
Abstract
Objective:
Attention-deficit/hyperactivity disorder (ADHD) is a chronic neurodevelopmental disorder. Due to lack of response to the medication and significant side effects of the treatment with stimulants, alternative medications should be considered. The aim of this study is to evaluate efficacy of agomelatine in treatment of ADHD.
Methods:
Fifty-four outpatients, children 6–15 years old, with diagnosis of ADHD according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) diagnostic criteria participated in a 6-week, parallel, double-blind, randomized clinical trial. Fifty patients completed 6 weeks of treatment with either ritalin (methylphenidate hydrochloride [MPH]) (20 mg/day in participants below 30 kg and 30 mg/day in patients with weight ≥30 kg) or agomelatine (15 mg/day in patients with weight ≥30 kg and 25 mg/day in patients with weight ≥45 kg). Participants were assessed using Parent and Teacher ADHD Rating Scale-IV at baseline and at weeks 3 and 6.
Results:
General linear model repeated measures showed no significant differences between the two groups on Parent and Teacher Rating Scale scores (F = 1.13, df = 1.26, p = 0.305, and F = 0.95, df = 1.25, p = 0.353, respectively). Changes in Teacher and Parent ADHD Rating Scale scores from baseline to the study end were not significantly different between the agomelatine group (9.28 ± 8.72 and 24.12 ± 7.04, respectively) and the MPH group (6.64 ± 11.04 and 25.76 ± 7.82, respectively) (p = 0.46 and p = 0.44, respectively). There was a trend for less insomnia in the agomelatine group versus MPH-treated group (4% vs. 24%, p = 0.09).
Conclusions:
A treatment course of 6 weeks with agomelatine demonstrated a favorable safety and efficacy profile in children and adolescents with ADHD. Nonetheless, larger controlled studies with longer treatment periods are necessary.
Introduction
A
Antidepressants have been reported to be effective in improving the symptoms of ADHD (Akhondzadeh et al. 2003; Tehrani-Doost et al. 2008; Zarinara et al. 2010; Niederhofer 2012). Agomelatine, a relatively new antidepressant, is a 5HT2c receptor antagonist, with additional agonist activity at the melatonergic MT1 and MT2 receptors, which are responsible for the circadian rhythm (Racagni et al. 2011). These advantages of agomelatine are proposed to be derived mostly by its ability to increase both Norepinephrine and Dopamine at frontocortical dopaminergic and adrenergic pathways, as well as its sleep-enhancing properties due to MT1 and MT2 potent agonist characteristics (Navailles et al. 2004; San and Arranz 2008; Fornaro et al. 2010; Quesseveur et al. 2012; Alamo et al. 2014). Having the property to affect both the catecholaminergic neurotransmission and the circadian rhythm qualifies agomelatine as a possible candidate for the treatment of ADHD. To the best of our knowledge, there is no previous study on the potential applications of agomelatine in children.
One study has investigated the efficacy of agomelatine in the treatment of late adolescents with ADHD, but not in children (Niederhofer 2012). In this study, we evaluate the efficacy of agomelatine in treatment of ADHD in children and adolescents compared with methylphenidate in a double-blinded clinical trial.
Methods
Trial design and setting
This study was a 6-week, single-center, randomized, double-blind, parallel-group clinical trial conducted from January 2014 to November 2015 on outpatients of the child and adolescent clinics at the Roozbeh Psychiatric Hospital affiliated with Tehran University of Medical Sciences (TUMS). The protocol was approved by the institutional review board (IRB) of TUMS (Grant No: 23222) and was in consistence with the Declaration of Helsinki and its successive revisions. After a complete description of the procedures and the purpose of the study, written informed consent was obtained from the patients or their legal guardian. It was declared to each patient and their guardian that they were free to withdraw from the trial without any negative effect on their treatment. This trial was registered at the Iranian registry of clinical trials (
Participants
Patients were recruited from outpatient girls and boys between ages 8 and 17 who met the criteria for ADHD based on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) (American Psychiatric Association 2000). The subjects had to have total and/or subscale scores of at least 1.5 standard deviations (SDs) above normal for the patient's age and gender on Attention-Deficit/Hyperactivity Disorder Rating Scale-IV (ADHD-RS-IV) to be included in the study (DuPaul and Power 1998). The diagnosis of ADHD was confirmed by the participant's child psychiatrist before initiation of the study based on the DSM-IV-TR criteria for ADHD, the Kiddie Schedule for Affective Disorders, and Schizophrenia-Present and Lifetime diagnostic interview and a thorough medical evaluation was performed (Ghanizadeh et al. 2006).
A complete medical history was taken and a thorough physical examination was performed. All patients were newly diagnosed and had combined subtype of the disease. Parents were interviewed carefully before admission to the trial. They were asked to rate the severity of the symptoms according to the ADHD-RS-IV based on the behavior of their children at home. The exclusion criteria included DSM-IV axis I psychiatric disorder comprising schizophrenia, history or current diagnosis of pervasive developmental disorders, any evidence of suicide risk, mental retardation (defined as intelligence quotation below 70), current psychiatric comorbidity except for oppositional defiant disorder, clinically significant chronic medical condition, including seizure and organic brain disorder and/or cardiac abnormalities, use of any medication that might have affected the patient's psychiatric condition in the past 2 weeks, and drug abuse or dependency in the past 6 months. Additionally, it was especially considered that the blood pressure, the pulse rate, and the liver function test of the participants were in the clinically normal range.
Intervention
Eligible subjects were randomly assigned to receive ritalin (methylphenidate hydrochloride [MPH]) at a dose of 1–1.25 mg/(kg·day) or up to 25 mg of agomelatine for 6 weeks. Patients in the MPH group received 5 mg MPH twice daily for the first week, followed by a 10 mg tablet twice daily for the rest of the trial. Patients who weighed more than 30 kg, received a 10 mg MPH tablet thrice daily from the second week of the study. Agomelatine was started as 15 mg/day in participants with weight ≥30 kg and 25 mg/day in patients with weight ≥45 kg in the morning and followed by placebo at lunch time. Medication adherence was measured by comparison of weekly tablet counts with participant reports of medication intake to estimate the proportion of dispensed medication that was actually ingested.
Outcome
Symptoms were rated using the Parent and Teacher ADHD-RS-IV at baseline and weeks 3 and 6 (DuPaul et al. 1998). The ADHD-RS-IV has been used extensively in Iran and offers valid measurement of attention and behavioral problems in school-age children (Kahbazi et al. 2009; Mohammadi et al. 2010, 2012; Abbasi et al. 2011; Jafarinia et al. 2012). It assesses the 18 symptoms of ADHD based on DSM-IV-TR on a 4-point scale. The primary outcome measure was the change in the scores of the parent version of ADHD-RS-IV from baseline to week 6 in each group. Secondary outcome measures were the change in scores of the teacher version of ADHD-RS-IV and response rate in each group.
Safety
All patients underwent a complete physical exam, psychiatric evaluation, assessment of medical history, electrocardiogram (ECG), liver function tests, and complete blood count (CBC) evaluations at the screening session. Moreover, a thorough medical examination was performed at the end of the study, and a 12-lead ECG and serum chemistry and hematology tests were also taken. Body weight and vital signs were measured at baseline and at each visit. Participants were asked to immediately inform the research team in case of any unexpected symptom or complaint during the study period. They were systematically asked for any side effects during the course of study using a checklist administered by a child psychiatrist at each visit as well.
Sample size
Based on the assumption of a mean difference (MD) of 5 on the Teacher and Parent ADHD Rating Scale, an SD of 5 on the Teacher and Parent ADHD Rating Scale (according to the pilot study), a power of 90%, and a two-tailed significance level of 0.05, a sample size of 46 was calculated. Assuming a 15% attrition rate, a total sample size of 54 was estimated.
Randomization, allocation concealment, and blinding
Participants were randomized by the permuted randomization block method using a computer-generated code (allocation ratio 1:1). The MPH and agomelatine tablets were identical in all their properties. The person dispensing the drug, the patient, the physician who referred the patient, the rater, and the statistical analyzer were all blinded to allocation. The allocation was carried out using sealed, opaque, and stapled envelopes with an aluminum foil inside in each envelope to make the content of the envelope unrecognizable in intense light.
Statistical analysis
Statistical Package of Social Science Software (SPSS version 22; IBM Company) was used to carry out the statistical analysis. Continuous and categorical variables were reported in the form of mean ± SD and frequency (%), respectively. General linear model repeated measure was used to compare ADHD Rating Scale scores between treatment groups during the study course. The two groups were considered as a between-subject factor, while the three measurements were counted as within-subject factor. Whenever Mauchly's test of sphericity was significant, Greenhouse–Geisser correction was used for degrees of freedom. In addition, a one-way measure analysis of variance with a two-tailed post hoc dependent t-test was performed to evaluate efficacy of each protocol on reduction of ADHD Rating Scale scores. Differences accounted significance whenever the p-value was equal or below 0.05. To compare categorical variables between the two groups, the chi-square test and Fisher's exact test were used.
Results
Participants
Among 95 participants who were screened for the eligibility criteria, 54 participants entered the trial and were randomized to receive either MPH (n = 27) or agomelatine (n = 27). In each group, two patients left the study before the first meeting on the 21st day due to lack of parent collaboration. This was excluded from the final analysis (Fig. 1). No significant differences were observed in regard to basic characteristics of subjects such as age, gender, and ethnicity between the two groups (Table 1).
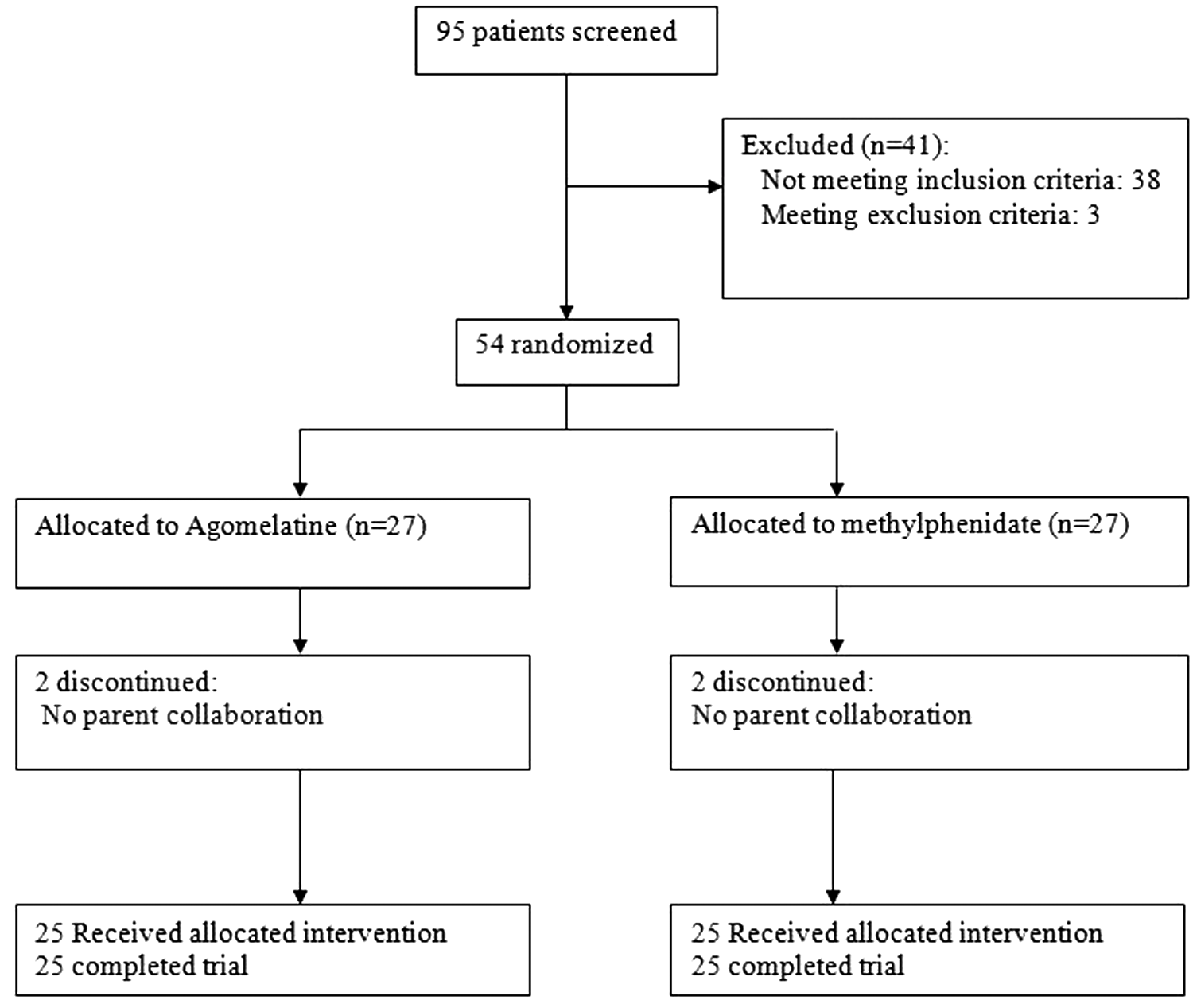
Flow diagram of the study.
SD, standard deviation; ADHD, attention-deficit/hyperactivity disorder.
Outcomes
The Parent ADHD Rating Scale
There was no significant difference in baseline Parent ADHD Rating Scale scores between the agomelatine and the MPH groups (33.12 ± 4.91 vs. 34 ± 6.89, respectively, MD [95% CI] = −0.88 [−4.28 to 2.52], t [−0.52], df = 48, p = 0.606). General linear model repeated measures showed no significant effect for treatment (between-subject factor) (F = 0.18, df = 1, p = 0.673) and time × treatment interaction (F = 1.13, df = 1.26, p = 0.305) as both treatment groups displayed a similar trajectory in declining ADHD symptoms over the 6-week period (Fig. 2). In both the agomelatine and the MPH groups, a one-way repeated measure ANOVA demonstrated a significant effect of time on Parent ADHD Rating Scale scores (F = 222.55, df = 1.44, p < 0.001, and F = 252.03, df = 1.10, p < 0.001, respectively). In addition, post hoc comparisons in these protocols showed significant improvement in Parent ADHD scores as soon as week 3 (p < 0.001). The difference between the two protocols was not significant at weeks 3 and 6. The difference was not significant either for Inattentive or Hyperactive/Impulsive subscales (Table 2). Parent ADHD Scale score changes at the endpoint from baseline were 24.12 ± 7.04 and 25.76 ± 7.82 for agomelatine and MPH, respectively. There was no significant difference between the reduction of scores at week 6 compared with baseline in the two treatment groups (t = −0.77, df = 48, p = 0.440). The difference between MPH and agomelatine groups in terms of responders (those with least 40% decrease in Parent ADHD Rating Scale score between the baseline and the endpoint) was not significant (92%, 23 of 25 for agomelatine vs. 96%, 24 of 25 for MPH) (p = 1.000). Agomelatine and MPH groups displayed an identical rate of robust improvement, 88% displayed 50% reduction in ADHD symptoms based upon parent ratings and a similar rate of robust improvement in teacher ratings (48% vs. 56%, respectively, p = 0.57)

Repeated measure for comparison of the effects of two treatments on Teacher ADHD Rating Scale score. Values represent mean ± standard error of mean. NS indicates nonsignificant; ADHD, attention-deficit/hyperactivity disorder.
ADHD, attention-deficit/hyperactivity disorder; SD, standard deviation.
Teacher ADHD Rating Scale
There was no significant difference in terms of Teacher ADHD Rating Scale scores at baseline between agomelatine and MPH treatment groups (23.52 ± 8.29 vs. 24.08 ± 10.78, MD [95% CI] = −0.56, respectively, [−6.03 to 4.91], t = −0.206, df = 48, p = 0.838). Difference between the two treatments was not significant as indicated by the effect of group investigated by general linear model repeated measures (F = 0.21, df = 1, p = 0.643). The trend of the two treatment groups was similar across time as was shown in the effect of time × treatment interaction (F = 0.95, df = 1.25, p = 0.353) (Fig. 3). Additionally, a significant effect of both treatments on improving Teacher ADHD Rating Scale scores was indicated (p < 0.001 for agomelatine and p = 0.003 for MPH). In both groups, post hoc comparisons of Teacher ADHD Rating Scale showed a significant reduction as soon as week 3. There was no significant difference between the treatment groups at the endpoint (p = 0.869). This observation was similar for both Inattentive and Hyperactive/Impulsive subscales (Table 2). The reductions at the endpoint compared with baseline were 9.28 ± 8.72 and 6.64 ± 11.04 scores for agomelatine and MPH, respectively. No significant difference was observed on the score reductions of the Teacher ADHD Rating Scale at week 6 compared with baseline in the two groups (p = 0.466). The responder rate (defined by at least 40% decrease in Teacher ADHD Rating Scale scores) was not significant between agomelatine and MPH groups (agomelatine: 52%, 13 of 25, and MPH 56%, 14 of 25) (p = 0.777). The marked improvement (defined by at least 50% decrease in Teacher ADHD Rating Scale scores) was not significant between agomelatine and MPH groups (agomelatine: 48%, 12 of 25, and MPH 56%, 14 of 25) (p = 0.571).
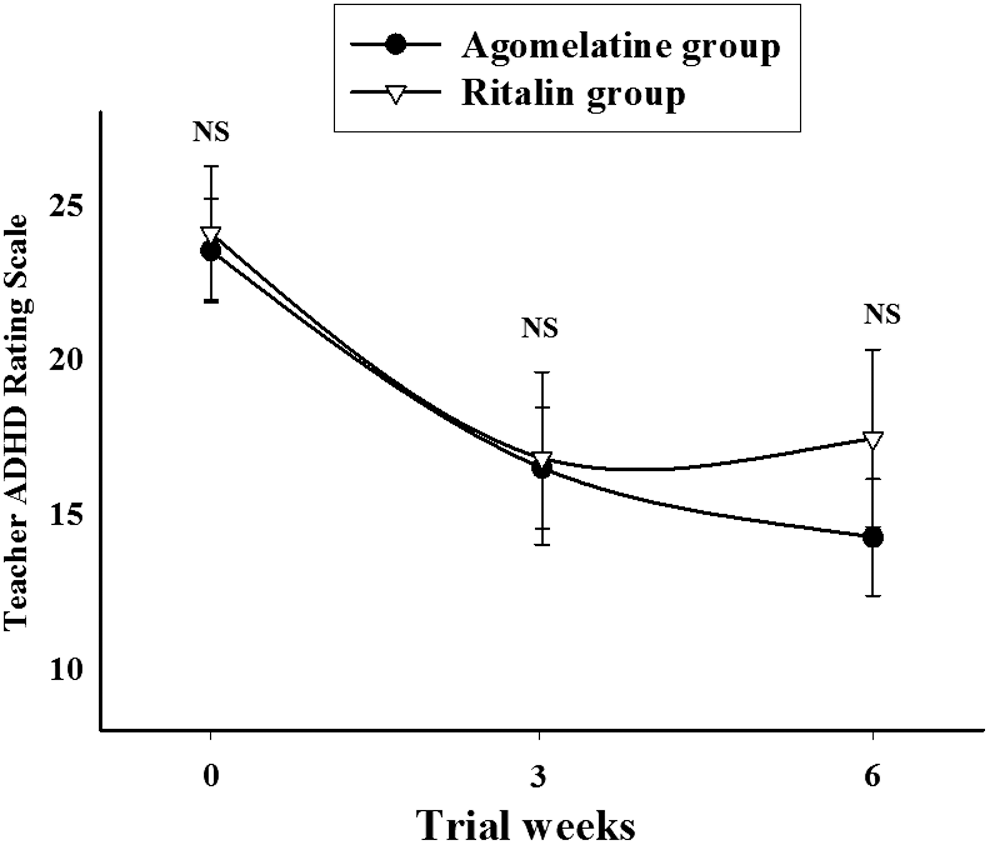
Repeated measure for comparison of the effects of two treatments on Teacher ADHD Rating Scale score. Values represent mean ± standard error of mean. NS indicates nonsignificant; ADHD, attention-deficit/hyperactivity disorder.
Adverse events
A number of the most probable side effects were studied (Table 3). No serious adverse event was observed and all noticed adverse effects were mild to moderate and tolerable. The frequency of side effects was not significantly different between the agomelatine and MPH groups. CBC elements and serum aminotransferase levels did not differ significantly between the two groups during the trial and at the study endpoint (Table 4).
RBC, red blood cell; WBC, white blood cell; HB, hemoglobin; Hct, hematocrit; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
Discussion
This double-blind randomized study addresses the safety and efficacy of agomelatine in children and young adults with ADHD. This study showed that agomelatine is effective in the treatment of ADHD, which is comparable with the stimulant drug MPH. Statistically significant effect of both agomelatine and MPH administrations on ADHD symptoms was demonstrated with no significant difference between the two treatments on the Parent and Teacher Rating Scale scores. Agomelatine also appeared to be safe and well tolerated. More specifically, agomelatine showed equally or less adverse effects even more often in comparison with MPH especially regarding insomnia.
The present results are in agreement with a previous study by Niederhofer conducted on 10 patients with ADHD Diagnostic and Statistical Manual of Mental Disorders, 3rd edition, revised (DSM-III-R) (American Psychiatric Association 1987) in a placebo-controlled trial, which demonstrated the superior effect of agomelatine compared with placebo in ADHD patients. It was mentioned that a spectrum of ADHD patients with associated oppositional defiance may benefit more and respond preferentially to agomelatine. Niederhofer concluded that agomelatine may be useful as a second-line medication especially if some level of additional sleep disorder coexisted (Niederhofer 2012).
In another study, Naguy et al. (2015) reported a 13-year-old female who was a case of severe ADHD, with an average response to methylphenidate, and who suffered from stimulant-related anxiety and insomnia, remarkably showing improvement of both anxiety and insomnia accompanied by improvement of ADHD symptoms and better academic performance after augmentation with agomelatine.
Considering Niederhofer's proposal, the possibility of better response with a combination of agomelatine and the current first-line medication, which was also confirmed by the sole case report mentioned earlier and our present findings, we suggest further evaluation of an augmentation therapy of both agomelatine and stimulants in the future studies. In addition, another positive property mentioned for agomelatine in some previous studies is withdrawal effect, although this property was related to its antidepressant effects (San and Arranz 2008; Chung et al. 2009; Fornaro et al. 2010).
Agomelatine is a drug with MT1/MT2 melatonergic receptor agonist and 5-HT2c receptor antagonist properties, which is currently utilized as an approved medication for depressive mood disorders. Moreover, agomelatine seems to have anxiolytic and analgesic effects with capability of improving sleep disorders and Parkinson's disease (Chung et al. 2009; Fornaro et al. 2010; Blier and El Mansari 2013; Alamo et al. 2014; Avila et al. 2015). Furthermore, recent research showed effects of agomelatine on cellular processes by increasing the expression of brain-derived neurotrophic factor in prefrontal cortex and hippocampus, the expression of activity-regulated cytoskeleton-associated protein in the prefrontal cortex, and attenuating stress-induced glutamate release in prefrontal/frontal cortex, all of which improve neural plasticity and resilience. In agreement with these notions, prolonged administration of agomelatine increases neurogenesis within the hippocampus. These unique actions of agomelatine are suggested to be a result of synergistic action on MT1/MT2 and 5-HT2c receptors (Racagni et al. 2011).
Considering the above characteristics of agomelatine and pathophysiology of the disease, including reduced volume of neural tissue, especially in the right frontal and parietal cortices and hypofunctioning of catecholaminergic circuits especially those associated with prefrontal cortex, may explain our study finding of agomelatine being comparatively effective as MPH for ADHD treatment to some extent (Curatolo et al. 2009; Purper-Ouakil et al. 2011). Recently available evidence suggests that circadian rhythm disruptions can at least modify severity and outcome of ADHD. Circadian rhythm may affect ADHD symptomatology, indicating an intrinsic link between the circadian and psychiatric conditions (Coogan and Thome 2011; Imeraj et al. 2012; Snitselaar et al. 2014). It is possible that agomelatine may improve the ADHD symptoms by improving circadian rhythm disturbances as well. An interesting finding, which empowers this possibility, is a decrease in nocturnal 6-sulfatoxymelatonin (6-S-aMT) excretion after administration of prolonged release methylphenidate (PRMPH) by Molina-Carballo et al. Excretion of 6-S-aMT was found to be significantly larger in patients with ADHD in the mentioned study. In the same study, PRMPH changed the morning and evening melatonin concentrations in patients with ADHD. These findings of Molina-Carballo et al. (2013) suggest that even the current standard treatment and commonly used stimulants may have an effect on circadian rhythm by regulating melatonin levels as well. ADHD is one of the most prevalent chronic childhood disorders, which often coexists with other psychiatric comorbidities. In some cases, families are not willing to consider stimulants especially since concerns have been expressed about upsurge in prescription of stimulants and engagement of a subgroup of young people in abuse and/or diversion of their prescription in the school. Moreover, in some cases, side effects of the current medication may worsen some comorbidities of the affected ones. In such instances, nonstimulant medications are capturing attention (Mohammadi and Akhondzadeh 2007, 2010; Cormier 2008; Kahbazi et al. 2009).
The limitations of the present study include the small number of participants, the lack of a placebo group, and administration of the ADHD Rating Scale as the only means for measuring outcomes. In addition, since we have administrated methylphenidate with a fixed dose, it is possible that there was still room for more improvement should we have decided to titrate dosage for each individual to achieve maximum effect.
Conclusion
The results of this study must be considered preliminary. This 6-week course of treatment with agomelatine showed favorable safety and efficacy profile in children and adolescents with ADHD. Considering the antidepressant effects of agomelatine, future studies on the effectiveness of agomelatine compared with both MPH and placebo should include a broader spectrum of ADHD patients, including those with comorbid mood and anxiety disorders, sleep problems, and inattentive presentation. Nevertheless, larger controlled studies for longer periods of time with the measurement of sleep and circadian indices, as well as the safety profile of agomelatine compared with MPH, are needed.
Clinical Significance
This is the first randomized and controlled trial evaluating the beneficial effects of agomelatine in children and adolescents with ADHD. Results from this trial indicate that agomelatine is a tolerable and effective therapy in ADHD, in particular as second-line therapy.
Footnotes
Acknowledgments
The funding organization had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript and the decision to submit the article for publication.
Disclosures
The authors do also affirm that there was no source of funding; none of the authors have direct or indirect commercial/financial incentive associating with publishing the article, and no funding agreement limits their ability to complete and publish the study. In addition, the authors do not have any conflicts of interest.