
Abstract
Objectives:
To identify the prevalence of stimulant and antidepressant medication use by children and adolescents with symptoms meeting the criteria for attention-deficit/hyperactivity disorder (ADHD) and major depressive disorder (MDD) in Australia. To identify factors associated with stimulant and antidepressant use by children and adolescents in Australia.
Methods:
Data are from a nationally representative sample of 4- to 17-year-olds (n = 6310). Parents completed the Diagnostic Interview Schedule for Children—Version IV (DISC-IV) and the Strengths and Difficulties Questionnaire. Eleven- to 17-year-olds completed a self-report version of the DISC-IV MDD module. Interviewers recorded prescribed medications used by participants in the previous 2 weeks.
Results:
During a 2-week period, 1.3% of all 4- to 17-year-olds and 13.7% of those with symptoms meeting the criteria for ADHD had used stimulant medication, while 0.9% of all 4- to 17-year-olds and 13.4% with MDD had used antidepressants. In total, 22.6% of those using stimulant medications and 57.7% using antidepressant medications did not have symptoms meeting criteria for ADHD or MDD, respectively. Among 11- to 17-year-olds, 5.6% of those with adolescent-only-reported MDD, 10.9% of those with parent/carer-only-reported MDD, and 25.7% of those with MDD reported by both parents/carers and adolescents were using antidepressant medications.
Conclusions:
Only a minority of 4- to 17-year-olds with ADHD and MDD were being treated with stimulant or antidepressant medication. The percentage of adolescents with MDD using antidepressant medications varied depending on whether adolescents, parents/carers, or both identified the presence of MDD. This highlights the importance of using information from both these informants when assessing and treating adolescent depressive disorder.
Introduction
A
Information about the ways in which stimulant and antidepressant medications are being used to treat children in the general community is important for several reasons (for brevity, the term “children” will generally be used to refer to “children and adolescents” in this article). First, there is only limited evidence that antidepressant medications are effective when used to treat childhood depressive disorders (Hetrick et al. 2012). Second, while there is evidence that stimulant medications provide short-term benefits for attention-deficit/hyperactivity disorder (ADHD), evidence of longer term benefits is weaker (Thomas et al. 2013; Storebo et al. 2015). Third, both stimulant and antidepressant medications can cause important adverse side effects (Psychotropic Expert Group 2013; Taylor et al. 2015).
The percentages of children with ADHD and major depressive disorder (MDD) in the community treated with stimulant and antidepressant medications are unclear. In addition, there is little information about the number of children without these disorders who are being treated with these medications. These are significant omissions because accurate targeting of medications is important to ensure that all children with treatable disorders receive appropriate medications, while those without disorders are not exposed to inappropriate treatments and adverse side effects.
The few studies examining rates of stimulant treatment for children with ADHD in the community have reported markedly differing results (Jensen et al. 1999; Angold et al. 2000; Sawyer et al. 2002; Green et al. 2005; Froehlich et al. 2007; Visser et al. 2010; Olfson et al. 2013). In the United States, Jensen et al. (1999) reported that 12.5% of children meeting ADHD criteria had been treated with stimulant medication during the previous 12 months, while Angold et al. (2000) reported that over a 4-year period, 72% of children with ADHD were treated with stimulant medication. More recently, Olfson et al. (2013) used data collected in the 2002–2004 National Comorbidity Survey of 13- to 18-year-olds and reported that 27.5% of those using antidepressants in the past year had a past 12-month depressive disorder, while 27.1% had ADHD. Among those using stimulants, 49.1% had ADHD and 14.9% had a depressive disorder. Data reported in the article also indicate that 12.5% of those with a depressive disorder were using antidepressants and 16.1% of those with ADHD were using stimulants (Olfson et al. 2013). Using data collected in the National Health and Nutrition Examination Survey of 8- to 15-year-olds, Froehlich et al. (2007) reported that in 2001–2004, 38.8% of children who met the criteria for ADHD had been treated with stimulant medication during the past year and 32.0% were treated for most of the year. An important limitation of all these previous studies is that rates of stimulant use were based on data collected more than 10 years ago and may not reflect current practice.
There have been very few studies investigating rates of stimulant or antidepressant use by children with ADHD or MDD outside the United States. In Great Britain, Green et al. (2005) reported that 43% of children with a hyperkinetic disorder who participated in a national survey of child and adolescent mental health were using some kind of medication. The majority were taking methylphenidate (41%), with smaller numbers using risperidone (3%), dexamphetamine (2%), clonidine (1%), and amitriptyline (1%). In Australia, Sawyer et al. (2002) used data from a national survey of 6- to 17-year-olds in 1998 and reported that among those with symptoms meeting the criteria for ADHD, 12.6% were using stimulant medication. Among those without ADHD, 0.5% were using stimulant medication. Due to the large number of children in the survey who did not have ADHD, children who were taking stimulants but whose symptoms did not meet the criteria for ADHD comprised 23% of all children who were using stimulant medication.
The aim of the present study was to identify (1) the prevalence of stimulant and antidepressant medication use by 4- to 17-year-olds with ADHD and MDD in Australia and (2) factors associated with stimulant and antidepressant use by all 4- to 17-year-olds in Australia.
Methods
Participants
The design of the second Australian National Child and Adolescent Mental Health Survey has been described in detail elsewhere (Hafekost et al. 2015; Lawrence et al. 2015). In brief, the survey was conducted during 2013–2014 using a multistage area-based sample selection procedure to ensure proportional representation of geographic areas across Australia. A random probability-based sample of 6310 parents/carers of 4- to 17-year-olds (55% of eligible households) completed face-to-face interviews with trained field workers. Self-report questionnaires were completed by 2967 eleven- to seventeen-year-olds in these households (89% of eligible youth) via a tablet computer.
Compared with the 2011 Australian census, the participating sample contained a higher proportion of children aged 4–7 years and a higher proportion of children from families with more than one child aged 4–17 years. Otherwise, the distribution of the sample matched the population distribution from the 2011 census by demographic and socioeconomic characteristics, such as household income, carer employment status, place of birth, household tenure, family type, and socioeconomic status. The sample data were weighted to adjust for patterns in nonresponse and represent the full Australian population of 4- to 17-year-olds (Australian Bureau of Statistics 2014).
Measures
Mental disorders
ADHD and MDD were assessed using the Diagnostic Interview Schedule for Children—Version IV (DISC-IV) completed by parents or primary carers (Fisher et al. 1993; Shaffer et al. 2000). Modules in the DISC-IV identify mental disorders on the basis of diagnostic criteria specified in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) using a structured diagnostic interview that can be used by lay interviewers (American Psychiatric Association 1994, 2000). Both current and 12-month mental disorders can be identified using the DISC-IV. A self-report version of the DISC-IV module for MDD was completed by 11- to 17-year-olds (Hafekost et al. 2015). The DISC-IV was also used to identify children with anxiety disorders and conduct disorder. However, to keep participant burden to reasonable proportions, other mental disorders were not assessed in the survey.
Mental health problems
Level of mental health problems was assessed using the Strengths and Difficulties Questionnaire (SDQ) completed by parents (Goodman 1997, 2001). The total SDQ score ranges between 0 and 40 (borderline cutoff >13). Subscales assess difficulties with hyperactivity (borderline cutoff >5), conduct problems (borderline cutoff >2), peer problems (borderline cutoff >2), and emotional symptoms (borderline cutoff >3). All subscale scores ranged between 0 and 10. The SDQ has excellent psychometric properties (Goodman 1997, 2001; Hawes and Dadds 2004).
Assessment of medication use
Parents/carers were asked to show field workers all prescription medications taken by children in the 2 weeks before the children's assessments. For the purpose of the study, medications coded as Anatomical Therapeutic Chemical (ATC) code N06B were classified as stimulant medications (World Health Organisation 2015). These included methylphenidate, dexamphetamine, and atomoxetine. All medications coded as ATC-N06A were categorized as antidepressant medication. These included imipramine, clomipramine, amitriptyline, nortriptyline, dothiepin/dosulepin, fluoxetine, citalopram, sertraline, fluvoxamine, escitalopram, mirtazapine, venlafaxine, duloxetine, and desvenlafaxine.
Sociodemographic characteristics
Sociodemographic characteristics were recorded, including family type and household income, using the Australian Bureau of Statistics standard formats (Lawrence et al. 2015).
Analysis of results
For the purpose of statistical analyses, children whose symptoms met the criteria for ADHD or MDD were categorized into the relevant diagnostic group. Among these, 42/603 (7.0%, 95% confidence interval [CI] = 5.0–9.5) children were comorbid for ADHD and MDD. In addition, for each SDQ scale, children were categorized into one of the two groups according to whether they scored above or below the borderline cutoff score on the SDQ scale.
All analyses were undertaken using Stata version 14.0 and accounted for the multistage survey design using the clustered sandwich estimator when calculating variances, standard errors, and CIs (StataCorp 2015). This adjusts for potential correlation between survey responses for individuals living within the same sampled geographic area (Australian Bureau of Statistics 2014; Hafekost et al. 2015; Lawrence et al. 2015). Factors associated with service use among children with disorders were assessed using multiple logistic regression methods. Differences with nonoverlapping 95% CIs were treated as statistically significant.
Ethics clearance
The research protocol for the study was approved by the Australian Government Department of Health Human Research Ethics Committee and The University of Western Australia Human Research Ethics Committee.
Results
All 4- to 17-year-olds
During the 2 weeks before the survey, 1.3% (95% CI = 0.9–1.7) of 4- to 17-year-olds had used stimulant medication and 0.9% (95% CI = 0.7–1.1) had used antidepressant medication. Only two sociodemographic characteristics differed significantly across groups for children using antidepressant or stimulant medication, with bivariable logistic regression indicating that females had less frequently used stimulant medication (OR: 0.21, 95% CI = 0.11–0.39), while older children had more frequently used antidepressant medication (OR: 8.21, 95% CI = 3.23–20.90) (Table 1).
All characteristics were reported by the parent. All ns rounded after weighting.
Any school service use in last 12 months; excludes participants not in school (n = 255).
ADHD, attention-deficit/hyperactivity disorder; CI, confidence interval; MDD, major depressive disorder; OR, odds ratio; SDQ, Strengths and Difficulties Questionnaire.
Children who had attended health and/or school services during the previous 12 months were more frequently using stimulant and antidepressant medications than those who had not attended these services. For example, 21.7% (95% CI = 16.0–28.8) of children attending pediatricians were using stimulant medication and 8.2% (95% CI = 5.3–12.3) were using antidepressant medication, while 22.2% (95% CI = 15.1–31.4) of children attending psychiatrists were using antidepressant medication and 10.9% (95% CI = 5.6–20.0) were using stimulant medication (Table 1). There was also a consistent pattern for children with SDQ scores above the borderline cutoff score to more frequently be using stimulant and antidepressant medications than those with scores below the cutoff.
4- to 17-year-olds with ADHD and/or MDD
Among children whose symptoms met the criteria for ADHD, 13.7% (95% CI = 10.1–18.1) had used stimulant medication and 2.6% (95% CI = 1.4–4.7) had used antidepressant medication (Table 1). Among those whose symptoms met the criteria for MDD, 13.4% (95% CI = 9.0–19.4) had used antidepressant medication and 4.4% (95% CI = 2.0–9.6) had used stimulant medication. Among those with comorbid ADHD and MDD, 9.0% (95% CI = 2.8–25.3) had used antidepressant medication and 18.5% (95% CI = 8.5–35.8) had used stimulant medication (Table 1).
Only 0.3% (95% CI = 0.2–0.5) of 4- to 17-year-olds without ADHD were being treated with stimulant medication. Similarly, only 0.5% (95% CI = 0.4–0.7) of those without MDD were being treated with antidepressant medication. However, due to the large number of 4- to 17-year-olds in these groups, in total, 22.6% (95% CI = 14.7–33.3) of those using stimulant medications and 57.7% (95% CI = 44.6–69.9) using antidepressant medications did not have symptoms that met the diagnostic criteria for ADHD or MDD, respectively.
The average SDQ hyperactivity and emotional symptoms scores were similar for children using stimulant medication regardless of whether or not their problems met the criteria for ADHD (Table 2). The mean SDQ scores of these children were also significantly higher than scores reported for children whose problems did not meet ADHD criteria and who were not using stimulant medication. The average SDQ scores for children using antidepressant medication were similar on all four SDQ subscales regardless of whether or not their problems met the criteria for MDD (Table 2). The mean scores of these children were also significantly higher than scores reported for children whose problems did not meet MDD criteria and who were not using antidepressant medication (Table 2).
Number of participants with MDD differs from the total reported in Table 1 due to rounding after weighting.
ADHD, attention-deficit/hyperactivity disorder; CI, confidence interval; MDD, major depressive disorder; SDQ, Strengths and Difficulties Questionnaire.
None of the children with a conduct disorder that was not comorbid with ADHD (n = 66) was using stimulants. Furthermore, only 1.1% (95% CI = 0.3–4.0) of children with an anxiety disorder not comorbid with ADHD (n = 302) were using stimulants. Among children with an anxiety disorder not comorbid with MDD (n = 334), 3.0% (95% CI = 1.7–5.4) were using antidepressants. Among children with a conduct disorder not comorbid with MDD (n = 107), 0.6% (95% CI = 0.1–3.9) were using antidepressants.
Multivariable analyses for all 4- to 17-year-olds
Results from the multivariable logistic regression analyses examining the strength of the association between medication use and the diagnostic and sociodemographic variables are shown in Table 3. It can be seen that the presence of ADHD or MDD had the strongest positive association with stimulant and antidepressant use, respectively. Female gender had a significant negative association with stimulant use, while age had a significant positive association with the use of antidepressant medication. In the multivariable models, children with SDQ hyperactivity and conduct problems scores above the borderline cutoff had an increased likelihood of stimulant use compared with those with scores in the normal range, after adjusting for the effect of diagnosis. Similarly, children with SDQ peer problems and emotional symptoms scores above the borderline cutoff had an increased likelihood of antidepressant use. The findings suggest that children with higher levels of symptoms in these areas were more likely to be using medication than those with lower levels, after adjusting for the effect of diagnosis.
Reference category is children without the disorder.
Reference category is children scoring below the borderline cutoff.
ADHD, attention-deficit/hyperactivity disorder; CI, confidence interval; MDD, major depressive disorder; ref, reference category; SDQ, Strengths and Difficulties Questionnaire.
11- to 17-year-olds with MDD
The percentage of 11- to 17-year-olds with parent- and/or adolescent-reported MDD who were using antidepressant medication is shown in Figure 1. The lowest percentage of adolescents using antidepressants occurred when the adolescent but not their parent reported symptoms meeting the criteria for MDD (5.6%, 95% CI = 3.3–9.1). The highest percentage (25.7%, 95% CI = 15.9–38.6) was using antidepressants when both the parent and the adolescent reported that the adolescent had symptoms meeting the criteria for MDD. When the parent but not the adolescent reported that the adolescent had symptoms consistent with a diagnosis of MDD, 10.9% (95% CI = 5.6–20.4) of adolescents were using antidepressants.
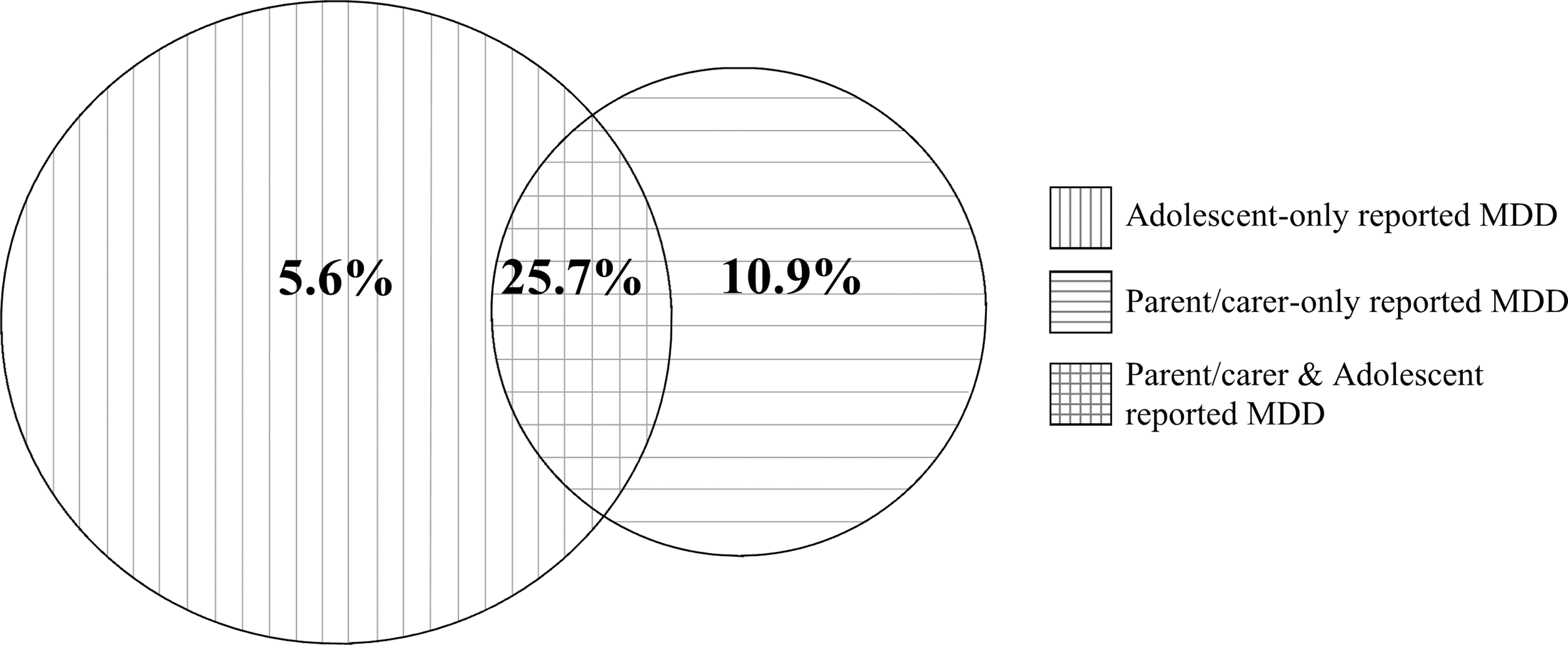
Percentage of adolescents with MDD reported by parents/carers and/or adolescents who were using antidepressant medication. The areas of the overlapping circles reflect the prevalence of MDD in the survey reported by (1) adolescents (5.8%), (2) parents/carers and adolescents (1.9%), and (3) parents/carers (2.8%). MDD, major depressive disorder.
If information about MDD symptoms was limited to that provided by parents (i.e., information from adolescents was not used), 16.8% (95% CI = 11.2–24.5) of adolescents identified as having MDD were using antidepressants. When only information from adolescents was used for this purpose, 10.5% (95% CI = 7.3–14.9) of adolescents identified as having MDD were using antidepressants.
Sensitivity analyses
We conducted two sensitivity analyses to assess the robustness of the findings we have reported. In the first sensitivity analysis, we examined the prevalence of medication use by children whose symptoms met the criteria for “current” ADHD and MDD. In the analyses described earlier, it was possible that children had ADHD or MDD up to 12 months before medication use was assessed. As such, it was possible (although unlikely) that their current use of medication was unrelated to this earlier problem. The first sensitivity analysis provides some reassurance that this possibility was not biasing estimates of current medication use. For the purpose of the analysis, children were considered to have a current disorder if they met the criteria for ADHD or MDD within the month before the survey. When this definition was used to identify those with a disorder, 15.6% (95% CI = 11.3–21.1) of children with ADHD were found to have used stimulant medication during the previous 2 weeks and 11.5% (95% CI = 4.5–26.5) with MDD had used antidepressant medication. These estimates vary little from those reported for 12-month ADHD and MDD.
In the second sensitivity analysis, we used linked data from the administrative records of medicines dispensed through the Pharmaceutical Benefits Scheme (PBS) in Australia. The analysis provides information about the extent to which stimulant and antidepressant medications were dispensed to children with symptoms that met the criteria for ADHD or MDD rather than the extent to which children were using the medications. The PBS provides access to a broad range of government-subsidized medications, including all stimulants and antidepressants reported in the present article. The linked data contain details of the dispensing of medications under the scheme, excluding medications supplied by hospitals or nonapproved pharmacies (a very small minority of pharmacies) (Page et al. 2015). Consent to access PBS data was obtained from parents, where the survey child was aged younger than 14 years and from adolescents themselves aged 14–17 years for a total of 4928 households (78%).
We examined stimulant and antidepressant medications dispensed in the 12 months before the survey. However, it should be noted that at the time this analysis was conducted only PBS data up to December 31, 2013, could be linked. As such, only participants who consented and who completed their survey by this time were included in this analysis (n = 3921). Based on results from this group, we estimate that 2.0% (95% CI = 1.5–2.6) of all children in Australia had been dispensed stimulant medication during the previous year and 0.7% (95% CI = 0.5–1.1) had been dispensed antidepressant medication. Among those with 12-month parent-reported ADHD, 20.3% (95% CI = 15.3–26.5) had been dispensed stimulant medication and 12.9% (95% CI = 6.4–24.2) of those with MDD had been dispensed antidepressant medication. When combined with information about children's medication use collected directly in the survey, this suggests that compared to those dispensed stimulants, a higher proportion of 4- to 17-year-olds dispensed antidepressants were taking their medication at the time of the survey.
Discussion
There were four key findings in the present study. First, only a small proportion of children in the general community were using stimulant or antidepressant medications, and current use varied little from that reported in the first Australian National Child and Adolescent Mental Health Survey (first survey: stimulant use = 1.8%, 95% CI = 1.5–2.3; antidepressant use = 0.4%, 95% CI = 0.2–0.6; second survey: stimulant use = 1.3%, 95% CI = 1.0–1.7; antidepressant use = 0.9%, 95% CI = 0.7–1.1) (Sawyer et al. 2002). Males were more likely to be receiving stimulant medication than females, and older children were more likely to be receiving antidepressant medication than younger children. These findings are consistent with several earlier studies (Fegert et al. 2006; Zito et al. 2006; Galera et al. 2014).
Second, only a minority of 4- to 17-year-olds with symptoms meeting the criteria for MDD or ADHD in the present study were being treated with antidepressant or stimulant medication. Furthermore, the percentage of those with ADHD being treated with stimulant medication in 2013–2014 (13.7%, 95% CI = 10.1–18.1) differed little from that identified in 1998 in Australia (12.6%, 95% CI = 9.8–16.1) (Sawyer et al. 2002). Although the study does not provide information about the appropriateness of dosage levels being prescribed for individual children with ADHD, the results suggest that at a population level, the use of stimulant medication to treat children with ADHD in Australia has not increased. As noted earlier, the percentage of children with ADHD using stimulant medication in previous studies has varied substantially (Jensen et al. 1999; Angold et al. 2000; Froehlich et al. 2007). Furthermore, within the same study in the United States, marked variations have been reported for children living in different regions, with 19% of children with ADHD reported as using stimulants in Oklahoma and 45% in South Carolina (Wolraich et al. 2014). Large variations in the extent to which stimulant and antidepressant medications are dispensed in different geographical regions of Australia have also been reported (Australian Commission on Safety and Quality in Health Care 2015). The percentage of children with ADHD using stimulants in the present study is consistent with those reported in two of the three studies conducted in the United States (Jensen et al. 1999; Froehlich et al. 2007) but substantially lower than the third study (Angold et al. 2000).
Third, the percentage of adolescents with symptoms meeting the criteria for MDD who were using antidepressant medication varied depending on the informant reporting the adolescent's symptomatology. The highest percentage (25.7%, 95% CI = 15.9–38.6) occurred when both parents/carers and adolescents reported symptomatology consistent with MDD and the lowest (5.6%, 95% CI = 3.3–9.1) when only self-reported problems met the criteria for the disorder. It seems likely that this difference reflects the key role that parents play in facilitating access to health services by adolescents with mental disorders. It also suggests that medical practitioners are more likely to prescribe medication when there is consistency in the information provided by parents and adolescents about adolescents' diagnostic status. Finally, the finding highlights the importance of obtaining information about depressive symptoms from both parents and adolescents when assessing and treating adolescent mental disorders. It cannot be assumed that information from one of these informants necessarily reflects the views of the other.
Fourth, as an absolute number, the majority of children in the present survey who were using stimulant medication or antidepressant medication did not have the symptoms required to meet the criteria for a diagnosis of ADHD or MDD. However, many of these children had a high level of emotional and behavioral problems comparable to that reported for children whose symptoms met these diagnostic criteria. This finding is consistent with results describing stimulant medication use in the previous Australian survey (Sawyer et al. 2002). It is also consistent with results from the national survey conducted in Great Britain, where it was reported that all the children taking stimulant medication had pervasive hyperactivity (i.e., overactivity, impulsiveness, and inattention) (Green et al. 2005).
Finally, although assessing the prevalence of medication treatment for children with anxiety disorders was not a core aim of this study, it is noteworthy that only a very small proportion of children with anxiety disorders not comorbid with MDD were being treated with antidepressants. This is surprising given evidence that selective serotonin reuptake inhibitors can be a useful treatment for anxiety disorders (Ipser et al. 2009).
Due to differences in participants' ages, the years when studies were conducted, the methodologies used to identify children with disorders, and the medications they were using, caution is needed when interpreting the meaning of differences in the estimated prevalence of psychotropic medication use in different studies. For example, the present study reported the prevalence of stimulant medication use across a 2-week period, while studies in the Netherlands and the United States reported the prevalence across 12-month periods. Furthermore, consistent with many studies, the present study lacked information from teachers about the functioning of children in the school environment. It is possible that the higher prevalence of stimulant use by children and adolescents reported in the Netherlands (2.1%) (Hodgkins et al. 2011) and both stimulant use (2.8%–3.5%) (Zuvekas and Vitiello 2012; Olfson et al. 2013) and antidepressant use in the United States (3.9%) (Olfson et al. 2013) compared with Australia reflect a lower use of psychotropic medication in Australia. However, it may also be due to the shorter period over which medication use was assessed in the present study or the different ways in which the presence of ADHD was identified in the three other studies (Hodgkins et al. 2011; Zuvekas and Vitiello 2012; Olfson et al. 2013).
Strengths of the present study are its use of a large nationally representative sample of 4- to 17-year-olds and the careful checking of medications by interviewers to ensure accuracy of reporting. Weaknesses include a lack of information from teachers about children's functioning at school and the absence of information about the effectiveness of the medications being used to treat the children's disorders. The study also provides only limited information about the extent to which children being treated with stimulant or antidepressant medication had mental disorders other than those assessed in the national survey. Finally, it is possible that children taking medication in the present study did not meet the criteria for MDD or ADHD because their problems had already responded to medication treatment. Information is available about this issue in a prospective study of 9- to 16-year-olds (n = 4500) in the community in which children's level of ADHD symptomatology had been evaluated in an earlier study assessment before they commenced taking stimulant medication (Angold et al. 2000). This showed that of the children taking stimulant medication who did not meet the criteria for ADHD (n = 270) at the time their medication use was evaluated, 71% did not have symptoms of ADHD at the earlier assessment preceding their commencement of stimulant medication. This suggests that treatment response to stimulant medication is unlikely to be the primary reason why many of the children in our study did not have symptoms meeting the criteria for ADHD at the time of their assessment for the national survey.
Conclusion
Treatment guidelines used in Australia recommend that nonmedication approaches be used for the management of MDD and ADHD before treatment with medication is considered (McDermott et al. 2010; Psychotropic Expert Group 2013; NICE 2015, 2016). It is possible that this explains the modest prevalence of medication use among children with these disorders identified in the present study. However, the results also highlight the continuing challenges faced by medical practitioners, parents, and children in an area where there have been few high-quality trials to guide clinical practice, where symptoms reported by parents and adolescents may differ greatly, and where it is often difficult to judge the likely benefits versus disadvantages of initiating a course of medication treatment for an individual child or adolescent referred for help.
Clinical Significance
Information about the ways in which stimulant and antidepressant medications are used to treat children and adolescents in the general community is important because (1) there is limited evidence that antidepressant medications are effective treatments for childhood depressive disorders, (2) although stimulant medications appear to have short-term benefits for ADHD, evidence of longer term benefits is weaker, and (3) both medications can cause important adverse side effects. Accurate targeting of medications is important to ensure that all children with treatable disorders receive appropriate medications, while those without disorders are not exposed to inappropriate treatments and adverse side effects.
Footnotes
Acknowledgments
The authors thank David Ellis, BPharm, Women's and Children's Health Network, for helpful pharmacological advice and Jennifer Hafekost, BSSc, DipEd, Telethon Kids Institute, for technical advice about the survey.
Disclosures
No competing financial interests exist.