
Abstract
Objective:
The aim of this study was to compare children and adolescents with attention-deficit/hyperactivity disorder (ADHD) to healthy children and adolescents in terms of state and trait empathy and emotion expression recognition skills. The goal was also to determine whether there are changes in emotion recognition and empathy measures in children with ADHD after methylphenidate (MPH) treatment.
Methods:
The research sample consisted of outpatient drug-naive children and adolescents between the age of 8 and 14 years (n = 65) with ADHD according to the Diagnostic and Statistical Manual of Mental Disorders, 4th ed. criteria, and healthy children and adolescents of the same age (n = 61). Scores of the oppositional problems (OPs) and conduct problems (CPs) were obtained to evaluate their impact on children's empathy skills with the Child Behavior Checklist. Self-reported (Bryant Index of Empathy, BEI) and parent-reported (Griffith Empathy Measurement-Parent Rating, GEM-PR) scales were used to evaluate trait empathy. The Empathy Response Task (ERT) was used to evaluate state empathy, and the Diagnostic Analysis of Nonverbal Accuracy-2 (DANVA-2) was used to evaluate facial expression recognition skills. The scales and tests were repeated after 12 weeks of MPH treatment in the ADHD group.
Results:
There were no significant statistical differences in trait empathy skills evaluated by parent-reported and self-reported measures, ERT, and DANVA-2 scores. In self-reported measures, the girls had higher scores than boys. From the results of the regression analysis, it was concluded that OPs were not associated with the measures. However, CPs were associated with the scores of the BEI, GEM-PR, and the match scores of the ERT. The average dosage of MPH in the group with ADHD was 0.83 ± 0.21 mg/(kg·d). While there was no change in the BEI and GEM-PR scores after 12 weeks of treatment, there was a significant increase in the ERT interpretation subscore and a significant decrease in the recognition error of anger and sadness expressions in the DANVA-2.
Conclusions:
The findings of our study suggest that children with ADHD have similar levels of trait and state empathy skills and facial expressions as healthy controls and CPs negatively affect their empathy skills. MPH treatment does not change trait empathy skills, yet there are some improvements in state empathy skills.
Introduction
I
Empathy as a basis of social interaction occurs with the help of facial expression recognition ability. Empathy also helps to quickly recognize the emotion from a short-term stimulus (Clark et al. 2008). Children with predominantly hyperactive impulsive-type ADHD make significantly more errors in facial expression recognition than healthy children (Milch-Reich et al. 1999).
Some studies have reported that inattentiveness and destructive and maladaptive behaviors may be treated, but that there is no change in positive social behavior and peer conditions in children with ADHD by pharmacological treatment modalities (Whalen and Henker 1991; Whalen et al. 1989). It has been suggested that methylphenidate (MPH) treatment may provide an improvement in emotion recognition by regulating neural activity in a review of studies over the last decade (Hermens et al. 2006).
The effects of pharmacological treatment by MPH or nonpharmacological psychotherapies on social cognition and empathy in children with ADHD have not been explored yet (Uekermann et al. 2010).
By taking the hypothesis that children with ADHD have less facial expression recognition and fewer state and trait empathy skills, this study aims to investigate whether there is a change in facial expression recognition and empathy measures in children with ADHD who receive MPH treatment.
Methods
This randomized and prospective study was carried out after obtaining approval from the Ethics Committee of Marmara University (September 2011/0095). Cases between the ages of 8 and 14 (n = 120) were included into this study who applied to the Child and Adolescent Psychiatry outpatient clinic at Marmara University Training and Research Hospital for the first time from December 2010 to March 2011. The children never had pharmacological treatment for ADHD. Before the cases and healthy volunteers were included in the study, consent forms were signed by their parents and teachers. Socioeconomic status was calculated on the basis of parents' education and income levels (Sasser et al. 2016). All tests were administered individually in a quiet room.
Study design
To diagnose ADHD both accurately and consistently, Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV-based diagnostic measures (American Psychiatric Association 1994) were administered using the Kiddie-Sads-Present and Lifetime Version (K-SADS-PL) (Kaufman et al. 1997). After the evaluation, the cases with ADHD were defined as group I. The healthy volunteers were matched for age and sex with group I and defined as group II.
Exclusionary criteria
For both groups, cases were excluded who had an intelligence quotient (IQ) <80 (Wechsler Intelligence Scale for Children-Revised, a well-known scale for assessing IQ in children between 6 and 16.), (Wechsler 1994) (n = 14), who had an unstable or chronic medical illness (n = 1), who had a history of head trauma (n = 1), epilepsy (n = 7), autistic spectrum disorder (n = 8), and psychosis (n = 1).
Apart from these, 23 cases were excluded with at least one comorbid diagnosis in anxiety (n = 8), oppositional defiant (n = 14), and mood disorders (n = 1). The study was carried out on 65 cases diagnosed with ADHD.
Clinical evaluation and measures
All parents were asked to evaluate their children using the K-SADS-PL, Child Behavior Checklist (CBCL) (Achenbach 2001), Swanson, Nolan, and Pelham–IV Questionnaire (SNAP-IV) (Bussing et al. 2008), and The Griffith Empathy Measure-Parent Rating (GEM-PR) (Dadds et al. 2008) before the medication was administered. All the children were asked to complete the Bryant Index for Empathy (BEI) (Bryant 1982), which evaluates trait empathy level. Subsequently, all children were administered the Diagnostic Analysis of Nonverbal Accuracy-2 (DANVA-2) (Nowicki and Duke 1994) and Empathy Response Task (ERT) (Braaten and Rosen 2000) tests. Child and Adult Faces subtests of DANVA-2 were used to assess facial expression recognition. Each computer-administered subtest includes 24 photographs of child or adult models (12 female, 12 male per subtest) displaying equal numbers of high- and low-intensity expressions of happiness, sadness, anger, and fear. Faces appear for 2 seconds. In a forced-choice format, participants indicate by button press which emotion a face expresses. Dependent variables were total errors of 48 photographs, created separately for each emotion. Child and adult faces subtests and high- and low-intensity expressions were combined to increase power. The participants respond verbally to eight fictitious episodes of ERT. Each episode was presented in the form of a short narrative about a fictitious child and illustrated by a black and white picture in which the character's face was left blank, so that the participants would not be able to gain information about the characters' feelings from facial cues. Each story was scored in two ways, by computing a match score and an interpretation score.
Pharmacological treatment
The children with ADHD in group I were given MPH HCl extended-release tablet (OROS MPH) treatment (0.83 ± 0.21 mg/(kg·d) for per person), which releases MPH by means of osmotic pressure and is a long-lasting and sustained-release pharmaceutical preparation, every morning at the same time (Swanson et al. 2002).
Every 4 weeks, the cases were followed-up by the Children's Global Assessment Scale to determine treatment compliance, efficacy, and side effects (Wagner et al. 2007).
Their parents were asked to complete the CBCL, SNAP-IV, and GEM-PR scales at the end of the 12th week. At the same time, the children in group I completed the BEI. The DANVA-2 and ERT were also applied to these children after treatment for the second time.
Statistical analysis
The data were evaluated using the Statistical Package for the Social Sciences (version 20) program. Descriptive statistics are shown as mean ± standard deviation or frequency (%). A 95% confidence interval was used to assess the data. The chi-square test was applied to categorical variables when comparing demographic data. The t-test was used while evaluating socioeconomic status, means for age, IQ, inattentiveness, hyperactivity, oppositional problem (OP) and CP scores.
In the comparison of GEM-PR, BEI, and the ERT data, which were used to evaluate state empathy and trait empathy, one-way analysis of variance (ANOVA) was used. Hierarchical regression analysis was used to define the effects of OP and CP on the GEM-PR, BEI, and ERT scores if a significant correlation was found between them with Pearson's correlation test. Facial expression recognition test errors were evaluated using repeated-measures analysis of covariance (ANCOVA) by way of 2 (group) × 2 (face-age) × 4 (emotion). The main effects of groups, face ages, and emotions on errors and the effects of face ages and emotions on groups were tested. The significance of F-statistics was interpreted by the least significant difference (LSD) t-test. The differences between pre- and post-treatment measurements were evaluated using ANCOVA. The alpha expressiveness value was regarded as <0.05.
Results
Group I consisted of 53 male children, whereas group II consisted of 46 male children. The average age was 10.86 ± 1.85 (years) and 11.21 ± 1.74 (years), respectively. There was no significant statistical difference between the groups in terms of age (p = 0.275) and gender (p = 0.402). When comparing the socioeconomic status between the groups I and II, there was no significant difference (p = 0.06), and the values were 11.14 ± 2.30 and 10.49 ± 1.54, respectively.
The comparison of IQ, ADHD symptoms, OP, and CP scores between the groups is shown in Table 1.
ADHD, attention-deficit/hyperactivity disorder; CBCL oppositional, standard score of CBCL oppositional problems; CBCL conduct, standard score of CBCL conduct problems scale; IQ (intelligence quotient), standard score of overall WISC-R; PR, parent ratings; SD, standard deviation; SNAP-IV, Swanson, Nolan, and Pelham–IV questionnaire; TR, teacher ratings were symbolized.
The children in the experimental group had higher OP, CP, inattentiveness, and hyperactivity values than the control group.
Following 2 × 2 ANOVA of GEM-PR and ERT scores, there were no significant differences in terms of ADHD status and gender. Gender did not have any effect on the scores of the groups with ADHD and non-ADHD. In the 2 × 2 ANOVA of the BEI, there was no significant difference in terms of ADHD status. Girls reported themselves to be more empathetic than the boys. However, gender did not have any effect on the data in the groups with ADHD and non-ADHD (Table 2).
ERT match is the match score and ERT interpretation is the interpretation score on the Empathy Response Task.
p < 0.05.
ADHD, attention-deficit/hyperactivity disorder; Child empathy, child-reported empathy on the Bryant Index for Empathy; Parent empathy, parent-reported empathy on Griffith Empathy Measurement; SD, standard deviation.
As a result of the correlation analysis, the OP scores only had a significant correlation with the BEI data (r = −0.42, p = 0.000). CP scores had a significant correlation with the GEM-PR, the BEI, and the ERT match subscore (r = −0.26, p = 0.005; r = −0.44, p = 0.000; r = −0.24, p = 0.009; respectively). Following the regression analysis, only CP scores had a significant negative relationship to the GEMP-PR, BEI, and the ERT match subscore (Table 3). The groups did not differ in their facial expression recognition errors (F(1, 122) = 1.69, p = 0.19, partial η2 = 0.01). A significant emotion effect was observed (F(1, 122) = 2.89, p = 0.038, partial η2 = 0.06). LSD t-tests showed that all subjects made more errors on anger than fearfulness, sadness, and happiness expressions; on fearfulness than happiness expressions; and on sadness than happiness expressions (each p < 0.001). There was no significant difference between sadness and fearfulness expression errors (p = 0.4) (Fig. 1).
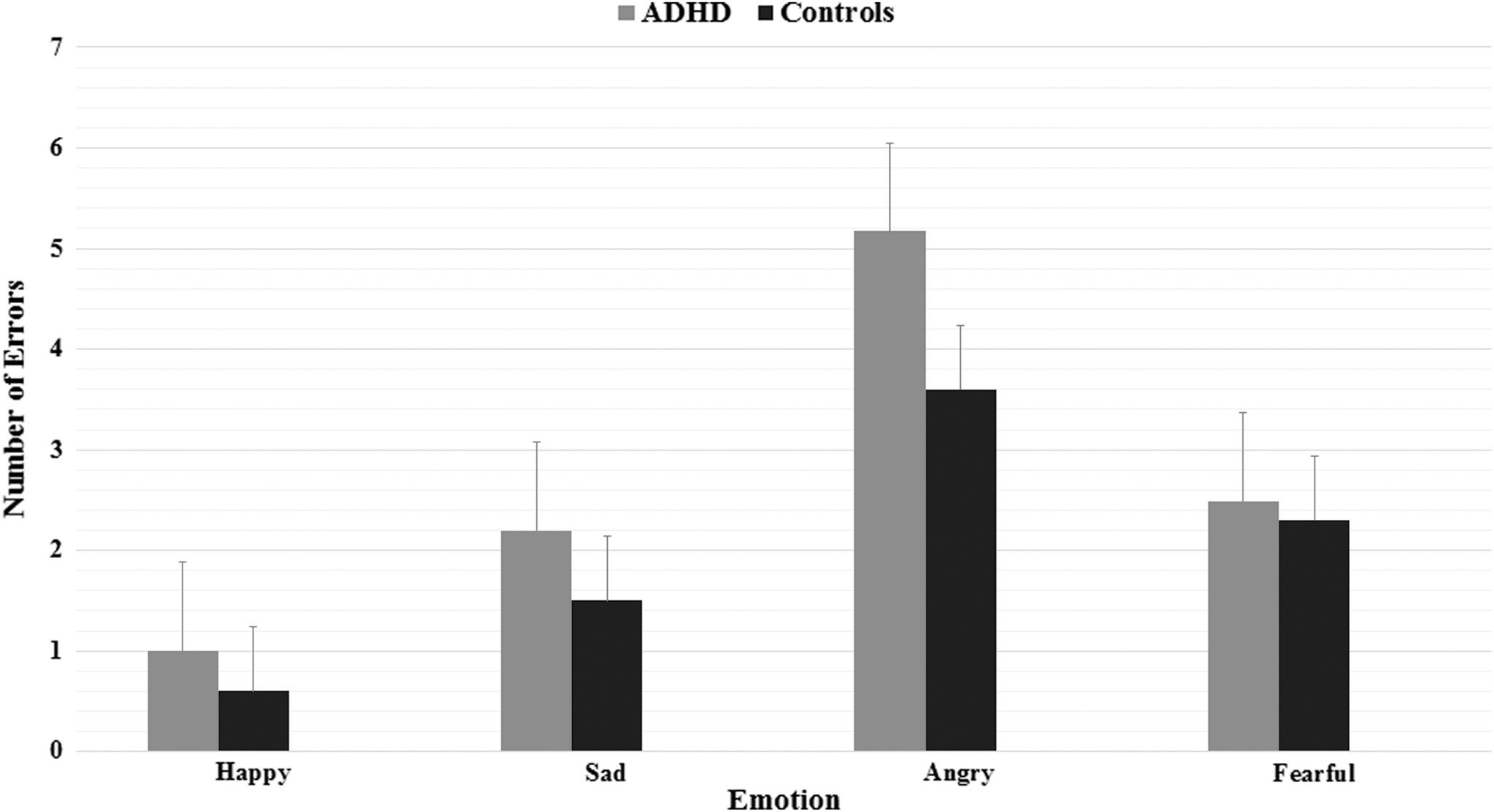
Facial expression recognition errors. Group effect: ADHD and controls did not differ significantly (p > 0.05). Emotion effect: anger>fearfulness, sadness, and happiness; fearfulness and sadness>happiness (p < 0.001); sadness and fearfulness did not differ significantly (p > 0.05). Means adjusted for intelligence quotient. ADHD, attention-deficit/hyperactivity disorder.
Predicting parent-reported empathy: R2 = 0.07. Predicting child-reported empathy: R2 = 0.21 for Step1; ΔR2 = 0.01 for Step 2. Predicting match scores: R2 = 0.06.
p < 0.01.
p < 0.001.
ERT, Empathy Response Task; SE, standard error.
Interactions between group and face-age or emotion were not significant, indicating that the impact of face-age or emotion on errors did not differ across groups.
After the repeated measures were carried out pre- and post-treatment, there was no significant difference in the scores of parent-reported and child-reported empathy in the group with ADHD (trait empathy; p > 0.05). There was no change in ERT match subscores in the empathy task (p > 0.05), yet there was a significant increase in the interpretation subscores (p < 0.05; Table 4). As the effects of CP scores on GEM-PR, BEI, and ERT match subscores were shown by regression analysis, the CP value was checked using ANCOVA when comparing the measures pre- and post-treatment.
Means adjusted for CP.
p < 0.05.
BEI, Bryant Index for Empathy; CP, conduct problem; ERT, Empathy Response Task; GEM-PR, Griffith Empathy Measurement-Parent Reported; SD, standard deviation.
In terms of pre- and post-treatment differences in facial expression recognition errors, errors of happiness and fearfulness did not differ between pre- and post-treatment (F(1, 48) = 3.49, p = 0.06, partial η2 = 0.06 and F(1, 48) = 0.11, p = 0.74, partial η2 = 0.002). However, errors of sadness and anger significantly decreased post-treatment (F(1, 48) = 5.54, p = 0.02, partial η2 = 0.1 and F(1, 48) = 29.17, p < 0.001, partial η2 = 0.38 (Fig. 2).
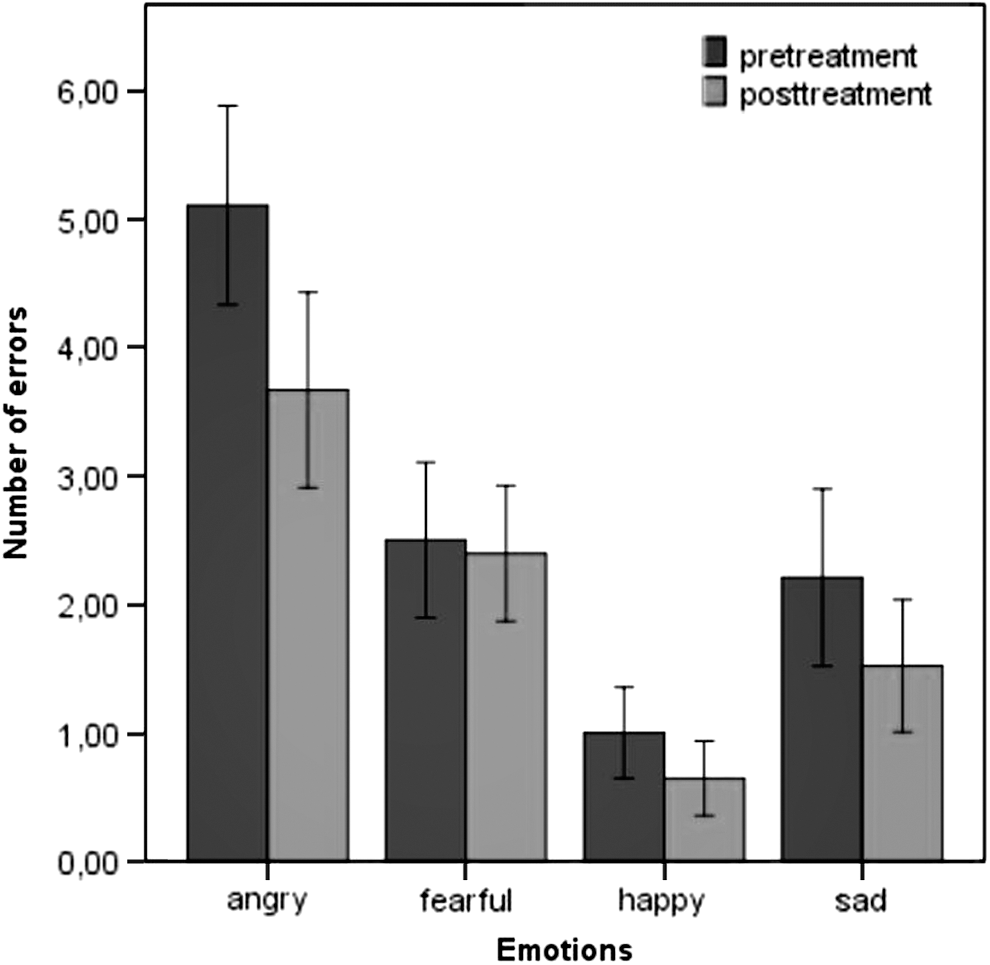
The comparison of facial expression recognition errors in the group with ADHD before and after treatment. Errors of anger and sadness significantly decreased (p < 0.001 and p < 0.05), but happiness and fearfulness did not change (p > 0.05). ADHD, attention-deficit/hyperactivity disorder.
Discussion
In this study, we first aimed to examine whether empathy skills and facial expression recognition levels showed differences between ADHD and non-ADHD groups. Our second aim was to determine whether gender, OP, and CP were significantly associated with trait empathy evaluated using parent-reported and self-reported scales and state empathy levels evaluated by a picture story task (ERT). The third was to evaluate whether MPH improved these parameters in the ADHD group.
Our main results demonstrate that there were no significant differences between groups in terms of trait and state empathy levels. In addition, in these results, no differences were found at the levels of facial expression recognition between the two groups. There are few studies on this subject in the literature. Marton et al. (2009) found that there was no significant difference in self-reported empathy between the children with ADHD and healthy children, whereas children with ADHD had higher scores than healthy children in the parent-reported empathy questionnaire. Schwenck et al. (2011) evaluated cognitive and affective empathy in children with ADHD and conduct disorder by self-reported measures and found no significant difference between groups, similar to our study. It may be said that children with ADHD define themselves as empathic as healthy children. However, more research is needed on parental assessments of children's empathy levels.
In contrast to our study, the ADHD group scored significantly lower than the comparison group on the match task and the interpretation task of ERT in Braaten and Rosen's (2000) study. Schwenck et al. (2011) reported that the healthy control group outperformed in ERT compared to ADHD-combined subtype and conduct disorder, but not to ADHD-predominately inattentive subtype. According to this study, the processing of emotional information seems to differ in ADHD subtypes (Schwenck et al. 2011). Unlike our study, the samples of these two studies (Braaten and Rosen 2000; Schwenck et al. 2011) consisted of only boys. And children with ADHD-predominantly inattentive type were not included in the first study.
Facial expression recognition skills of children with ADHD have been evaluated by DANVA-2 in three studies (Cadesky et al. 2000l; Guyer et al. 2007; Seymour et al. 2013). Guyer et al. (2007), in parallel with our study, showed that children with ADHD or conduct disorder performed similar to the control group on the DANVA-2 test. Some findings in the other two studies do not overlap with our research. Seymour et al. (2013) found that children with ADHD made significantly more errors in facial expression recognition such as anger, sadness, and fearfulness compared to the control group in child faces. There were no significant differences between the two groups in adult faces (Seymour et al. 2013). Cadesky et al. (2000) interestingly showed that the ADHD+CP group performed better than the ADHD and CP groups and was as accurate as the control group. Children with only CP and only ADHD were significantly less accurate at interpreting emotions than normal controls on the DANVA-2 (Cadesky et al. 2000). Detailed new studies are needed to clarify whether ADHD subtypes and CP change levels of facial expression recognition on the DANVA-2.
Looking at the results for our second aim, gender and OP were not found associated with the empathy task and scales, whereas both clinical and nonclinical CP scores led to a significant change in empathy scales and the match subscore of ERT. In contrast to our study, Marton et al. (2009) suggested that the gender and clinical CP score had a significant effect on parent- and child-reported scales of empathy, yet children with ADHD who have nonclinical levels of CP had a similar level of empathy as healthy controls. It can be said that CP at the clinical level was negatively associated with empathy scores. However, the effects of gender, OP, and CP at the nonclinical level on empathy scales are controversial and further studies are needed about this.
Our results for the third aim demonstrate that after 12 weeks of treatment with OROS MPH, the levels of interpretation subscore of ERT significantly increased, whereas the recognition errors of sad and anger expressions significantly decreased and there was no significant change in the levels of parent- and self-reported measures of empathy, the match subscore of ERT, and the errors of happy and fearful expressions in our study. There are only a limited number of studies evaluating the effects of MPH treatment on facial expression recognition, but the DANVA-2 test was not used in these studies. In a study in which event-related potentials were used, the researchers evaluated whether there were some improvements in facial expression recognition in children and adolescents with ADHD after a 4-week MPH treatment. It was reported that there was an increase in the recognition of angry facial expressions, consistent with our study (Williams et al. 2008). In another study, it was found that MPH improved facial expression recognition abilities; however, this improvement was not statistically significant (Beyer von Morgenstern et al. 2014). There have been no studies in the literature to examine whether MPH has caused changes on the ERT and empathy scales. Our study is valuable in that respect. However, it needs to be supported with large-sample and long-term follow-up studies.
There are some limitations in our study. Scores were not examined according to ADHD subtypes. Children with ADHD-predominately inattentive type were found more empathic than children with ADHD-combined type on the ERT in a previous study (Schwenck et al. 2011). The second limitation of our study is that there is no specific information about whether the parent-reported empathy scale is filled by the mother or father, and it may have confounded the results. On the contrary, the different levels of reading skills resulting from the wide age range might have reduced the sensitivity of self-reported measurements. Apart from these, the main limitation of this study is that trait empathy is a skill that can change in the long term, so this study evaluated the posttreatment trait empathy skill changes in the short term (3 months).
Further randomized controlled studies to investigate the long-term effects of MPH treatment on empathy functions and facial expression recognition will provide reliable results. Empathy is a complex structure; any index may show a person's ability to be empathic for a short period. Multiple measurements, such as the measurement of individuals' physiological and facial reactions to the events that may cause empathy, direct observation, and notification of empathic experiences, will provide a more complete perspective of empathy.
Conclusion
From our study, it can be concluded that children with ADHD have similar levels of trait and state empathy and facial expression recognition as healthy controls. CP is negatively associated with empathy skills. MPH increases to recognize negative facial expressions such as sadness and anger and the ability to make empathic interpretations to the picture stories. It would be beneficial to carry out more comprehensive studies, including pharmacogenetic, psychosocial, and environmental factors, to evaluate the cultural diversity.
Footnotes
Clinical Significance
This is one of the few studies in the literature to evaluate differences in both empathy and facial expression recognition skills with multiple measurements between ADHD and non-ADHD groups and the first study to investigate the effects of MPH on these skills. MPH may increase the quality of social relations of children with ADHD especially who have clinical levels of CP by increasing the ability to recognize negative facial expressions and make empathic comments as well as reducing the symptoms of inattentiveness and hyperactivity.
Authors' Contribution
F.G.: study concept and design, acquisition of the subjects and/or data, analysis and interpretation of the data, and preparation of the article. I.Y. and Y.Y.: selection of the patients into the study who met the inclusion criteria, interpretation of the discussion. Y.Y. and S.G.: study concept and design, analysis and interpretation of the data, and preparation of the article. O.S.: study concept and design and preparation of the article, and revised the article critically for important intellectual content. All authors have approved the final version of the article.
Disclosures
No competing financial interests exist. We, the authors of the article, declare that we or any of our family members do not hold any positions (as an employee, shareholder, etc.) in any company that may potentially create a conflict of interest. There has been no conflict of interest during the preparation of the study, data collection, interpretation of results, and article writing.