
Abstract
Objective:
Irritability (aggression, self-injury, and severe tantrums) associated with autism spectrum disorder (ASD) is often treated with second-generation antipsychotics (SGAs), which are well known for their associated risk of weight gain in youth. Recent reports suggest that youth with ASD treated with SGAs may suffer more pronounced weight gain than typically developing children. In this study, we present a comprehensive comparison of weight gain effects of five SGAs in a clinical population of youth with ASD.
Methods:
We completed a subanalysis of demographic and treatment data describing 202 youth with ASD treated at two large, subspecialty psychiatry clinics. Included subjects were between 2 and 20 years of age and were treated with one of five SGAs (risperidone, aripiprazole, olanzapine, quetiapine, or ziprasidone) for up to 4 years. We calculated change in each participant's body–mass index (BMI) z-score during the treatment period using a linear model where the dependent variable was change in BMI z-score and the independent variables were SGA used and duration of treatment. First, these models were run for each drug separately, then the SGA groups were run together to estimate differences between groups. We also adjusted these models for weight gain-attenuating concomitant medications.
Results:
Treatment with risperidone, aripiprazole, and olanzapine resulted in statistically significant increase in BMI z-score (p = 0.03, 0.05, and <0.01 respectively). Ziprasidone and quetiapine were not associated with an increase in BMI z-score in this analysis (p = 0.47 and p = 0.11). Subjects treated with olanzapine showed a statistically significant greater increase in BMI z-score when compared with the other SGAs (all p-values <0.05). These results did not change when adjusted for multiple testing or weight gain-attenuating medication as covariate.
Conclusion:
Clinicians treating youth with ASD may be able to use this information to balance the risks and benefits of SGA treatment when managing ASD-associated irritability.
Introduction
A
SGAs are highly associated with risk of weight gain and subsequent health concerns such as changes in glucose and lipid metabolism as well as poor cardiovascular outcomes (Maayan and Correll 2011; Galling et al. 2016). Furthermore, evidence suggests that youth with ASD may be at particular risk of weight gain, further increasing the risk of using SGAs to treat ASD-associated behavioral symptoms (Maayan and Correll 2011). Of additional concern, risperidone is known to cause elevated prolactin levels, with the potential to cause gynecomastia and galactorrhea, and olanzapine may directly stimulate pancreatic insulin secretion, may increase blood leptin levels, and has been found to increase blood lipid levels (Kleinberg et al. 1999; Melkersson and Dahl 2004). Despite these known risks, to date, there has not been a head-to-head comparison of SGA weight gain effects in ASD, although weight gain has been consistently demonstrated in SGA research in this population (Aman et al. 2005; Wink et al. 2014). As youth with ASD are at high risk of obesity and its complications, information describing the specific risks associated with individual SGAs is vital to clinicians and caregivers (Curtin et al. 2014).
In this article, we present the first comprehensive comparison of weight gain associated with five commonly used SGAs through a review of naturalistic ASD treatment data. Based on previous pediatric research and work done by our group, we hypothesized that olanzapine would be associated with the largest weight gain and that ziprasidone would cause the least amount of weight gain in our population (Correll et al. 2009; Dominick et al. 2015).
Methods
As part of a larger comprehensive assessment of medication management in ASD, we analyzed chart review data describing individuals with ASD treated at two large subspecialty clinics: the Christian Sarkine Autism Treatment Center (CSATC) and Cincinnati Children's Hospital Medical Center (CCHMC). From our ASD medication management RedCap database (CSATC) and from CCHMC electronic medical records, we identified individuals with ASD between the ages of 2 and 20 years who were treated by our investigators (L.K.W., E.V.P., and C.A.E.) between July 2004 and December 2014, who had at least 2 body–mass index (BMI) scores reported, and who were treated with risperidone, aripiprazole, olanzapine, quetiapine, or ziprasidone for a maximum of 4 years. The included age range of participants was chosen based on Centers for Disease Control growth charts (
At baseline, we compared demographic data between pairs of drug groups using Fisher's exact test for categorical variables and the Wilcoxon rank-sum test for continuous variables. We then calculated the change in BMI z-scores over the treatment period using a robust linear model where the dependent variable was change in BMI z-score and the independent variables were SGA group (five levels) and the duration of treatment. A robust model was used to account for outliers in the data as robust methods are reasonably efficient when the data follow a normal distribution, but unlike traditional methods, they are also resistant to the effect of outliers (Hoaglin et al. 1983). These models first were run for each drug separately, adjusting for duration to determine if there was significant change in BMI z-score between treatment periods. Then, all SGAs were run together in the same model to estimate differences between treatment groups in change in BMI z-score. This resulted in 10 pairwise comparisons between the 5 SGAs. Finally, as some participants were concomitantly treated with medications that can attenuate weight gain [metformin, topiramate, psychostimulants (Klein et al. 2006; Faraone et al. 2008; Fiedorowicz et al. 2012)], we analyzed the above robust linear model with and without adjustment of the use of a weight gain-attenuating medication (a dichotomous variable where either a weight-attenuating medication was used at the beginning or end of the treatment period, or never). To address concerns of type I error due to multiple tests, we utilized the false discovery rate (FDR) so that the overall familywise error rate was 0.05 (Benjamini and Hochberg 1995). All statistical analyses were conducted using SAS® version 9.3 (SAS Institute, Inc., Cary, NC). This project was approved by both applicable Institutional Review Boards.
Results
Two hundred and two individuals with ASD met inclusion criteria for this project. Participants ranged from 2.92 to 19.45 years of age (10.28, standard deviation [SD] 4.04), were predominantly male (83.17%), white (76.24%), diagnosed with having autistic disorder (57.92%), and many were diagnosed with ID (50.78%). Nine participants were also diagnosed with having Fragile X syndrome and one participant had Angelman syndrome. The mean BMI z-score of participants at baseline was 0.88 (SD 1.30), and the mean duration of treatment was 1.22 years (SD 0.97). Demographic data organized by SGA treatment group are reported in Table 1. Table 2 describes concomitant medications prescribed at baseline and final visit within the defined treatment window, also organized by SGA treatment group.
Autistic disorder versus Asperger's disorder and pervasive developmental disorder not otherwise specified combined.
BMI, body–mass index; ID, intellectual disability; n, number; SD, standard deviation.
Weight gain-attenuating mediations are in italic.
Number of participants treated with class of medication when initiated treatment with SGA during the treatment period.
Number of participants treated with class of medication when finished treatment with SGA during the treatment period.
Antiepileptic drug other than topiramate.
AED, antiepileptic drug; alpha-2, alpha-2-antagonist; benzo, benzodiazepine; SGSs, second-generation antipsychotics; SNRI, serotonin norepinephrine reuptake inhibitor.
At baseline, statistical analysis using Fisher's exact and Wilcoxon rank-sum tests revealed notable differences between SGA treatment groups, although gender and race did not differ statistically across the five groups (ps > 0.05). Ziprasidone was prescribed to an older age group compared with both risperidone and aripiprazole (ps < 0.01). Risperidone was prescribed to a younger age group than both olanzapine and quetiapine (p = 0.04 and p = 0.01, respectively). The ziprasidone group had a higher BMI z-score at baseline than aripiprazole, risperidone, and olanzapine (ps < 0.01). The olanzapine group had the smallest number of participants of the five groups and lower baseline mean BMI z-score compared with aripiprazole and quetiapine (p = 0.02 and p < 0.01, respectively). The olanzapine group also had the greatest percentage of subjects with diagnoses of having both autistic disorder and ID. There was no statistically significant difference in duration of treatment between groups (ps > 0.05).
Individual robust models for each drug revealed that individuals treated with risperidone, aripiprazole, and olanzapine had statistically significant increases in BMI z-score during the treatment period (Fig. 1 and Table 3, p = 0.03, 0.05, <0.01, respectively). Individuals treated with quetiapine and ziprasidone did not have statistically significant increases in BMI z-score in this analysis (p = 0.47 and p = 0.11). Subjects treated with olanzapine had the greatest increase in BMI z-score with treatment (+0.96, standard error = 0.36). The robust model that directly compared treatment groups found that olanzapine was associated with significantly more weight gain than the other four SGAs (Table 4, all ps < 0.05). All other comparisons between SGAs were not statistically significant, although a trend toward aripiprazole being associated with more weight gain than ziprasidone and quetiapine was noted (both ps = 0.08). When we controlled for multiple comparisons, all previously significant p-values remained statistically significant. When results were adjusted for concomitant use of weight gain-attenuating medications as a covariate, minor changes in p-values occurred, but when adjusted for multiple testing, the statistically significant results remained (Table 5).
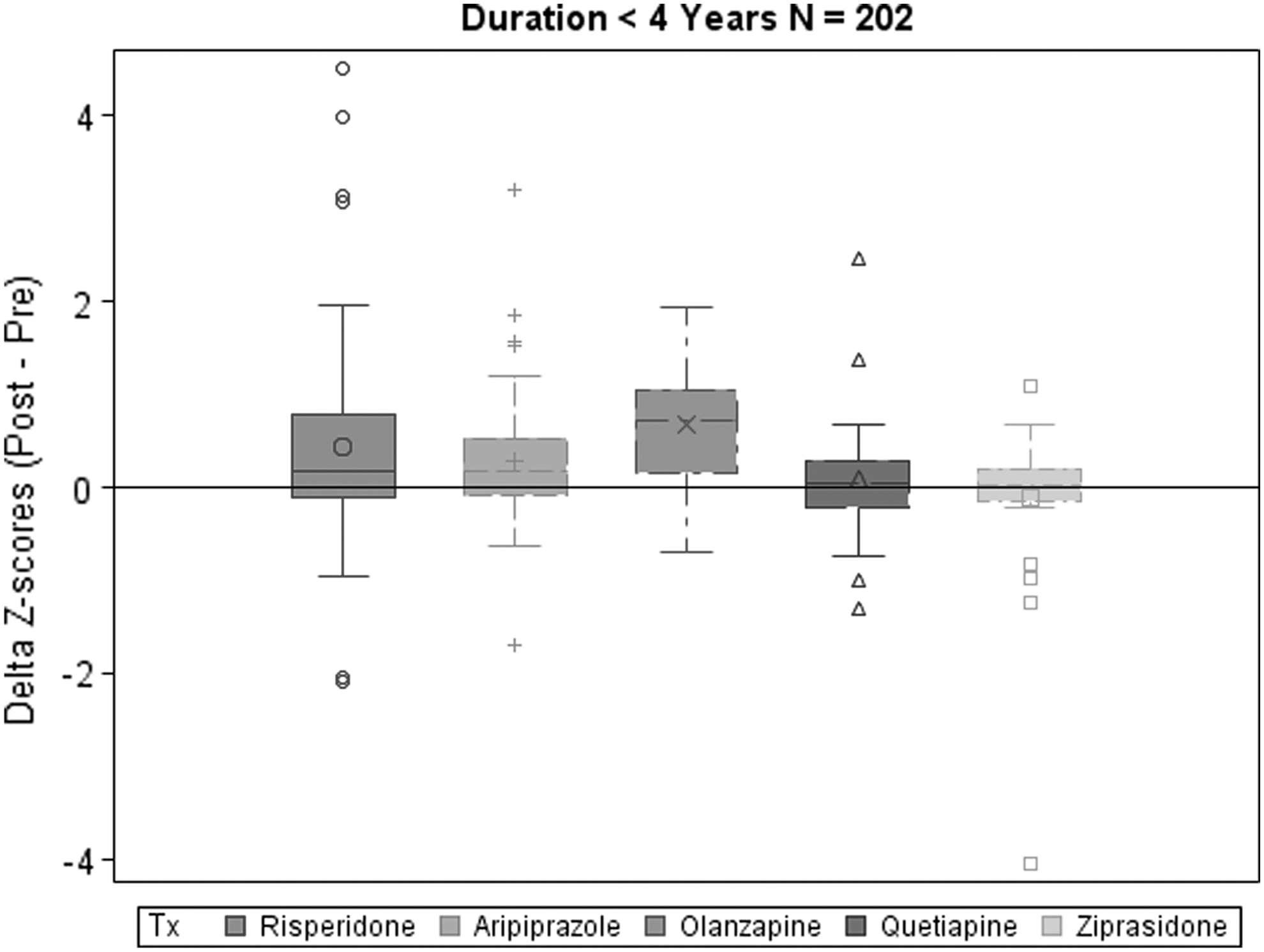
Change in BMI z-score with second-generation antipsychotic treatment. BMI, body–mass index; n, number; Delta z-score, change in BMI z-score; Tx, treatment.
Bold values are statistically significant.
Robust regression model.
0.0496 rounded up to 0.05.
BMI, body–mass index; CI, confidence interval; FDR, false discovery rate.
Bold values are statistically significant.
Italic values are borderline significant.
Robust regression model, p-values adjusted for multiple testing.
BMI, body–mass index; CI, confidence interval; FDR, false discovery rate; A, aripiprazole; O, olanzapine; Q, quetiapine; R, risperidone; Z, ziprasidone.
Bold values are statistically significant.
Italic values are borderline significant.
p-Value is changed to be statistically significant after adjusting for weight gain-attenuating medication use.
BMI, body–mass index; CI, confidence interval; FDR, false discovery rate; A, aripiprazole; O, olanzapine; Q, quetiapine; R, risperidone; Z, ziprasidone.
Discussion
To our knowledge, this is the first head-to-head comparison of weight gain associated with five commonly used SGAs for treatment of disruptive behavior in youth with ASD. As expected, olanzapine was associated with the most significant weight gain among the five SGAs compared. In addition, as expected, ziprasidone was not associated with statistically significant weight gain in this review, although interestingly ziprasidone was not significantly different from the other medications, with the exception of olanzapine. In addition, confirming previous work in this area (Wink 2014), risperidone and aripiprazole were both associated with significant weight gain, but did not separate significantly from each other. Interestingly, quetiapine was not associated with significant weight gain in this patient group, despite weight gain noted with this medication in clinical trials (Martin et al. 1999; Findling et al. 2004). Furthermore, this review demonstrated no significant impact of weight gain-attenuating concomitant medications in this study population, although the study is limited by the small numbers of participants prescribed these medications.
The results of this study must be considered in context of its limitations. Most notably, there were important differences between drug treatment groups at baseline. There were notably fewer participants in the olanzapine group, which may have influenced results. Additionally, the risperidone group had the youngest and the ziprasidone group had the oldest mean patient age at baseline. This may reflect the prescribing practice of using the most evidence-based medication as first-line treatment in the youngest individuals and reserving the less evidence-based medications for treatment of older individuals. Furthermore, olanzapine was prescribed to the group with the lowest baseline BMI z-score, suggesting that olanzapine may have been reserved for individuals who were potentially able to tolerate expected weight gain. Furthermore, quetiapine and ziprasidone were both prescribed to older age groups than risperidone, which may have been a factor in the lack of increase in BMI z-score associated with these two drugs, as previous studies have indicated a slower rate of SGA-associated weight gain in older populations (Hellings et al. 2001). Clearly, age and baseline BMI played a significant role in guiding drug choice; however, how these biases impacted the BMI z-score change with treatment in this analysis is unclear.
Additional limitations of this report relate to its retrospective and naturalistic design. We had little ability to control for the impact of SGA dose, duration of treatment, and concomitant medication usage on BMI z-score change. We attempted to minimize the impact of this variability by adjusting our results for duration of treatment and concomitant medications that may have attenuated weight gain. However, we were unable to control for SGA dosage. Additionally, we did not have access to information regarding family dietary and health history, which may have influenced BMI z-score change with treatment. The sample is also biased toward individuals with potentially more severe pathology and previous treatment failures resulting in referral to our tertiary care ASD treatment centers. Furthermore, all treatment groups had baseline above average mean BMI z-scores, which may have also impacted BMI z-score change with treatment.
Conclusion
The goal of this study was to provide information on the weight gain effect of five commonly used SGAs for treatment of ASD-associated irritability. Given the nature of this retrospective chart review study, the results of this study must be considered along with its limitations. However, we believe that this study adds to the growing safety data regarding use of SGAs in ASD and lays the ground work for future controlled head-to-head analysis of SGA treatment in ASD patients. In the meantime, clinicians treating individuals with ASD may be able to use these data to help guide difficult treatment decisions.
Clinical Significance
To our knowledge, this is the first head-to-head comparison of weight gain associated with five commonly used SGAs for treatment of disruptive behavior in youth with ASD. Our results demonstrate that olanzapine was associated with the most significant weight gain among the five SGAs compared, and ziprasidone was not associated with statically significant weight gain in our population. Surprisingly, quetiapine was also not associated with significant weight gain in this patient group. Given the nature of this retrospective chart review study, the results of this study must be considered along with its limitations. However, we feel these data will help guide clinicians as they make difficult treatment decisions.
Footnotes
Acknowledgment
The authors would like to acknowledge the contribution of Ryan Adams, PhD, for assistance with the manuscript and data analysis review.
Authors' Contributions
All authors participated significantly in appropriate portions of the work, including conception and/or design of the study, acquisition and/or analysis of the data, drafting and/or revision of the manuscript, and approval of the final draft. Craig Erickson, MD, takes responsibility for the integrity of the work as a whole, from inception to publication.
Disclosures
Dr. Yoon has no conflicts to report. Dr. Wink's current research is supported by the Simons Research Foundation, Autism Speaks, Riovant Sciences Ltd., and Cures Within Reach. Dr. Wink has served as a past consultant for Otsuka. Dr. Pedapati receives research support from the Cincinnati Children's Hospital Research Foundation. Dr. Horn served as a consultant for inVentiv Health in 2014. Dr. Erickson receives or has received research grant support from the John Merck Fund, Indiana University School of Medicine, CCHMC, Autism Speaks, the United States Department of Defense, the Simons Foundation, the U.S. Centers for Disease Control, the National Fragile X Foundation, The Roche Group, Neuren Pharmaceuticals, the National Institutes of Health, and Riovant Sciences Ltd.