
Abstract
Antipsychotic (ATP) prescription rates have increased in children and adolescents despite concern regarding the safety and effectiveness of ATP usage in community populations. Rising safety concerns and uncertainty regarding ATP effectiveness in children stress the need for improvement in routine clinical outcome monitoring and research. Due to the growing number of children exposed to atypical ATPs, studies assessing the risk/benefit ratio of administering ATPs in this age group—especially in off-label conditions—become of high importance. The Centre for Interventional Pediatric Psychopharmacology and Rare Diseases (CIPPRD) uses a suite of instruments to monitor outcomes using the web-based HealthTracker™, a health monitoring platform. The HealthTracker allows for capture of symptoms, side effects, quality of life, patient experience, and lifetime response to individualized treatments using a multi-informant multimodal methodology. It enables the tracking of ongoing medical treatments and assists in shared treatment decision-making, longitudinal patient centered outcome monitoring, and helps optimize care. An example of its use in the CIPPRD is provided to demonstrate how it can be used for ATP-related outcome monitoring in complex neurodisability within routine clinical practice.
Introduction
T
Recent changes in atypical ATP prescription use have not only been noted in the United States but also in the United Kingdom, although the intensity and increased use are not as large as witnessed in the United States (Rani et al. 2008). ATPs are usually prescribed by psychiatrists, and in the United Kingdom, general practitioners are increasingly prescribing atypical ATPs for the treatment of off-label conditions, that is, outside the terms of marketing authorization.
In this review, we document the changes in ATP usage in children and emphasize the importance of outcomes research. In the following sections, we will describe the trend of ATP prescription rates in the United States as well as in other European countries. With regard to the accreted occurrence of safety concerns about medical treatment, we will stress the need to advance future outcomes research to ensure optimal treatment. Finally, we will provide an example of currently used outcome measurements at the Centre for Interventional Pediatric Psychopharmacology and Rare Diseases (CIPPRD) (Maudsley Hospital, London, United Kingdom).
Extended Use of ATPs over the Past Two Decades
Prescription of ATP medication over the past decades has increased in youth and even exceeds the increase of ATP administration among adults (Kalverdijk et al. 2008; Zito et al. 2013; Bachmann et al. 2014). Although the prevalence of psychiatric disorders has not significantly increased over the last two decades (Safer et al. 2015), clinician-reported diagnoses for severe conditions, for example, bipolar disorder in young children, have increased, with a consequent rise in usage rates of ATP use. Safer et al. (2015) surmise that the increase in treatment is related to the broader clinical diagnostics of psychiatric disorders (e.g., DSM-V “other specified disorder and unspecified disorder” [American Psychiatric Association, 2013]) as well as to the intense marketing by drug companies and the rising acceptance of medication for emotional and behavioral conditions by the public.
Increase in ATP Use in Children in the United States and Europe
From an American viewpoint, visits in which a second generation (atypical) ATP was dispensed to Medicaid-insured children and adolescents in Texas increased almost 500% between 1996 and 2000 (Patel et al. 2002). Overall, the pediatric usage rate of ATPs in the entire United States in 2002 was nearly sixfold the ATP usage rate of 1993 (Olfson et al. 2006) and this trend seems to be steadily increasing (Olfson et al. 2012). More broadly, it was shown recently that children and adolescents receiving any outpatient mental health service increased from 9.2% (1996–1998) to 13.3% (2010–2012) in the United States (Olfson et al. 2015).
Comparable trends have also been reported in European countries (Kalverdijk et al. 2008; Bachmann et al. 2014). In the Netherlands, the use of ATPs in 2005 doubled since 1997, with second-generation ATPs increasing almost ninefold and the first-generation ATPs staying relatively stable (Kalverdijk et al. 2008). The use of second-generation (atypical) ATPs has preferentially increased rather than the first-generation (typical) agents in Germany (Bachmann et al. 2014), in Spain (Santamaría et al. 2002; Verdoux et al. 2010), in Scotland (Verdoux et al. 2010), and France (Verdoux et al. 2015). In the United Kingdom, the use of second-generation ATPs showed a 60-fold increase between 1992 and 2005, whereas the prescription of first-generation ATPs declined (Rani et al. 2008).
When comparing the rates of increase in Germany, Spain, and the United Kingdom with the changes in the United States, the overall increases are generally lower (Santamaría et al. 2002; Rani et al. 2008; Bachmann et al. 2014). In a cross-national study by Zito et al. (2008), while atypical ATPs represented 66% of total ATP medications dispensed in the United States, they encompassed 48% in the Netherlands and only 5% in Germany. In the United States, the overall ATP prevalence of use has risen between 1992 and 2005, while the pattern of new users has been relatively steady in the United Kingdom (Rani et al. 2008). In the United States, Cooper et al. (2006) indicated that the number of new ATP users in 2001 was twice the number from 1996 (Cooper et al. 2004, 2006).
Various factors, such as the marketing of atypical ATPs since the mid-1990s as safer alternatives to conventional ATPs (Seida et al. 2012; Steinhausen, 2015), different study designs, varying healthcare delivery systems within countries, differences in availability and provision of clinical and healthcare services, may preclude definitive inferences from being made and can impede an accurate comparison of international trends. With regard to increases in ATP use in children in the United States and Europe, societal attitudes across borders and regions also need to be considered. For example in the United States, many families do not have insurance coverage to complete often protracted and time-consuming nonpharmacological treatments, and as such, families might prefer an ATP-based intervention. In this context, medication might be seen as an efficacious and inexpensive alternative (Harrison et al. 2012).
Socioeconomic Differences in ATP Treatment in Children and Adolescents
Youth with Medicaid coverage, that is, the healthcare program of the United States for youth with low income or who qualify with other vulnerabilities, are five times more likely to be prescribed ATPs than those that are privately insured (Crystal et al. 2009). One in five children and adolescents in Medicaid (19.2%) who were taking long-acting stimulants for attention-deficit/hyperactivity disorder (ADHD) also took atypical ATPs for at least 2 weeks (Kamble et al. 2015). Furthermore, only in 27% of Medicaid-insured youth aged <18 years were the FDA-specific guidelines for ATPs followed (Rettew et al. 2015). Zito and coworkers explored the increased use of ATPs by comparing data from 1997 to 2006 in 456,315 Medicaid-insured youth aged 2–17 years in a mid-Atlantic state (Zito et al. 2013). In this study, the Medicaid eligibility categories were Temporary Assistance for Needy Families [TANF], State Children's Health Insurance Program [SCHIP], Supplemental Security Income [SSI], and foster care. The study found that from 1997 to 2006, the increase in ATP use was the most apparent in youths who where Medicaid eligible who qualified for low (SCHIP) followed by very low (TANF) family incomes and reflects the increased use of ATP medication for behavioral disorders (Zito et al. 2013). Other factors that may also contribute to increased off-label ATP use include challenges that Medicaid-enrolled children face when accessing nonpharmacologic mental health treatment, as well as limited options of these treatments compared to privately insured children as described by Rubin et al. (2013). In summary, the magnitude of ATP usage is far greater in Medicaid-insured youths in comparison to those privately insured. Furthermore, there has been relatively little emphasis on community-treated populations with respect to the length of exposure (Burcu et al. 2014).
Rising Safety Concerns
Questions remain on the value of using atypical ATPs in treating off-label conditions (Crystal et al. 2009; Zito et al. 2013). Metabolic and endocrine side effects have become a major concern in the administration of atypical ATPs to children and adolescents. The deleterious impact they can have on child and adolescent health has not been fully evaluated (Vitiello et al. 2009). In comparison to adults, children and adolescents are more prone to the risks of ATP treatment. Main side effect concerns include manifestation of extrapyramidal symptoms and associated metabolic and endocrine defects. In the following section, we discuss the main side effect concerns.
Metabolic syndrome in childhood and youths
Childhood involves a period of physical and cognitive growth during which the influence of atypical ATPs on multiple physiological systems might lead to profound perturbations in neurodevelopment (Almandil et al. 2013). The application of second-generation ATPs can heighten the risk of developing the metabolic syndrome, also known as Syndrome X. This disorder is characterized by insulin resistance, central obesity, hypertension, and glucose intolerance with elevated risk of developing type II diabetes and cardiovascular diseases (Eckel et al. 2005). Analyses of metabolic effects of second-generation ATPs during childhood and adolescence are still very limited, and the differing drugs seem to vary in their propensity to induce side effects. In a systematic review and meta-analysis by Almandil et al. (2013) of 21 double-blind randomized controlled trials, statistically significant weight gain during treatment with the drugs olanzapine, risperidone, and aripiprazole was observed, with olanzapine having the greatest effect. Some others have shown that aripiprazole has a mild influence on the adult physiology, but has greater effects on child physiology (Raffin et al. 2014). Increase in weight and body mass index heightens the risk of developing type II diabetes in adults as well as in children. Bobo et al. (2013) have shown that the risk of developing type II diabetes increased threefold for children and youths treated with ATPs, and the risk rises with elevated dosage. Notably, the risk remained even after 1 year of cessation of ATP medication (Bobo et al. 2013). Moreover, weight gain appears to have an impact beyond possible metabolic changes. With increased weight gain, the effectiveness in symptom reduction narrows, underlining the importance of continuous monitoring during treatment (Martínez-Ortega et al. 2013).
Typical versus atypical ATPs
The shift toward increased use of atypical ATPs can be partly explained by their supposed lower risk of the development of extrapyramidal symptoms (Seida et al. 2012). In a Spanish sample that analyzed the ATP use in children and adolescents, it was shown that haloperidol was the most common typical ATP and risperidone the most common atypical ATP that had been prescribed within this age group (Baeza et al. 2014). In general, typical (first generation) ATPs are more often associated with sedation and the less often occurring neuroleptic malignant syndrome and tardive dyskinesia. By contrast, weight gain, type II diabetes, and higher levels of lipid and prolactin are considered to be side effects associated with the use of atypical (second generation) ATPs (Seida et al. 2012).
Only a few studies have compared the benefits and adverse events associated with typical and atypical ATPs and/or their influence across various age groups. In a systematic review by Young et al. (2015), it was concluded that ATP polypharmacy and long-term treatment increase the risk and severity of side effects. Clozapine, an atypical ATP, was the ATP medication most associated with metabolic disturbances and olanzapine, another atypical ATP, associated with weight gain (Young et al. 2015). In other studies, it was shown that the risk of developing extrapyramidal symptoms was amplified in children treated with atypical ATPs as well for typical ATP treatment, as it is shown for adults (Seida et al. 2012, Cohen et al. 2012). Thus, the whole clinical picture of side-effects induced by ATPs seems to be more complex. This has been shown in a study, investigating rare adverse events, in children aged 0–12 years, which were reported and submitted to the FDA Adverse Event Reporting System (FAERS). Diverse effects depending on which ATP subclass was administered were found (Kimura et al. 2015). The Treatment of Early-Onset Schizophrenia Spectrum (TEOSS) study explored the safety and effectiveness of two second generation ATPs, olanzapine and risperidone, with a first generation ATP, molindone, in 116 youth 8–19 years of age with early-onset schizophrenia spectrum disorders during an 8-week treatment period (Sikich et al. 2008). In this double-blind study, no statistically significant differences in response rates (molindone: 50%; olanzapine: 34%; risperidone: 46%) or magnitude of symptom reduction between the treatment groups were observed. When evaluating the metabolic profile of patients, the highest weight gain was seen in the olanzapine and risperidone treatment groups. Of these, treatment with olanzapine showed the greater propensity toward weight gain, increased fasting cholesterol, low-density lipoprotein, insulin, and liver transaminase levels. Higher levels of self-reported akathisia were noted in the molindone treatment group (Sikich et al. 2008). In this study, following review of interim safety data by the National Institute of Mental Health (NIMH) Data and Safety Monitoring Board, assignment to the olanzapine treatment arm was terminated because of the greater increases in weight gain (Sikich et al. 2008). Taken together, the results from this trial question the value of using second-generation ATPs to treat early-onset schizophrenia in youth. Given the usage rates of atypical ATPs in youth for nonpsychotic disorders, from a public health perspective, this study further highlights the safety concerns of ATP usage in youth, particularly in relation to weight gain and metabolic dysfunction (Sikich et al., 2008). The TEOSS study continued to follow a subgroup of 54 youths for a further 44 weeks (Findling et al. 2010). In this study, only 12% of patients completed the full trial (52 weeks), while 26% of patients, who qualified for maintenance treatment, completed the 44-week extension trial. Adverse events, poor response, followed by noncompliance to study-related procedures were the common factors for study discontinuation. Overall, these observations further highlight the complexity of the side effect profiles between typical and atypical ATPs (Findling et al. 2010).
With a varied and profile of serious adverse events emerging with atypical ATP use in community populations, a more detailed analysis is warranted when approaching its use in nonpsychotic patients. Careful side effects monitoring should become part of routine care. Side effects such as metabolic syndrome, type II diabetes, abnormal serum lipid and prolactin levels need regular monitoring. However, baseline lipid and glucose levels are still seldom assessed, and thus, the management of side effects is largely deemed inadequate (Young et al. 2015). The detection of extrapyramidal symptoms is much more straightforward and might result in more frequent diagnosis, and consequently, the management of extrapyramidal symptoms can be dealt with quite rapidly. In this regard, treatment with ATP medication that causes metabolic syndrome might mistakenly appear to be safe compared to those that cause extrapyramidal symptoms, as side effects associated with metabolic syndrome cannot be detected easily and usually require clinical laboratory blood assays. A systematic assessment is needed to capture the complete side effect profile of each ATP as well as combinations of medication administered.
Caution when analyzing safety concerns
A detailed evaluation of safety research in the pediatric population is warranted to assure reliable reports of ATP exposure in children and adolescents. Although an increased number of studies examine ATPs in children, many studies focus on effectiveness alone. This gap in research, however, seems to be declining as more recent published articles are more often taking safety assessment into account (Cohen et al. 2012). Nevertheless, the diversity of safety measurements that has been used hampers the comparison of studies as well as use of different ATPs (Greenhill et al. 2003). There is no standard measurement to assure that drug safety monitoring is established reliably. Moreover, a lack of agreement about a suitable definition of possible side effects and variations in their dimensions make an examination difficult (Greenhill et al. 2003). One particular challenge is the demarcation between treatment emergent adverse events from those that are new symptoms of mental and behavioral conditions, that is, behavioral toxicity (Offidani et al. 2014).
In a RCT by the Research Units of Pediatric Psychopharmacology (RUPP) autism network, additional safety evaluations were included when assessing the treatment of irritability in children and adolescents with autism treated with aripiprazole and placebo. Evaluations were based on weight and laboratory measures, structured assessment through scales addressing various possible side effects, as well as severity of symptoms in regard to autism and the medication intervention (Marcus et al. 2009; Owen et al. 2009). Tailoring assessments in studies to the particular needs and characteristics of the studied disorder, population, and the medication would allow (at least for short-term use in trial populations) a valid and efficient evaluation of ATP safety in the future.
Monitoring to assure efficacy and safety
Although there have been innovative attempts in recent years to monitor and control the prescription of atypical ATPs through peer review policies in the United States Medicaid system (Schmid et al. 2015), a study in two state Medicaid programs showed the new policies to have a modest effect in reducing ATP use in children and adolescents (Stein et al. 2014). Nevertheless, policies may have an effect on new prescription use rather than existing ATP treatment. Additional research on physician peer review is desirable.
Monitoring atypical ATP usage would provide a tool for early detection and reversal of possible side effects and ensure a safer use of atypical ATPs in children and adolescents. There is substantial evidence that patient-reported outcome measurements (PROMs) reflect the patient's perception as well as the actual health status of the patient and result in the reduced necessity of applying diagnostic tests (Oates et al. 2000). PROMs can also help to monitor important proximal outcome domains such as physical and psychological symptoms, satisfaction, and quality of life (QoL) aspects. However, the task of assessing distal outcomes (i.e., functional improvement by measuring school performance, reducing juvenile justice services, and social development among community-treated populations) remains a topic receiving little or no research attention.
HealthTracker™ (
The CIPPRD Model
In chronic illness, patient-centered care includes active involvement of patients because healthcare decisions have long-term implications. The treatment pathway may often be at a crossroads with diverging paths that will have important ramifications for personalized care. In terms of medical management in chronic illness, shared decision-making is central to optimal response as more than one path may exist and should reflect biopsychosocial factors, including the type of disorder, associated physical illness, patient and family factors, insurance coverage and healthcare system factors, life stressors, adaptive functioning, and social development.
The systematic management and monitoring of patients with complex neuropsychiatric presentations in rare diseases is problematic, and therapeutic strategies aimed at improving patient-centered outcomes are limited. The CIPPRD at the Maudsley Hospital is a national specialist psychopharmacology unit, which focuses on providing whole-person medicine and integrated mental and physical healthcare in children and young people with complex, severe, multicomorbid, often treatment-resistant disorders, and manages rare, serious, psychotropic-induced side effects in children and youth aged 2–24 years. Coworking with cardiology, hematology, endocrinology, neurology, and other departments across the United Kingdom, the CIPPRD offers highly specialist personalized pharmacological and psychological assessment and treatment for neuropsychiatric problems such as severe emotional, behavioral, and autonomic dysregulation (EBAD) in children with genetic disorders (Rett Syndrome, Septo-Optic Dysplasia, Mucopolysaccharidoses, and other rare diseases), neurodegenerative (dementias) and neurometabolic disorders in children and young adults. EBAD is often treated with ATPs long term. The integration of clinical and academic work allows CIPPRD to translate its findings into clinical practice. The CIPPRD model for patient-centered care is shown in Figure 1.
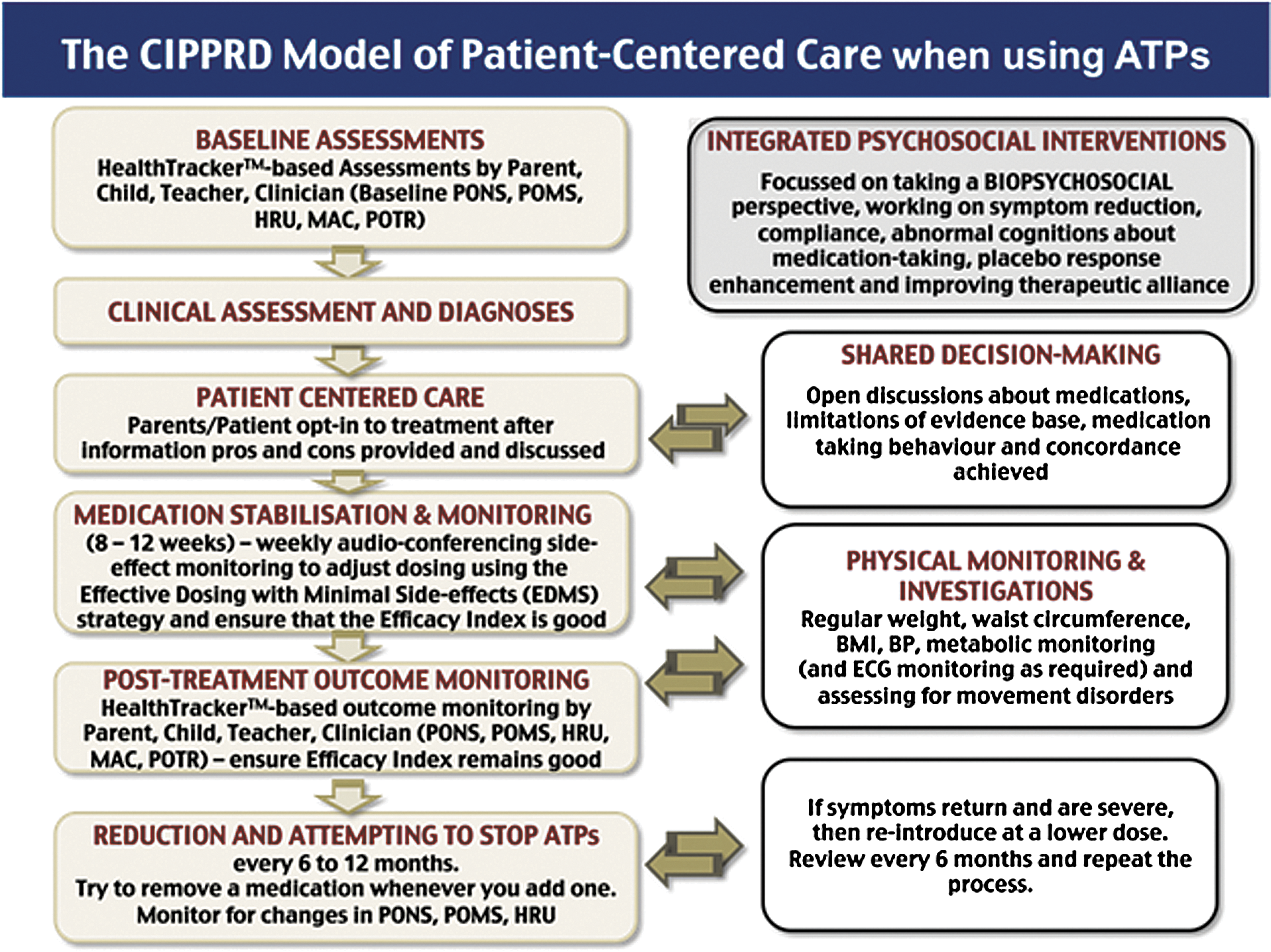
The CIPPRD Model of Patient-Centered Care. ATPs, antipsychotics; BMI, body mass index; BP, blood pressure; CIPPRD, Centre for Interventional Pediatric Psychopharmacology and Rare Diseases; ECG, electrocardiogram; EDMS, effective dosing and minimal side-effects; HRU, How R U; MAC, medication adherence and compliance; POMS, profile of medication side effects; PONS, profile of neuropsychiatric symptoms; POTR, profile of treatment response. Color images available online at
As many patients in the CIPPRD are managed using ATPs, it harnesses e-Health strategies using web-based patient monitoring (using the HealthTracker) and biometric physiological data (real-time autonomic variability in heart rate, skin conductance, blood volume pressure, perspiration, and temperature) captured using wearable sensor technology.
The CIPPRD provides three programs for assessment and treatment in three distinct areas. These are the (1) Consultation-Led Effective Assessment and Recovery (CLEAR) program, (2) the Complex Multi-diagnoses Patient-Led Effective Treatment & Empowerment (COMPLETE) program, and (3) the Comprehensive Assistance for Rare Etiologies (CARE) program. ATPs are used in managing patients in all three pathways. The key points of these programs are described below: (1) The CLEAR Program - implements rigorous methods to prevent and reduce inpatient care in the very severely ill. The team assists in optimizing care and recovery in children with acute serious psychopathology; managing children who are too dangerous to be managed in routine inpatient settings; and assisting in managing nonresponders in long inpatient admissions. (2) The COMPLETE Program - addresses the needs of subjects with treatment-resistant multiple severe co-occurring neuropsychiatric disorders (average of 5 or more conditions). The team has developed strategies that help manage patients with multi-comorbidity, which are outlined in the following sections. (3) The CARE Program - addresses the neuropsychiatric needs of patients with multisystem involvement, especially when managing EBAD (Singh and Santosh, 2016). Psychophysiological monitoring is central to the care of children with neurometabolic and rare diseases, including neurodegeneration and severe and profound acquired brain injury. Currently, there are specific programs for Rett syndrome, Septo-Optic Dysplasia, and Mucopolysaccharidoses. Children with serious psychotropic-induced side effects such as tardive dyskinesia, metabolic syndrome, Clozapine-induced pericarditis, arrhythmias while on ATPs, and reintroduction of ATPs in those who develop Steven–Johnson syndrome and children with severe acquired brain injury among others are managed here.
The CIPPRD routinely consults patients, parents, and clinicians, using focus groups to engage key stakeholders and canvass opinion. Based on this, the CIPPRD has developed an e-Health augmented model that can be used in routine clinical care where ATPs are prescribed to children and adolescents. Some of these approaches are discussed below.
Art of prescribing
Families’ attitudes, beliefs, and perceptions about psychiatric illness and treatment play a large role in medication treatment decisions. A trusting provider–patient relationship has a positive effect on adherence. Parents and patients respond better when they feel understood, accept why treatment is necessary, and are in agreement with the prescriber regarding the need for the treatment (Santosh, 2014). Rewards experienced from medication treatment include improvement in symptoms, school performance, and family relationships and reduced level of parenting stress. Identified costs include impact of side effects, social stigma, lack of response, fears of addiction, and fear of changing the child's personality (Hamrin et al. 2010). To provide participatory care through shared decision-making, safety and effectiveness monitoring, the CIPPRD uses several instruments that capture information on the aspects described above to improve patient-centered outcomes. Multifaceted individualized treatments are used to target symptoms and minimize side effects. Instruments such as the Profile of Treatment Response (POTR), Medication Adherence and Compliance scale, Profile of Neuropsychiatric Symptoms (PONS), Emotional and Behavioral Side effects Scale (EBSS), Physical Side effects Scale (PSS), and “How R U” scale (HRU) are incorporated into daily, routine clinical practice to provide shared decision-making and patient-centered care. At the CIPPRD, diagnostic rigor is ensured when diagnosing comorbidity (better labeled as coexisting disorders) by first checking that the central symptoms of the coexisting disorder are present, such as the presence of obsessions for diagnosing obsessive compulsive disorder (OCD); symptoms attain “thresholds” used in classificatory systems and are developmentally inappropriate; ensuring that symptoms are NOT “double counted” (such as counting hyperactivity for both ADHD and hypomania); making sure that each disorder creates additional impairment; verifying that the start and course of the disorders are not indistinguishable from one another; and using several sources of clinically evaluable information to ascertain the aforementioned criteria (Santosh, 2014).
Effective dosing with minimum side effects strategy
The effective dosing with minimum side effects (EDMS) strategy uses short telephone-based medication monitoring calls to assist in the care and management in the CIPPRD. The EDMS strategy aims to use the lowest possible dose of a medication to achieve adequate management of symptoms with minimal side effects. ATPs are initiated at roughly 1/6th–1/8th of the dose one would assume the child might need, and then increasing it by that amount every 5–6 half-lives of the drug when being introduced (Santosh and Singh, 2016). For example, a child being initiated on aripiprazole for a nonpsychotic indication would be started on 0.5 mg per day and increased by 0.5 mg every 7 days, to get to a therapeutic dose of 2–3 mg per day in a few weeks. This approach produces symptom improvement with minimal side-effects, arising from a combination of (1) the biological response to the medication, (2) the improved therapeutic alliance, and (3) a possible priming effect that might harness placebo response; all leading to improvement being achieved with smaller doses of medication than is conventionally used.
Web-based health and drug safety monitoring in child and adolescent mental health
The CIPPRD currently uses the HealthTracker suite of instruments to assist monitoring the progression of treatment of patients, including those taking ATPs. HealthTracker allows multimodal presentation of questionnaires, such as the PONS; Profile of Medication Side effects (POMS) comprising the EBSS and the PSS; HRU; and POTR, and assists in automatically providing scales based on the developmental level to assure that the questions are being understood by the patient. The HealthTracker provides clinicians with baseline and longitudinal overview of symptom, side effects, QoL, patient experience, and treatment response for each patient (Santosh and Singh, 2016). The completion of the provided online questionnaires in HealthTracker before having a face-to-face appointment expedites the patients’ treatment pathway by enabling the clinician to focus on the issues troubling the patient and/or the parents/caregivers within each appointment in a time-efficient way. Using web-based PROMs routinely in mental as well as medical healthcare systems would assist clinicians in their daily work and help to optimize patient outcomes. The measures are elaborated further below.
• Profile of Neuropsychiatric Symptoms (PONS): The PONS scale is a reliable and valid web-based PCOM that allows screening and assessment of frequency and severity of impairment of 30 specific symptom domains commonly seen in neuropsychiatric disorders in children and adolescents (Santosh et al. 2015). Symptoms of developmental disorders such as ADHD, autism spectrum disorder, OCD, motor coordination disorder, disruptive disorders (oppositional defiant disorder/conduct disorder), psychoses, bipolar disorder, and anxiety and depressive disorders can be assessed. Different versions of the scale for children of different ages as well as parents, teachers, and the clinicians allow a simplified use of the instrument. Using a web-based instrument allows the use of audio assistance for those with reading difficulties, adapts for visual impairment, and provides age-appropriate questions to make the instrument easily accessible (Santosh et al. 2015).
• Medication Side effects and “How R U”: Medication side effects can be captured using the EBSS and PSS, and the “How R U” scale is a web-based QoL measurement (Santosh et al. 2015).
• Profile of Treatment Response (POTR): Information that is obtained on the clinician POTR consists of the type of medication, dosage, duration of use; symptoms targeted; daily functioning of the child/adolescent, severity of illness, effectiveness of treatment, and reason for discontinuation (if applicable). The information on the treatment response is obtained directly from the child/adolescent, parent/caregiver, and the clinician. As part of this, the therapeutic efficacy index (a scale assessing the therapeutic effect of the drug treatment) has been modified, with clear guidelines for scoring clinical improvement and side effects. This ensures comparability of therapeutic efficacy between ATPs and other medication to ensure that the patient receives the most effective treatment with the lowest side effect profile. This scale can help decision-making around whether a medication, such as an ATP, should continue to be prescribed to the individual patient or whether a different treatment should be considered. This provides a longitudinal understanding of the patient's history of treatment response.
An example of using the above measures on HealthTracker for routine monitoring of aripiprazole use in 34 patients managed in the CIPPRD is shown in Figure 2. As this is a relatively small sample, this system-wide monitoring tool needs to be evaluated on a larger sample of patients on different ATPs.
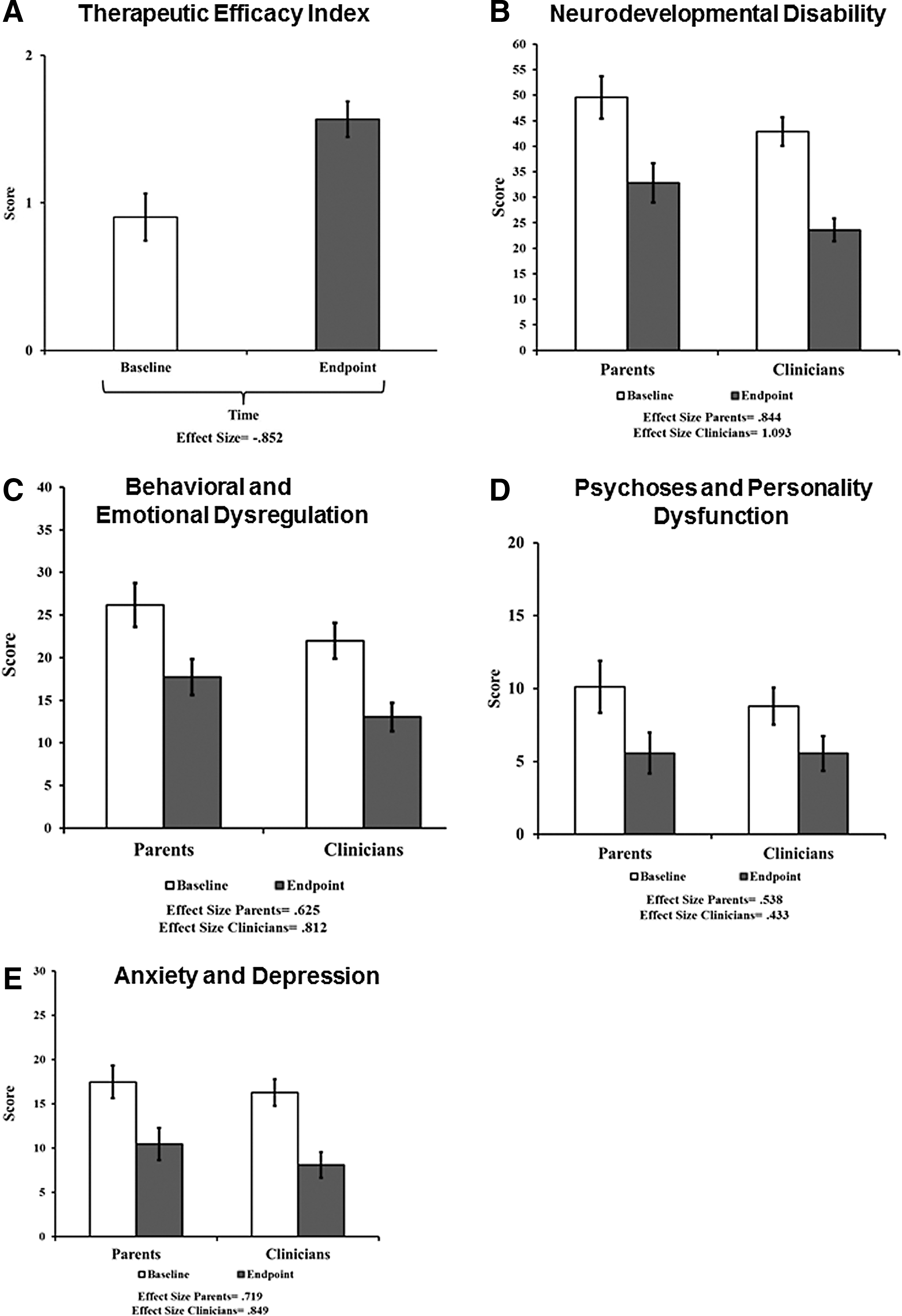
Monitoring aripiprazole effectiveness and profiling response in the CIPPRD. Longitudinal study of aripiprazole (mean [ ± SD] daily dose of aripiprazole 3.89 mg ±5.44) on neuropsychiatric outcomes in CIPPRD patients (n = 34) during a 12-month duration. Data are presented as raw scores for Parents and Clinicians Therapeutic Efficacy Index
In general, clinicians would benefit from web-based questionnaires on prior history to gain relevant information before seeing their patients for the first time so as to know beforehand which aspects to focus on during the clinical examination. This applies also for the monitoring of psychotropic usage in patients. A major problem with metabolic syndrome monitoring in ATP usage is the need for regular blood tests—many clinicians state that the children refuse blood tests and so they do not have data available to make a diagnosis of metabolic syndrome. Longitudinal ATP drug safety and clinical effectiveness monitoring could easily become routine clinical practice as in the CIPPRD, with the use of web-based monitoring using platforms such as the HealthTracker. This would especially be useful in tracking the effectiveness and possible treatment emergent adverse events of atypical ATP in off-label conditions such as aggressive behavior in youths (especially in those who are in the child welfare system). Using online measures within and across national services would support advances in global outcomes research in ATPs. This would reduce the costs associated with unnecessary care (Paris, 2015) while improving healthcare service delivery efficiently.
Limitations
Despite the evidence presented in this review describing high rates of psychotropic medication among children and young adolescents, the findings are in part challenged by Merikangas et al. (2013), who suggest that many children in the United States with unrecognized psychiatric needs never use mental health services and even less obtain treatment when these concerns are acknowledged. However, it is clear that the intensity of psychotropic medication use in children and adolescents is much greater in the United States than in Europe. Rubin (2013) outlines the difficulties when analyzing psychotropic use in children and adolescents. It is important to stress that ATP treatment is not the same for all children within the United States, especially those in the child welfare system. Accordingly, caution should be exercised in the absence of standardized monitoring of effectiveness and safety of psychotropic medication usage in children, and future studies should take these possible variations between populations into consideration. It might also be prudent to measure therapeutic effectiveness, patient experience, adaptive functioning, and the value of treatment, especially for longer-term functional outcomes when large prospective cohort studies are planned.
Conclusion
In summary, over the past decades, an increase in atypical ATP usage in children has become apparent not only in the United States but also in European countries such as the United Kingdom, Germany, the Netherlands, and Spain (Santamaría et al. 2002; Olfson et al. 2006; Kalverdijk et al. 2008; Bachmann et al. 2014). The goal of this article was to stress the need for expanded outcomes research with regard to ATP usage in children and adolescents. Not only do children represent a vulnerable population that is being exposed to psychotropic medications but the missing evaluation of atypical ATP response, safety, and tolerability in off-label conditions also underlines the need for further investigation (Almandil et al. 2013, Rubin 2013). The use of PROMs routinely in clinical practice using systems such as the HealthTracker, as being done in the CIPPRD model of patient care, would allow one not only to determine the effectiveness of ATPs but also allow the use of lowest possible doses needed and identify whether the benefits outweigh the risks. That said, cost effectiveness studies in naturalistic settings that include costs of not only the medication but also the costs of monitoring and managing the side effects such as metabolic syndrome and extrapyramidal symptoms should be encouraged. Further development of web-based monitoring using standardized measures, completed by the child and parents, reviewed in clinic by clinicians for risk/benefit analyses and shared decision-making, would provide a broadened insight into the actual medication use and ensure optimized patient-centered treatment.
Footnotes
Acknowledgments
The authors are grateful to the patients and families and the team of dedicated professionals (Dr. Kitty Kwan, Dr. Pushpika Singappuli, Dr. Chiara Colonnelli, Dr. Maria Xirou, Dr. Kate Lievesley, Dr. Katherine Hooker, Ms Corrine Thompson, Ms Winifred Eva, and Ms Cassandra Deane) working together in the Centre for Interventional Pediatric Psychopharmacology and Rare Diseases (CIPPRD) that have allowed us to develop the models described above.
Author Contributions
Dr. Paramala Santosh provided the necessary data and important intellectual content, revised the article, and provided critical oversight for the structure of the article. Dr. Federico Fiori analyzed the data and reviewed the article. Ms. Laura Bell and Dr. Jatinder Singh conducted the literature review, wrote the article and revised it, and provided intellectual oversight. All authors have read and approved the final article.
Disclosures
Dr. Paramala Santosh is the Head of the Centre for Interventional Pediatric Psychopharmacology and Rare Diseases (CIPPRD), Maudsley Hospital, London, and is also the coinventor of the HealthTracker and is a Director and shareholder in HealthTracker Ltd.
Dr. Federico Fiori is a Data Analyst employed by HealthTracker Ltd.
The other authors have no conflicts of interest to declare.