varenicline was also found to significantly increase striatal DRD2, with the effects being long lasting (Crunelle et al. 2011). In the patient presented in this study, dopamine imbalance was predictable from genetic studies. With varenicline, dopamine levels decreased to normal and DOPAC levels stabilized. He had experienced imbalanced frequently elevated levels of both epinephrine and norepinephrine before varenicline, suggesting a chronic elevation in the sympathetic tone. The severe aggressive behavior and anxiety felt by the patient may have been due to this sustained state of “fight or flight.” With varenicline, epinephrine levels stabilized and norepinephrine levels decreased. Other interesting results following the use of varenicline include the reduction of taurine levels, the elevation of glutamate and glycine levels, as well as the equilibration of histamine levels. Little is known about the effect of elevated taurine levels; however, taurine is recognized as protective in nature (Timbrell et al. 1995). As elevated levels of glutamate can be potentially neurotoxic, it is important to determine if the levels remain elevated with prolonged use of varenicline by repeat testing. Involved in the production of inflammation, histamine provides some insight into the overall condition of the immune system. In recent years, the connection between the sympathetic nervous system and chronic inflammation has developed significantly (Straub et al. 2006; Jänig 2014). Therefore, it is possible that in reducing the sympathetic tone, varenicline was able to also aid in the equilibration of the immune system as observed in the Cunningham panel (Fig. 1).
There appears to be a U-shaped response curve in this 165-lb man, with optimal results at 1–1.5 mg/day and loss of benefit at 2 mg/day. This would be consistent with the good response to 0.5 mg/day by the 85-lb 9-year old in the first case report. Although we cannot be sure from two cases, there appears to be a suggested dose range of about 1 mg/day for adults with ASD and proportionately less for children.
The parents continue to share the prescriber's concerns about long-term safety and hope that this case study will promote controlled research into the potential benefits and safety of varenicline for treatment of ASD. As with any open trial, there is always the possibility of placebo effect being responsible for the benefits observed. This is especially true in cases of autism as parents are desperate to find improvement for their children. Ultimately, it is necessary to evaluate the efficacy of varenicline with a placebo-controlled randomized trial. Before this, it is important to resolve the question of dosage in a more systematic way.
Conclusion
As with the previous report, these encouraging results warrant further controlled research before clinical recommendations can be made. The preliminary nature of this report should be emphasized. As an anecdotal case report, it does not constitute a basis for clinical recommendations. Rather, the results of varenicline in this patient and the previous case indicate a need for further research. A logical progression might involve first a dose-finding study in adults with autism, followed by a placebo-controlled pilot trial in adults and adolescents, and finally a multisite randomized clinical trial first in adults and adolescents, and then in children with autism. Alternatively, the dose-finding study and adult/adolescent placebo-controlled pilot trial could be combined. It is our hope that this report will aid in promoting such research efforts.
Clinical Significance
To the best of our knowledge, this is only the second report of an individual with autism treated with varenicline, an α4β2 nicotinic acetylcholine receptor partial agonist. In both cases there was an ABA experiment of nature in which after initial improvement, varenicline was stopped because of concerns about potential long-term effects, then after deterioration, varenicline was resumed with resumption of improvement. These encouraging results warrant further controlled research before clinical recommendations can be made. We hope that this report will aid in promoting such research efforts.
Footnotes
Disclosures
M.M. has nothing to disclose. P.H. has received funding from Bristol-Myers Squibb in 1992 to study Abilify in autism. L.E.A. has received research funding from Curemark, Forest, Lilly, Neuropharm, Novartis, Noven, Shire, and Young Living (as well as NIH and Autism Speaks) and has consulted with or been on advisory boards for Gowlings, Neuropharm, Novartis, Noven, Organon, Otsuka, Pfizer, Roche, Seaside Therapeutics, Sigma Tau, Shire, and Tris Pharma and received travel support from Noven.