
Abstract
Background:
Pediatric obsessive-compulsive disorder (OCD) is a common, debilitating illness. When childhood OCD symptom onset is described as acute and severe, diagnostic criteria for pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS) and pediatric acute-onset neuropsychiatric syndrome (PANS) should be considered. However, the frequency and differentiating features of these putative syndromes within pediatric OCD remain poorly understood.
Objectives:
To determine the prevalence and characteristics of those meeting PANDAS and/or PANS criteria within pediatric OCD, as determined by parent report and clinician interview.
Methods:
Consecutive youth presenting to a subspecialty pediatric OCD clinic were rigorously assessed through the Anxiety Disorders Interview Schedule for DSM-IV, the Children's Yale–Brown Obsessive-Compulsive Scale, and through self- and parent-report measures, including a medical questionnaire. Strict diagnostic criteria for PANDAS and PANS were applied to determine prevalence rates, and comparative analyses were performed between subgroups.
Results:
Among 136 youth with a lifetime OCD diagnosis, 5% (n = 7; 95% adjusted Wald interval: 1%–10%) met proposed criteria for PANDAS and/or PANS, of whom two met PANDAS criteria, four met PANS criteria, and one met criteria for both. Those in the PANDAS/PANS subgroup were more likely to have autoimmune illness, less likely to report symmetry factor symptoms, and had greater OCD-related family impairment during their worst OCD episode.
Conclusion:
A small yet significant percentage of pediatric OCD outpatients met criteria for PANDAS and/or PANS, justifying routine screening and attention to related characteristics during assessment and management. Longitudinal studies of these putative subtypes are warranted.
Introduction
O
The first description of PANDAS, published in 1998, defined it as the sudden onset of obsessive-compulsive or tic disorder symptoms following a Group A Streptococcus (GAS) infection (Swedo et al. 1998). In a clinic setting, this is observed as a cluster of abrupt onset symptoms following a GAS infection, including a pathogenic flare with severe obsessive compulsions (e.g., shoe licking) and/or tics (e.g., whooping), and concomitant symptoms, including developmental (behavioral) regression, marked separation anxiety, and aggression (Chang et al. 2015; Murphy et al. 2012). Due, in part, to the challenge of determining a temporal association between GAS infection and the onset of OCD and/or tic symptoms, relatively few PANDAS cases have been confirmed through these strict criteria (Gabbay et al. 2008). Thus, the validity of PANDAS as a unique clinical entity has been brought into question, becoming a topic of significant debate and controversy among psychiatrists and neurologists (Murphy et al. 2014).
In an effort to resolve this debate, a new diagnostic syndrome was proposed in 2012. Termed pediatric acute-onset neuropsychiatric syndrome (PANS), this new definition addressed the primary criticism of the PANDAS definition by eliminating the requirement of a preceding GAS infection. Additionally, to account for a broader range of clinical presentations, the new description added a food restriction criterion and the tics criterion was excluded (Swedo et al. 2012) (Table 1).
As proposed in Swedo et al. (1998).
As proposed by Swedo et al. (2012).
Such as sleep disturbances, enuresis, or urinary frequency.
Such as Sydenham chorea, systemic lupus erythematosus, or Tourette's disorder.
OCD, obsessive-compulsive disorder.
It is notable that OCD symptoms are a foundational criterion in the clinical descriptions and diagnostic requirements for both PANDAS and PANS. Yet, to date, the prevalence of PANDAS and PANS has only been studied in pediatric samples comprised primarily of patients with tic (Singer et al. 2000) or movement disorders (Kilbertus et al. 2014). Singer et al. (2000) evaluated 80 pediatric subjects (5–17 years) with a tic disorder diagnosis. Of these, 42 (53%) reported a sudden onset of tics. Only 9 of the 42 cases (11%) were associated with streptococcal infections and none met criteria for PANDAS. PANS had not yet been described at the time of publication.
Kilbertus et al. (2014) assessed 284 children presenting to a movement disorders clinic and identified 39 (14%) with sudden-onset tics and/or OCD. PANDAS diagnosis was based upon the presence of at least one symptom exacerbation following initial assessment, with concurrent evidence of acute Group A beta hemolytic Streptococcus (GABHS) infection. None met the criteria for PANDAS, and only 1% (n = 2/284) met the criteria for PANS. This suggests a relatively low overall prevalence of PANS within the pediatric movement disorder population.
No study has examined the prevalence of children and youth meeting the criteria for PANDAS and PANS within an OCD population (Williams and Swedo 2015). While the etiological factors of PANDAS and PANS remain in debate, determining the frequency of children and youth meeting criteria within the pediatric OCD population (as established by interview and parent report) is important to guide standard clinical assessment.
The characterization of symptoms and broad functioning of youth meeting PANDAS/PANS criteria is also necessary to guide best management practices. Only a small number of studies have been published to describe the diagnostic and nondiagnostic presentation, history, and functioning characteristics of patients diagnosed with PANDAS and PANS. In 2010, Bernstein et al. reported that in comparison with those with a classic OCD (COCD) presentation (n = 18), those meeting PANDAS criteria (n = 21) displayed increased urinary urgency, inattention, hyperactivity, impulsivity, deterioration in handwriting, and school performance decline. All these characteristics were captured in the subsequently defined PANS diagnostic criteria.
More recently, the characteristics of two PANS samples have been reported. Murphy et al. (2015) identified three distinct symptom clusters within 43 PANS-diagnosed youth: (1) nearly all (93%) displayed four to five of the eight core PANS symptoms (although only two are required for diagnosis); (2) most (92%) reported streptococcal-related symptoms; and (3) half (51%) demonstrated more than one putative cytokine-driven/physiological symptom (e.g., food restriction).
Frankovich et al. (2015) reported on the first 53 youth assessed in a PANS specialty clinic, of whom 19 met full PANS criteria. Of these 19, many experienced GAS infections at symptom onset (21%) and during flares (74%), in addition to reporting a relapsing/remitting course (84%). Additionally, the PANS patients reported prominent sleep disturbances (84%), urinary issues (58%), sensory amplification (66%), and generalized pain (68%).
A nondiagnostic characteristic that has not been well studied in pediatric OCD and its putative subtypes is the impact of illness on the family (Vikas et al. 2011). Family functioning deficits in pediatric OCD have been associated with increased severity in COCD cases [for review, see Murphy and Flessner (2015)], and this relationship may also exist in PANDAS/PANS cases. Important from a clinical perspective, the centrality of family factors has been increasingly recognized in the management of OCD symptoms (Freeman et al. 2003; Merlo et al. 2009).
The primary aim of this study was to assess the prevalence of those meeting PANDAS and PANS criteria in a pediatric OCD outpatient sample. The secondary aim was to shed light on these putative pediatric OCD subtypes by detailing diagnostic and nondiagnostic features of the PANDAS/PANS cases, including medical and psychiatric history, family functioning characteristics, and OCD symptom factors.
Methods
All study protocols were approved by the University of British Columbia ethics board. Patients and their caregiver(s) were fully informed of all aspects of the study before they gave their written assent and consent to take part in this research project.
Assessments
Consecutive, physician-referred patient assessments were conducted at the University of British Columbia Provincial OCD Program (UBC-POP) between October 2011 and June 2015. Each new OCD patient within our program was assessed for the presence or absence of PANDAS and PANS criteria. OCD diagnosis was rigorously established through a clinical psychologist-administered structured interview and confirmed by a child and adolescent psychiatrist.
Baseline assessments were conducted with participants and at least one caregiver in attendance, with an opportunity for separate interviews when desired or appropriate. When clinician measures were not completed, the relevant information was extracted from patient charts if available. Full assessment also included completion of online parent- and child-report questionnaires before the interview date, which are described in detail below. Parent- and child-report measures were completed through research electronic data capture (REDCap; Vanderbilt University, Nashville, TN), an online software tool for collecting and storing clinical and translational data (Harris et al. 2009). Measures collected by REDCap included the OCD Family Functioning (OFF) Scale (Stewart et al. 2011) and an OCD background and medical questionnaire.
Study measures and instruments
The Anxiety Disorders Interview Schedule for DSM-IV (ADIS-IV) (Silverman and Albano 1996) is a semistructured, validated diagnostic instrument that was modified for this study to assess both current and lifetime psychiatric disorder diagnoses. In addition, questions were added to screen for obsessive-compulsive-related disorders and to specifically collect data regarding diagnostic criteria for PANS and PANDAS (Swedo et al. 1998, 2012).
The Children's Yale-Brown Obsessive Compulsive Scale (CY-BOCS) (Goodman et al. 1989) is a gold standard clinician report measure of pediatric OCD severity, rating 10 items between 0 (no symptoms) and 4 (extreme symptoms). Standard CY-BOCS cutoff scores were used to define five severity levels: subclinical (0–7), mild (8–15), moderate (16–23), severe (24–31), and extreme (32–40). The CY-BOCS checklist established the presence of symptoms within four OCD symptom dimensions or factors as follows: forbidden thoughts (i.e., aggressive, religious, and sexual obsession categories), symmetry (i.e., symmetry obsessions, checking, counting, ordering, and repeating compulsion categories), cleaning (i.e., contamination, somatic obsessions, and cleaning compulsion categories), and hoarding (i.e., hoarding obsession/compulsion categories) (Bloch et al. 2008). Participants reporting at least one lifetime symptom within a symptom category were assigned a score of 1 for that category; otherwise, a score of 0 was assigned. Total symptom factor scores were determined by summing all relevant category scores, and as such, the range for the forbidden thoughts factor was 0–3, the range for the symmetry factor was 0–5, the range for the cleaning factor was 0–3, and the range for the hoarding factor was 0–2.
The OFF scale (Stewart et al. 2011) is a three-part, validated self-report measure completed by both parents and OCD-affected youth. Part 1 comprises 21 items, reporting frequency of OCD-related interference with respect to daily family activities, social life, work/school performance, and emotions among family members (0 = never, 1 = little, 2 = often, 3 = daily; total score range 0–63) at current and worst-ever OCD severity time points. Part 2 measures frequency at which specific OCD symptoms interfere with family functioning. Part 3 measures the impact of OCD on family role functioning. For purposes of this study, part 1 items at worst-ever OCD severity were selected as the most pertinent measure of OCD impact on family function. As one or both parents completed the OFF scale, a combined mean score derived from all sources was used for each participant during analyses.
Additional data were collected using a background and medical questionnaire and included questions about age at OCD onset, age at initial assessment, gender, ethnicity, birth complications, and developmental history. Information was also collected regarding individual medical and psychiatric histories. This included history of streptococcal infections, other infections (e.g., ear, skin, tooth infection, pneumonia), endocrine disorders (e.g., growth delay/short stature, late-onset puberty), blood disorders (e.g., anemia), urinary and bowel incontinence, meningitis, multiple sclerosis, rheumatoid arthritis, Crohn's disease, eczema/psoriasis, autoimmune disease, allergy, chronic hives, asthma/or lung problems, anxiety, OCD, ADHD, and tic disorders.
For the purpose of categorizing youth into PANDAS/PANS and COCD subgroups, two approaches were used to capture data about the presence of related symptoms at illness onset (Table 1). First, parents independently reported on whether or not PANS and PANDAS diagnostic criteria were present at the time of illness onset through an online REDCap link. Second, clinical psychologists administered the semistructured ADIS diagnostic interview with extension questions to inquire about the presence of these criteria.
Eligibility
Patients were eligible if they met all criteria for a lifetime Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) (American Psychiatric Association 1994) OCD diagnosis, gave their assent, and had the consent of at least one caregiver to participate in the study. In total, 136 participants were recruited, who were 54% male, and ranged between 6 and 19 years old.
Data analyses
Data analyses were conducted through SPSS (version 22) (IBM Corporation 2013). The proportion of PANDAS/PANS cases discovered was reported using a point estimate and the 95% adjusted Wald interval as the number was small (Agresti and Coull 1998). To compare diagnostic and nondiagnostic presentations, categorical data were analyzed using Fisher's exact test. Continuous data were analyzed using two-tailed independent sample t-tests, which provide appropriate type I error rates for small groups. For all analyses, the statistical threshold was set at α = 0.05. As the inferential analyses were exploratory in nature, Bonferroni correction for multiple comparisons was not applied. In all instances, the valid percent was reported if data were missing.
Results
Among 136 participants diagnosed with lifetime presence of pediatric OCD, two met criteria for PANDAS (1%), four met criteria for PANS (3%), and one met criteria for both PANDAS and PANS (1%) (Table 2). As such, 5% (95% adjusted Wald interval: 1%–10%) of the cases in this pediatric OCD outpatient sample met PANDAS and/or PANS criteria (Fig. 1).
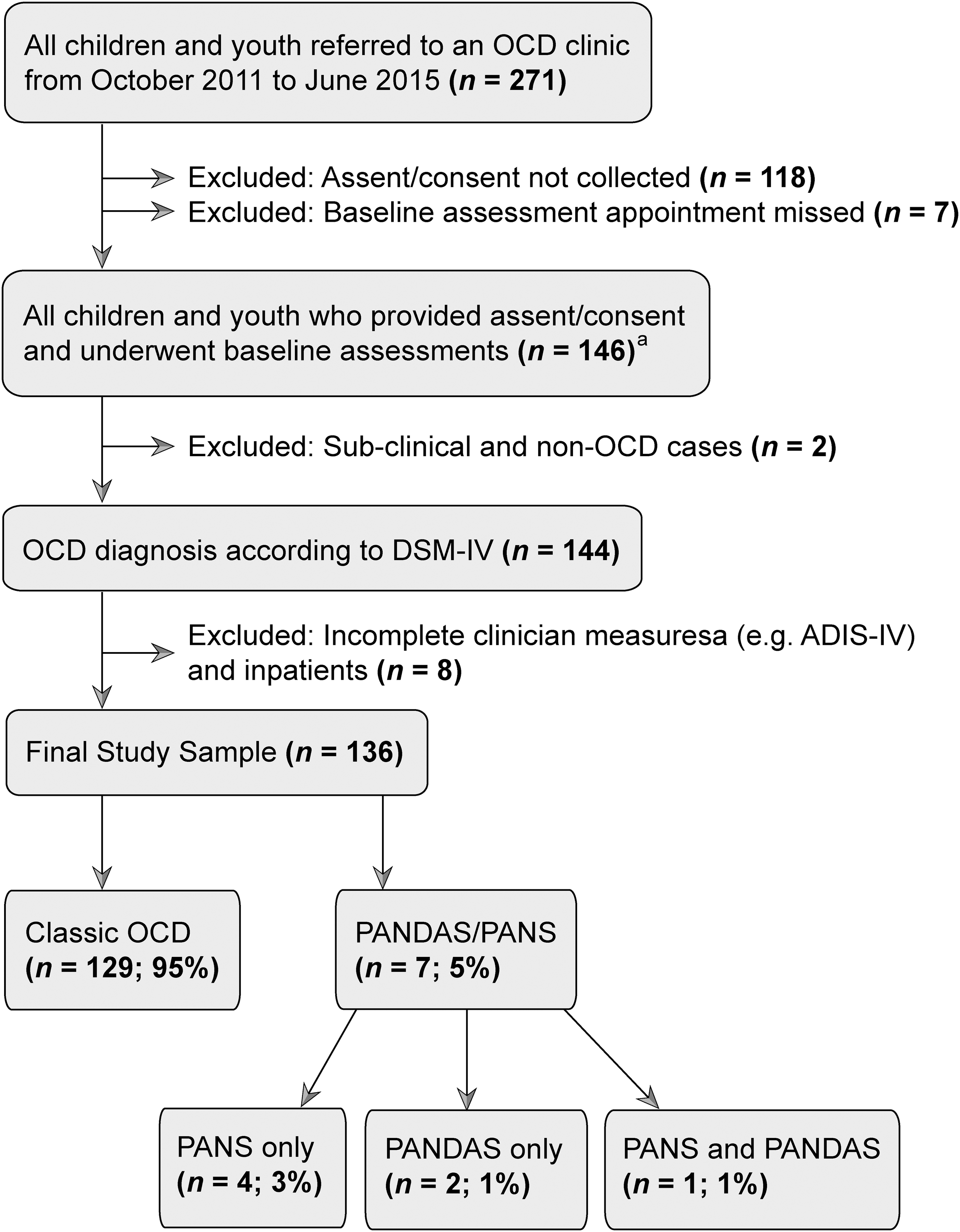
Sampling methodology used to determine prevalence of PANDAS and PANS in a pediatric OCD outpatient clinic. aFor participants with incomplete clinician measures, relevant information from patient charts was extracted when available. OCD, obsessive-compulsive disorder; ADIS-IV, Anxiety Disorders Interview Schedule for DSM-IV; PANDAS, pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections; PANS, pediatric acute-onset neuropsychiatric syndrome.
Based upon parent report and clinical interview at assessment.
Parents noted puberty onset was late.
This denotes the reported presence of emotional state rather than a clinical diagnosis of an anxiety or depressive disorder.
ADHD medications also taken (methylphenidate and atomoxetine).
ADHD medications also taken (clonidine).
ADHD, attention-deficit/hyperactivity disorder; GAS, Group A Streptococcus; OCD, obsessive-compulsive disorder; PANDAS, pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections; PANS, pediatric acute-onset neuropsychiatric syndrome; P1, PANDAS/PANS patient 1, etc.; SSRI, selective serotonin reuptake inhibitor.
Demographics and medical histories
All of those meeting PANDAS and PANS criteria self-identified as white, whereas the overall sample was reportedly more diverse (71% white, 18% Asian, 11% other). The percentage of boys in the PANDAS/PANS subgroup (71%; n = 5/7 valid responses) did not differ significantly from that in the COCD subgroup (53%; n = 68/128 valid responses; p = 0.452).
At initial symptom onset, PANDAS/PANS participants were approximately the same age (9.3 years old, SD = 5.2) as the COCD participants (9.4 years old, SD = 2.7) (p = 0.953). At the time of assessment, the PANDAS/PANS subgroup (11.4 years, SD = 4.1) was on average 2 years younger than the COCD subgroup (13.1 years, SD = 2.7; p = 0.131). As such, the PANDAS/PANS youth were assessed 2 years earlier in the course of their illness compared with the COCD patients (OCD duration: 2.0 years vs. 3.9 years; p = 0.053) (Table 3).
Measured by the clinician-rated CY-BOCS (scored of 40) at baseline assessment.
OCD-related family impairment at worst OCD severity (OFF Scale-Part 1 score of 63).
Based on lifetime history as assessed by the ADIS interview, as opposed to indicating subthreshold symptoms presenting at OCD onset (reported in Table 2).
Mood disorders, including major depressive disorder and dysthymia.
Anxiety disorders, including panic disorder, agoraphobia, separation anxiety disorder, and social phobia.
Tic disorders, including Tourette's disorder, chronic motor/vocal tic disorder, and transient tic disorder.
ADHD, attention-deficit/hyperactivity disorder; ADIS, anxiety disorders interview schedule; CY-BOCS, Children's Yale-Brown Obsessive Compulsive Scale; COCD, classic obsessive-compulsive disorder; OFF, OCD Family Functioning.
At assessment, 29% (n = 2) of those in the PANDAS/PANS subgroup reported taking both a selective serotonin reuptake inhibitor (SSRI) (i.e., fluoxetine) and an atypical antipsychotic (i.e., risperidone) medication to manage OCD symptoms. The others in the PANDAS/PANS subgroup reported taking antibiotics, ibuprofen, omega-3 fatty acids, probiotics, or no medications/supplements (Table 2). Among the COCD patients, 45% (n = 13/29 valid responses) reported taking an SSRI (p = 1.00) and 7% (n = 2/29 valid responses) reported taking an atypical antipsychotic (p = 0.062) to manage OCD symptoms. Seven percent of COCD participants reported taking omega-3 fatty acids (n = 2/27 valid responses), but none reported using antibiotics, ibuprofen, or probiotics to manage their OCD symptoms.
Regarding medical histories, all but one of those in the PANDAS/PANS subgroup (n = 6/7) endorsed a lifetime history of streptococcal infection, in contrast to the COCD subgroup where a history of GAS infection was reported in less than half of the cases (n = 47%; 41/87 valid responses) (p = 0.020) (Table 4). In contrast, regarding other reported infections, there was no statistical difference between the proportion of those reporting a history of skin infections (e.g., staphylococcus) in PANDAS/PANS (43%; n = 3/7) and COCD (46%; n = 41/89 valid responses) subgroups (p = 1.000). Parents of PANDAS/PANS participants (57%; n = 4/7) were significantly more likely than parents of COCD participants (18%; n = 17/92 valid responses) to report a history of urinary incontinence for their child (p = 0.035).
Based on Fisher's exact test between PANDAS/PANS and COCD subgroups.
No one reported rheumatic fever history.
Parent report of OCD symptoms beginning or worsening with the onset of this health issue.
No one reported lupus or immunodeficiency. One COCD case had multiple sclerosis (<1% of total sample) and one had rheumatoid arthritis (<1% of total sample).
Immune-related illnesses reported by Murphy et al. (2015).
Once COCD patient reported an autoimmune history and also reported a history of eczema/psoriasis.
COCD, classic obsessive-compulsive disorder; PANDAS, pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections; PANS, pediatric acute-onset neuropsychiatric syndrome; P1, PANDAS/PANS patient 1, etc.
Based upon the parent-reported medical questionnaire, 29% (n = 2/7) of the PANDAS/PANS subgroup and one percent (n = 1/99 valid responses) of the COCD subgroup had a lifetime presence of an autoimmune disease (p = 0.011) (Table 3). In addition, for five (71%) of those within the PANDAS/PANS subgroup, parents reported a history of at least one of the following diseases with putative autoimmune and inflammatory etiologies: allergies, asthma, chronic hives, or eczema/psoriasis. However, the presence of at least one of these illnesses did not statistically differ from the COCD group (52%; 49/94 valid responses) (p = 0.445).
OCD characteristics and psychiatric history
Those meeting proposed diagnostic criteria for PANDAS/PANS did not have clinician-assessed differences in OCD severity at assessment, but did report increased OCD-related family impairment at the time of worst OCD severity (mean OFF score Part 1 = 41.4, SD = 7.2) compared with the COCD subgroup (mean OFF score Part 1 = 31.7, SD = 11.5) (p = 0.031) (Table 4). CY-BOCS checklist data allowed examination of OCD symptom dimensions for each subgroup (Bloch et al. 2008). Respondents meeting PANDAS/PANS criteria were approximately two times less likely to report current symmetry factor symptoms (mean factor score = 1.3 of 5) indicating fewer symmetry, ordering, counting, checking, and repeating category symptoms compared with the COCD subgroup (mean factor score = 2.8 of 5) (p = 0.014). No other symptom factor significantly delineated groups (Table 4).
The concurrent presence of an anxious (57%), depressed/labile (57%), or irritable (71%) mood during OCD onset was reported for the majority of those in the PANDAS/PANS subgroup (Table 2). However, none of those meeting PANDAS/PANS criteria received a mood or anxiety disorder diagnosis as established through the ADIS diagnostic interview, and there were no between-group differences in this regard (Table 4). There were also no significant group differences with respect to other comorbidities or reported family psychiatric diagnoses, perinatal, or developmental histories (Supplementary Table S1; Supplementary Data are available online at
Discussion
Prevalence interpretation
To our knowledge, this is the first study to assess prevalence rates of PANDAS and PANS within a pediatric OCD sample. A small yet significant percentage (5%; 95% adjusted Wald interval: 1%–10%) of new cases in our OCD outpatient clinic met PANDAS or PANS threshold criteria as assessed through parent report and clinical interview (Fig. 1). The prevalence and related confidence interval reported here are notably greater than zero, supporting the legitimacy of a PANDAS/PANS subgroup within the pediatric OCD population.
The identified prevalence rate reported in this study is proximal to those from studies of heterogeneous samples recruited from pediatric motor (Kilbertus et al. 2014) and tic disorder (Singer et al. 2000) populations. Kilbertus et al. found that 1% met criteria for PANS. Singer et al. found that although no participant met the full PANDAS criteria, 11% reported abrupt symptom onset. A subgroup within this 11% may have met the less stringent PANS criteria had the information regarding criteria been available at the time.
While the differing base populations and the introduction of the PANS definition may account for cross-study variability, differences in methodologies likely also contributed to reported prevalence rates. Singer et al. relied on self-reports to determine streptococcal infection history. In comparison, Kilbertus et al. used more stringent criteria by identifying potential PANDAS cases presenting with acute symptom onset and following them to determine whether subsequent tic or OCD symptom exacerbations were associated with at least one positive throat culture and a positive ASOT and/or anti-DNAse B test, with decreasing serologic titers during convalescence (Supplementary Table S2).
In the current study, each newly assessed patient within a pediatric OCD outpatient program was prospectively and systematically examined for the presence or absence of PANDAS and PANS criteria. OCD diagnosis was rigorously established through psychologist-administered structured interview and confirmed by a child and adolescent psychiatrist. The lag between initial symptom onset and initial clinical assessment mandated reliance on parent and youth reports for data collection. It also precluded data collection during the exacerbation that would optimally involve physical neurologic examination (to confirm choreiform and neuropsychiatric signs), tanner staging (to confirm prepubertal status), and bacterial cultures (to confirm active GAS infection).
As an unavoidable consequence of this study design, recall bias may have influenced parent descriptions of events related to initial symptom onset. Moreover, subgroup differences may have influenced their potential to access and attend initial outpatient OCD assessments within our program. In contrast to those with an ongoing waxing/waning course (as described for classic OCD), youth with an episodic/relapsing/remitting course (as described for PANDAS/PANS) may have been more likely to experience dramatic symptom improvement or remission by the time of the scheduled initial assessment. In addition, progressive deterioration of the PANDAS/PANS subgroup during wait times (Murphy et al. 2015) may have led to assessments in urgent care clinics and/or inpatient wards, thus bypassing the standard outpatient baseline assessments provided by the study site's OCD program.
The above-noted sequelae of our study design may have influenced prevalence estimates in opposite directions. The fact that diagnostic signs and symptoms related to the initial episode were based on parent report rather than direct observation may have led to overestimates of PANDAS/PANS. In contrast, the notable delay between onset and assessment may have differentially impacted subgroups, with greater cancellation rates and more significant changes in severity in the episodic PANDAS/PANS subgroup, leading to underestimates of prevalence and OCD severity.
A major strength of this study is that it was conducted at the only pediatric OCD subspecialty clinic within a universal healthcare catchment area during the identified study period. This factor significantly improves the generalizability of the study findings to the broader pediatric OCD population. Given the polarization of clinical perspectives regarding PANDAS/PANS, families in countries with private healthcare systems have been known to forgo local healthcare in preference for facilities with expert reputations. As such, it is extremely challenging to accurately determine PANDAS/PANS rates within pediatric OCD in a private healthcare system. In contrast, this study was conducted at a center where families of the OCD-affected youth did not have supported alternative subspecialty treatment options. As such, the influence of families' clinic preference was markedly decreased in this sample compared with American-based studies.
Exploratory comparison of PANDAS/PANS versus classic pediatric OCD subgroups
As a secondary study aim, characteristics of the identified PANDAS/PANS and COCD subgroups were examined. The relatively low prevalence and absolute number of PANDAS/PANS cases in the sample imposed a limitation on the power to conduct comparative analyses. This restricted the ability to identify subtle group differences, indicating that results demonstrating statistically significant differences are worthy of greater confidence than those where differences were not found. While an inferential statistical approach appropriate for small samples was utilized, larger studies are required to generalize findings to the broader population. Subgroups were compared with respect to OCD characteristics, demographics, perinatal, developmental, medical, psychiatric, and family psychiatric history.
OCD-related characteristics
There were two main OCD-related differences identified between subgroups, including family impairment at the time of worst OCD severity, and OCD symptom types. In addition, reported between-group differences in OCD duration and in anxiety disorder history approximated significance. These combined findings suggest that the PANDAS/PANS subgroup is characterized by youth with abrupt-onset illness, a notable change from a baseline with little pathology, more urgent need for assessment, and greater family impact.
A key differentiating characteristic between subgroups was the degree of family impairment at worst OCD severity, which was nearly 25% higher in the subgroup meeting PANDAS/PANS criteria compared with the COCD group. This suggests that PANDAS/PANS cases may have been more severe and disruptive at illness onset and more likely to require urgent care and family respite than COCD patients. While no significant differences were observed for OCD severity at initial clinic assessment, ratings for OCD severity at onset were unfortunately not collected. As noted above, it is possible that PANDAS/PANS patients were more severe at symptom onset, with decreased severity by the time of initial assessment due to episodic course.
The PANDAS/PANS group reported a lower prevalence of symmetry factor-related OCD symptoms (i.e., symmetry obsessions, checking, counting, ordering, and repeating compulsions) than the COCD group (Table 4). These results are consistent, in part, with those reported by Swedo et al. (1998) in the largest PANDAS cohort to date (n = 50), in which children with PANDAS were less likely to exhibit counting symptoms (4/24; 17%) than symptoms related to other factors (e.g., contamination, 16/24; 67%). The results are not consistent, however, with other studies in which no significant differences in symptom factors were identified (Bernstein et al. 2010).
While age of onset was similar across subgroups (p = 0.953), those with PANDAS/PANS had a shorter OCD duration at the time of initial assessment, a finding that approached statistical significance (p = 0.053). The first result is in keeping with research conducted by Bernstein et al. (2010) who reported that the PANDAS/PANS average age of onset (7.27 years, SD = 2.61) was not significantly different from the age of onset of the classic pediatric OCD patients (8.65, SD = 3.35). However, it is notable that the current study and the Bernstein study reported earlier PANDAS/PANS onset ages than the onset reported in the literature for classic pediatric OCD (10.3 years, SD = 2.5) (Geller and March 2012). In contrast to the current study and the Bernstein study, other groups specializing in PANDAS and PANS have found a significant age difference, reporting that PANDAS/PANS onset often occurs 2–4 years before the onset of COCD (Murphy et al. 2015).
In regard to the second result that those with PANDAS/PANS had a shorter OCD duration at the time of initial assessment, it may be clinically relevant that PANDAS/PANS youth were assessed 2 years earlier in the course of their illness compared with the COCD patients (OCD duration: 2.0 years vs. 3.9 years). One potential explanation for this result is that the parents of children with acute and severe OCD symptoms may have advocated more forcefully for their children to be assessed in a specialty clinic.
Non-OCD-related characteristics
Parents in the PANDAS/PANS subgroup reported increased lifetime prevalence of streptococcal infections (p = 0.012), urinary incontinence (p = 0.03), and autoimmune illness (p = 0.011) compared with those in the COCD subgroup. Given their presence within diagnostic criteria, it is unsurprising that the streptococcal infections and urinary symptoms were more common in PANDAS/PANS cases. However, the increased reported presence of autoimmune illness in these cases is informative.
While the causative mechanisms underlying PANDAS and PANS remain under debate, a dominant hypothesis is that an infection triggers an immune response causing deleterious effects on the brain, particularly the basal ganglia, frontal cortex, and thalamus (Williams and Swedo 2015). This hypothesis has some support from epidemiological (Mell et al. 2005) and animal studies (Brimberg et al. 2012) and as such, the PANDAS/PANS population may be expected to exhibit a high prevalence of comorbid autoimmune disease (Geller and March 2012). PANDAS/PANS respondents in this study were more likely than COCD respondents to endorse a history of autoimmune disease. This finding is consistent with the elevated prevalence of family autoimmune/inflammatory disease in PANS (71% Frankovich et al. 2015) and of maternal autoimmune disease in likely PANDAS versus unlikely PANDAS cases (Murphy et al. 2010). It is also consistent with a recent large electronic health record study in which a significantly increased odds ratio of IgA deficiency was identified between pediatric OCD versus ADHD, autism spectrum disorders, and anxiety disorder patients (Kyle Williams, personal communication, October 3, 2016). This is relevant given that IgA deficiency predisposes to autoimmunity and is the immune deficiency most commonly comorbid with autoimmune disorders.
A caveat to the autoimmune finding reported here is that PANDAS/PANS participants were not more likely to endorse items for diseases with likely autoimmune etiologies, such as those reported by Murphy et al. (2015) (e.g., asthma, allergies, thyroiditis, and psoriasis) (Table 3). It is very likely, given the relatively low population base rates of these disorders, sufficient power may not have been present to detect differences for these individual autoimmune-linked diseases. This finding is consistent with a previous study reporting on 77 youth with PANDAS (2.0–14.5 years), who were no more likely to report individual autoimmune disorders than controls (hypothyroidism: 4% vs. 4%; autoimmune thyroiditis: 2% vs. 1%; celiac disease: 1% vs. 0.1%) and who did not test positive for autoantibodies more often than controls (Stagi et al. 2014). To better illuminate the possible PANDAS/PANS-autoimmune relationship, future studies should attempt to report on a standard set of autoimmune/inflammatory disorders, perhaps based on the clinical evaluation guidelines suggested by the PANS consensus conference (Chang et al. 2015). Additionally, future studies would benefit from much larger samples and pooled data across sites.
With respect to other potential etiologic factors contributing to OCD vulnerability, no environmental risk factors have been convincingly associated with OCD to date (Brander et al. 2016), and no environmental factors were associated with PANDAS/PANS in this sample. It is notable that birth complications were not reported in the PANDAS/PANS subgroup. This is in contrast to COCD where perinatal complications have been associated with OCD in later life (Vasconcelos et al. 2007). One could speculate that the processes underlying PANDAS/PANS represent but one pathway to emergence of the OCD phenotype. Genetic risk may be another important pathway. While headway has been made in confirming the pleiotropic effects of variants that contribute shared risk to psychiatric disorders, including OCD (Gatt et al. 2015) (Cross Disorder Group of the Psychiatric Genomics Consortium 2013), no genetic data were collected in this study.
Conclusion
The present findings indicate that PANDAS/PANS cases represent a legitimate subgroup within pediatric OCD, occurring in at least 1 of 20 assessments. Exploratory analyses suggest that this subgroup is characterized by significant family impact that drives earlier referral for assessment. Autoimmune issues were related to PANDAS/PANS status, but should be further explored using a standard set of identified diseases and larger sample sizes. Finally, future studies should include OCD inpatient populations, those exhibiting acute-onset food restriction, and comparison with community samples to fully understand the prevalence and characteristics of PANS and PANDAS across populations.
Clinical Significance
Screening for PANDAS/PANS should be included as a standard part of pediatric OCD assessment. This is particularly warranted in cases where an abrupt onset is described. Management strategies should include strategies that mitigate the significant impact of OCD symptoms on the family functioning of patients with PANDAS/PANS.
Footnotes
Acknowledgments
The authors would like to thank Laura Belschner and Sarah Yao Lin for their help with data management and Rachel Ho for data entry. Additionally, they are grateful to Boris Kuzeljevic for guidance on the statistical analyses.
Disclosures
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.