
Abstract

Chief Complaint and Presenting Problem
J.
History of Present Illness
Mother reported that J. was a difficult to soothe baby who by age 2 years was significantly hyperactive. As a preschool child, J. developed additional behavioral and emotional difficulties that impacted his functioning both at home and at day care. Problematic behavior included low frustration tolerance and aggression; for example, J. had a history of cruelty to animals. Emotional problems included tantrums, crying episodes, outbursts, and demanding behavior; as a result, J. was reported to have poor peer relationships. J. was referred at age 5 and a half years to a community clinic affiliated with an academic teaching hospital for threatening to kill his older sister during an argument.
J. was subsequently diagnosed with a disruptive behavior disorder, not otherwise specified. His initial treatment plan included weekly group therapy with an emphasis on social skills training, parent management training (PMT) and dyadic work with J. and his mother. A psycho-educational evaluation revealed findings including a learning disorder, not otherwise specified, and a mixed receptive-expressive language disorder. J.'s mother was often non-adherent to the PMT program.
In addition, J. began to frequently smell his fingers and to check to see if they were clean; difficulties around separation with mother and frequent crying were also observed. A subsequent re-evaluation resulted in a diagnosis of an anxiety disorder, not otherwise specified; a formal diagnosis of OCD was not given. At that time, the other symptoms suggestive of an anxiety disorder were separation difficulties from mother, easy tearfulness, and an increase in disruptive behaviors around anxiety-provoking content, both in group therapy and in dyadic work with J.
In this context J.'s parents, who had been having significant conflicts, made plans to divorce just prior to J.'s sixth birthday. J. subsequently began to express suicidal ideation and guilt-laden thought content that he was a “bad child” and would “burn in the fire.” His finger smelling increased in frequency and he began washing his hands frequently, expressing anxiety if he was interrupted.
J.'s clinicians viewed his diagnosis as an anxiety disorder not otherwise specified, with a co-occurring learning disorder. By six years and nine months his separation anxiety was noted to have increased significantly; he began to refuse to shower or play in a room alone as a result of fear that his mother would abandon him.
On J.'s seventh birthday a diagnosis of ADHD was confirmed. After J.'s finger smelling began to increase significantly, referral was made to a pediatric neurologist for diagnostic clarification. The neurologist reportedly felt that the finger smelling was a tic, and diagnosed a tic disorder (based on this single tic). Upon retrospective review, multiple other simple tics, including shoulder shrugging, grunting, nasal flaring, jaw thrusting, biting, and eye rolling, appeared to be present at this time, but had not been brought to clinical attention. Given these additional motor and vocal tics that had been present for more than one year, J. would also have met diagnostic criteria for Tourette's Disorder (TD)
By the time J. was age seven and a half, the full diagnostic picture of ADHD, OCD, and TD was established. At age nine J. was referred for group exposure-response prevention (ERP) therapy for his obsessive-compulsive symptoms. At his pre-treatment evaluation, J. disclosed mostly harm obsessions, with concerns that he would be eaten by a shark. He refused to shower, afraid that a shark could emerge from the drain. He refused to sleep or leave home without his mother, fearing something bad might happen to him. He had also developed additional tics, including complex motor tics and vocal tics. His most frequent tic was biting, as J. would gnaw at his clothing, chew on headphones and erasers, and bite into the air. J. had also bitten his mother and himself. His biting was often preceded by eye darting, shoulder thrusting, jaw extending, and chin dropping. Vocal tics included throat clearing and mild grunts.
Over the course of group treatment J.'s OCD symptoms improved. His shark obsessions decreased so significantly that he was able to go to the beach, shower, and sleep by himself. He still exhibited some separation anxiety, but could better tolerate separations.
Past Psychiatric History
J. had no formal psychiatric treatment prior to his referral at age 5. At age 5, J. underwent psycho-educational evaluation. Stanford-Binet Intelligence Scales— Fifth Edition (SB-5; Roid 2003) demonstrated average non-verbal Intelligence Quotient (IQ) and low average verbal IQ. Preschool Language Scale, Fourth Edition (PLS-4; Zimmerman & Castilleja 2005) revealed receptive and expressive language functioning to be one year below age expectancy. Vineland Adaptive Behavior Scales, Second Edition (Vineland-II; Sparrow et al. 2005) demonstrated daily living and motor skills in the adequate range, communication within the moderately low range, and socialization in the low range.
Developmental and Personal History
J. was the product of an uneventful pregnancy with full prenatal care and no maternal use of alcohol, tobacco, or narcotics. Delivery was via Caesarean section; birth weight was 8 pounds, 12 ounces. Postnatal history was uneventful. From infancy, J.'s mother described him as difficult to soothe.
Educational History
J. entered day care at age four years. He was reported to be a socially well-related child, but exhibited significant behavior problems. J. entered mainstream kindergarten with an Individualized Education Plan that included a regular classroom with weekly speech therapy. He performed well academically, but his behavior remained problematic. At age eight, he transitioned to a 12:1:1 classroom setting to address ongoing ADHD symptoms and learning issues.
Social History
J. lived with his mother, an 18-year-old maternal half-sister, and a 20-year-old maternal half-brother in an inner city neighborhood. Mother had worked full time since her separation from father, who saw J. on weekend supervised visits. Mother had full custody.
Pertinent Family History
J.'s maternal half-brother had received speech therapy during childhood. Maternal half-sister had diabetes due to obesity, and was being treated for depression in a community clinic. A maternal cousin also received treatment for hyperactivity. There was no established family history of OCD or TD. There was reportedly no diagnosed psychiatric history in paternal relatives.
Medical History/Medications/Recent Physical Examination
J. had no history of major medical problems such as asthma, hearing, or visual impairments. J. had not experienced any serious physical injuries. He was hospitalized once at age 2 years for four days due to a fever attributable to tonsillitis. J. was allergic to eggs, cockroaches, and cats.
With regard to growth and development, J.'s weight was well above the 95th percentile for most of his life (see FIG. 1). Notable was the growth curve change at approximately age 9–9 1/2 years that coincided with his completion of his group CBT with ERP for OCD. In contrast, J.'s stimulant regimen had been initiated one day shy of his seventh birthday; it had also been increased just prior to the start of his group CBT.
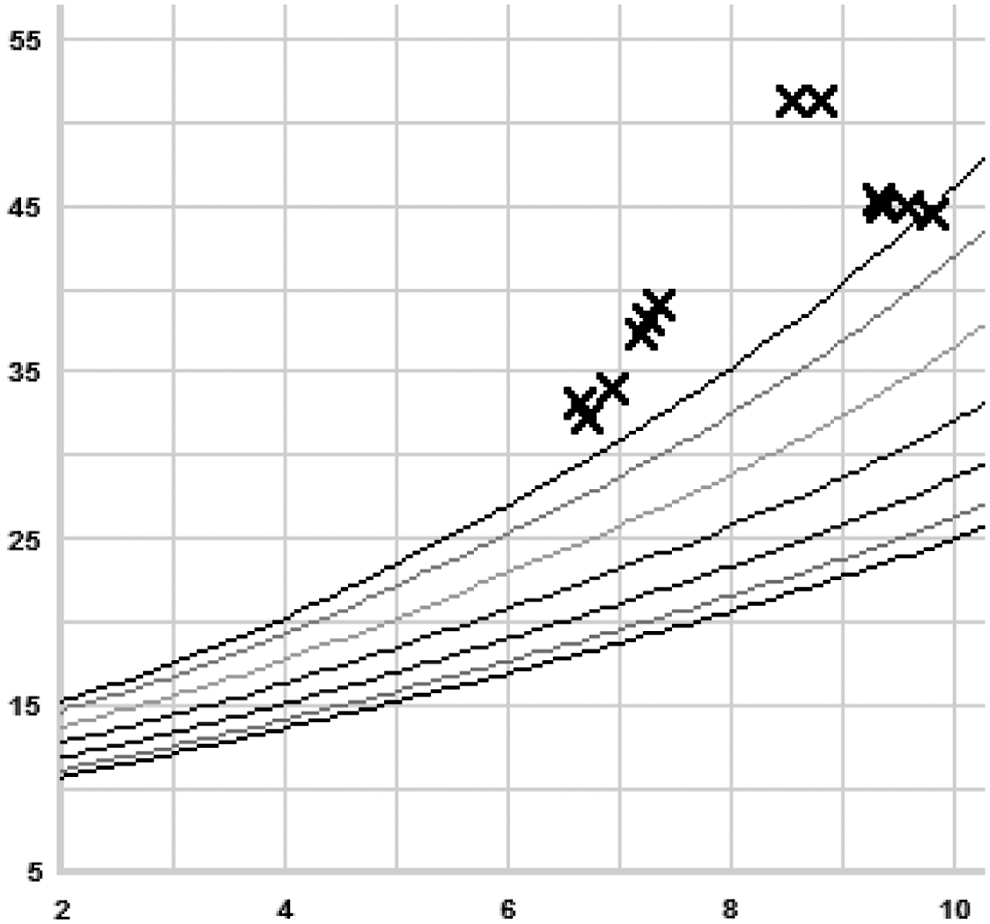
Weight in pounds by age in years. X axis denotes age in years, Y axis denotes weight in pounds. Highest curve line represents 95th percentile of weight for given age.
Medication History
J.'s first trial of psychotropic medication began at age five years and eight months, after two months of group treatment for symptoms of anxiety; his primary working diagnosis was an anxiety disorder not otherwise specified. J. was started on fluoxetine 2.5 mg each morning that was titrated upward to 5 mg just before his sixth birthday, and to 10 mg by six years of age. Shortly after his sixth birthday, mother began to report that J. had become more aggressive on fluoxetine, and his teacher became concerned about an increase in hyperactivity and impulsivity. The school psychologist raised a question of ADHD.
Although a stimulant was considered, a trial was deferred while J.'s fluoxetine was increased to 12.5 mg to target these symptoms. Just prior to his seventh birthday his fluoxetine was increased to 20 mg without any significant change in his presentation. J. remained anxious over separation, and as described above, demonstrated guilty thoughts, expressed suicidal ideation, and was often emotionally labile and explosive in the context of his parents' divorce.
Given an additional diagnosis of ADHD, an extended release (ER) formulation of dexmethylphenidate 5 mg was added to J.'s medication regimen just one day shy of his seventh birthday. Within one month it was increased to 10 mg, then to 15 mg and 20 mg over the following two months. J.'s finger smelling behaviors increased, although there was no documentation of any other increase in tic behaviors; at age eight his fluoxetine was subsequently increased to 25 mg and then to 30 mg. J. had no sleep disturbance on this regimen, and although his weight curve appeared to change at approximately this time, neither he nor his mother noted any loss of appetite nor restricted behaviors.
At that time, with the input of a specialist in tic disorders, guanfacine 0.25 mg twice a day was added to address the finger smelling, and increased to 0.25 mg each morning and 0.5 mg at bedtime. No adverse effects were noted, and there appeared to be a significant improvement in both J.'s anxiety and his tic-related behaviors. His stimulant was also increased to 30 mg just prior to his enrollment in group CBT. J.'s medications were held at the following doses throughout his participation in his group CBT for OCD program: • Fluoxetine 30mg each morning
• Dexmethylphenidate ER 30 mg each morning
• Guanfacine 0.25 mg each morning and 0.5 mg
Whereas these medications appeared to be optimized to J.'s participation in group treatment, they were purposely held constant throughout the duration of his group CBT participation in order to accurately assess the efficacy of this intervention. Following his completion of his group treatment at age nine and a half, J.'s dexmethylphenidate was reduced from 30 mg to 20 mg, guanfacine was increased to 1 mg by mouth twice a day, and fluoxetine was continued at 30 mg. One month later, his dexmethylphenidate was further reduced to 15 mg, guanfacine increased to 1 mg in the morning and 2 mg at bedtime, and fluoxetine increased to 40 mg. One week later his guanfacine was titrated to 2 mg twice a day. J.'s tics significantly decreased on this regimen, his anxiety improved, and his ADHD symptoms appeared stable despite the lower stimulant dosing. There were no adverse effects. Over the next three months J.'s fluoxetine was slowly increased to his final dose of 80 mg. His anxiety at the last point of follow up was significantly reduced. J.'s final pharmacotherapy regimen was: • Fluoxetine 80 mg in the morning
• Dexmethylphenidate ER 15 mg in the morning
• Guanfacine 2 mg twice a day
Mental Status Exam
At the conclusion of group treatment, J. presented as an overweight nine-year-old boy at his first medication management visit. In contrast to his presentation during the most of his group CBT, J. was nearly motionless with a rigid, upright posture, and lacked spontaneous speech. He frequently grunted, flared his nostrils, shriveled his nose, and cleared his throat. Throughout his group CBT he was often loquacious, exhibited echolalia, and described as “silly” by his peers; however during this visit he appeared to be very inhibited and restricted in his ability to engage in discussion or play.
J. quickly revealed obsessions concerning the intake of food. He had lost significant weight (see FIG. 1). He was cooperative, although his affect was mostly restricted to anxiety. There was no evidence of thought disorder or suicidal or homicidal ideation. Although he could recognize that his shark obsessions were “stupid,” he remained fearful of and often avoided discussion of these OCD symptoms. He recognized his tics as tics, and understood that his medications were helpful in allowing him to remain “the boss” of himself, his focus, and his behaviors. His insight and judgment were fair.
Brief Formulation
J. was a 9-year-old boy referred for medication management following group CBT for OCD, during which his harm obsessions and rage attacks significantly decreased. J.'s early development was characterized by hyperactivity, impulsivity, and aggressive behavior; he met diagnostic criteria for ADHD. Additionally, J. had multiple motor and vocal tics, and met diagnostic criteria for TD. Given expressive and receptive language delays, a specific communication disorder was also considered.
From a biological perspective, J. may have been rendered vulnerable to neurodevelopmental and psychiatric disorders, as his maternal family history was notable for affective illness and possible ADHD. J.'s obesity would also place him at risk for medical complications such as diabetes, which had already developed in his maternal half-sister, hypertension, and cardiovascular disease.
From a psychosocial perspective, J.'s symptoms were significantly exacerbated at the time of his parents' divorce. The divorce occurred in temporal association with his transition into school age, at a time when social-emotional and cognitive developmental tasks predominate. His internalizing symptoms and development of brief suicidal ideation may be understood as a product of the changes in his family at that time. Additionally, his symptom-focused CBT for OCD appeared to have altered the foci around which his anxiety manifested, demonstrating the ability of a psychosocial intervention to fundamentally alter the presentation of a neurobiologically derived disorder.
Multi-Axial Diagnoses
Discussion
The development and evolution of J.'s symptoms and clinical course over time represents a common but challenging dilemma for child and adolescent psychiatrists. In the case of children with the “triad” of OCD, ADHD, and TD, which frequently co-occur, each set of symptoms tends to have its own developmental course. The child's clinical picture is constantly evolving, so unless the child and adolescent psychiatrist can anticipate the full clinical picture at age 5–6 years, often before all symptoms have presented, he or she may miss the pharmacotherapeutic boat! Indeed, the temporal course of triad symptomology is unique and marked by OCD, ADHD, and TD presentations at different developmental ages (Shprecher et al. 2014).
Given that we often need to treat target symptoms, regardless of diagnosis, before the full picture has developed, it is important to be able to anticipate that pharmacotherapy may need to evolve as well. As life events often influence the presentation of TD (Steinberg et al. 2013) and the triad, much as they did in the case of J., the psychopharmacologist must also be attentive to the child's experiences in the development of an optimized treatment.
In this case, J. had a suboptimal response to social skills group treatment, parent management training, and eventually to a trial of selective serotonin reuptake inhibitor (SSRI) monotherapy. Behaviors that were initially described as aggressive and a product of disruptive behavior disorder may have been more responsive to a stimulant than an SSRI. It appears that J.'s comorbid anxiety appeared to be the priority for his treatment team at that time; indeed clinicians are frequently in a quest for parsimony: to find one disorder to explain the full presentation of symptoms. As is the case for J., ADHD and OCD symptoms usually cause greater distress and/or impairment in children with TD (Wanderer et al. 2012). Thus it is not surprising that J.'s clinicians first targeted these problems.
The ADHD-OCD-TD triad, described in categorical nosology, may in fact represent one specific neurodevelopmental phenotype (O'Rourke et al. 2011). Genomic studies will help identify children at risk for this phenotype. One way to conceptualize this putative phenotype is an underlying inherited deficit in inhibitory control with specific developmental courses of each set of symptoms (Sheppard et al. 1999). For example, hyperactivity, impulsivity, and disruptive behavior would predominate in early childhood, motor and vocal tics upon the transition to the school-age years, and obsessions, compulsions, and anxiety in the early adolescent years. Indeed this developmental progression and course would parallel specific development of circuits in underlying brain regions from basal ganglia to anterior cingulate and pre-frontal cortex.
An alpha-2 agonist such as guanfacine might be a promising monotherapy at the outset to target ADHD symptoms and then tics. Although one could also hypothesize that guanfacine might have some anxiolytic effects, it would be unlikely that it would target OCD symptoms directly like an SSRI. Both J.'s disruptive behavior and his tics may have responded if this had been initiated earlier in the course of his treatment. J. demonstrates the pharmacotherapeutic challenges of treating ADHD when TD is present (Sood & Coffey 2013). Following J.'s participation in group CBT for OCD, his clinician opted to taper his stimulant while titrating his SSRI and alpha-2 agonist. J. demonstrated a good response in terms of both anxiety and tic severity, without significant exacerbation of ADHD symptoms J.'s reduction of anxiety enabled him to resume his food intake, improved peer relations, and unrestricted thought and play.
J.'s marked response to ERP for his OCD was in contrast to his lack of response to parent management therapy. This generates another interesting point: not all disruptive behavior is a function of ADHD or oppositional defiant disorder (ODD). It is likely that at least some of J.'s disruptive and aggressive behavior was driven by anxiety and was a prelude to later onset tics and OCD symptoms. Temper outbursts are not uncommon in children with OCD (Geller et al. 1996; Krebs et al. 2013), with TD (Chen et al. 2013; Budman et al. 2003), as well as in those with the triad (Pollak et al. 2009; Stephens & Sandor 1999; Lebowitz et al. 2012).
Taken together, this case demonstrates the unique factors that must be considered when treating a child with the triad of ADHD, OCD, and TD. An accurate understanding of developmental psychopathology and diagnostic formulation will lead to an individualized targeted combined pharmacotherapy, and can yield significant benefit to the child and to his or her family.
Footnotes
Acknowledgments
We would like to acknowledge and thank Zoey Shaw for her assistance in review and preparation of the manuscript.
Disclosures
Dr. Rice has no conflicts of interest or financial ties to disclose. Dr. Coffey has received research support from Eli Lily Pharmaceutical, NIMH, NINDS, Tourette Syndrome Association, Otsuka, Shire, Bristol-Myers, Pfizer, and Boehringer Ingelheim.