
Abstract
Objective:
To determine current and lifetime psychopathology and assess quality of life (QoL) in offspring of a parent with bipolar disorder (BD).
Methods:
We investigated 43 offspring of bipolar parents (high-risk offspring [HRO]) (mean age 12.5 ± 3.1; range 6.7–17.9 years) and 43 comparison offspring matched for sex, age, and IQ of healthy parents. Lifetime and current presence of Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5) diagnoses were assessed using Kiddie-Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version (K-SADS-PL). We administered parent and self-report versions of General Behavior Inventory and the Screen for Child Anxiety-Related Emotional Disorders (SCARED). QoL was evaluated using the self-report questionnaire KIDSCREN-52.
Results:
Thirty-seven HRO (86%) and 18 controls (42%) met DSM-5 criteria for at least one lifetime psychiatric diagnosis (adjusted OR = 7.20; 95% CI 2.27–22.81). Compared to controls, HRO had higher lifetime frequency of any mood disorder (33% vs. 2%, p < 0.001), anxiety disorder (60% vs. 14%, p < 0.001), and attention-deficit/hyperactivity disorder (26% vs. 5%, p = 0.01). After adjustment for confounders, only mood (OR = 13.05; 95% CI 1.41–120.60) and anxiety (OR = 9.69; 95% CI 2.75–34.31) disorders remained significantly more frequent in the HRO group. In comparison with controls, HRO scored lower in the following domains: QoL, social support and relationship with peers (p = 0.003; Cohen's d = 0.91), parent relationships and home life (p = 0.008; d = 0.67), as well as self-perception (p = 0.04; d = 0.55).
Conclusions:
In agreement with other studies, we found a higher rate of lifetime anxiety and mood disorders in children and adolescents at confirmed familial risk for BD. Reduction in QoL was already evident across a number of domains. Adult psychiatrists should incorporate into their assessment procedures targeted questions on the presence of psychopathology in offspring of their adult patients with severe mental disorders and child services should bridge with adult services providing accessible services to children of affected parents.
Introduction
B
Accurate diagnosis is challenging especially over the emergent course in young people. As was previously reported in high-risk offspring (HRO) studies, major mood episodes are often preceded by nonmood disorders in childhood, followed in adolescence by subthreshold mood disturbances (Duffy et al. 2002, 2010, 2013; Hillegers et al. 2005; Mesman et al. 2013).
Supporting these prospective observations, a retrospective analysis of bipolar adolescents showed that the majority of patients initially underwent psychiatric treatment for a condition other than BD, including anxiety disorder, unipolar mood disorder, and attention-deficit/hyperactivity disorder (ADHD) (Lázaro et al. 2007; Goetz et al. 2015). These patients are frequently exposed to different psychotropic medications, which may alter the clinical course of evolving psychopathology (Chang et al. 2010; MacKenzie et al. 2016). Therefore, to substantially improve early detection, predictive evidence based on early precursors and other risk factors is needed.
BD is highly heritable with an estimated up to 85% of the variance in risk determined by genetic factors (Smoller and Finn 2003). The family history of BD represents the strongest predictor for the development of BD and first-degree relatives of affected individuals have approximately a 10-fold increased disorder risk compared with relatives of unaffected controls (Smoller and Finn 2003).
Children raised by a parent with BD, not only inherit genetic risk factors but are also exposed to environmental stressors related to having a seriously ill parent and that likely interact with this predisposition to determine illness (Goodday et al. 2015). Therefore, the systematic prospective assessment of offspring of bipolar parents (HRO) is considered the approach of choice to map origins of evolving illness and identify the earliest signs and symptoms and associated biomarkers. Cross-sectional and longitudinal offspring studies reported up to 70% risk for any psychiatric disorder; specifically, these studies demonstrated an elevation of mood disorders, anxiety disorders, neurodevelopmental disorders, and substance use compared to offspring of healthy parents (Hillegers et al. 2005; Duffy et al. 2007; Egeland et al. 2012; Birmaher et al. 2014).
A severe mental disorder in a parent leads to an increase in the level of stress within the family. Thus, it represents a critical factor involving the QoL in children and adolescent offspring (Bee et al. 2014). The term “quality of life” generally refers to an individual's perception of his or her life experience within the context of personal goals, expectations, and beliefs (Group WHO 1995). Measures in one-dimensional models of QoL quantify satisfaction with a single life aspect. Multidimensional models cover satisfaction across a broader range of domains, including physical, emotional, mental, social, and behavioral components of well-being and functioning as perceived by patients and other individuals (Ravens-Sieberer et al. 2013).
It has been reported that youths suffering from BD have significantly lower quality-of-life scores than those with a number of somatic illnesses such as asthma, atopic dermatitis, arthritis, and also in comparison to youths affected with unipolar depression and behavior disorders (Freeman et al. 2009). Mental illness in a parent has been associated with an increased risk for a wide spectrum of emotional and behavioral problems in offspring, as well as impairment of the offspring's physical health; a multidimensional assessment of QoL is recommended (Bee et al. 2013). Surprisingly to our knowledge, only one study has examined QoL in a well-defined sample of a child and adolescent offspring at risk for BD and assessed which factors are associated with the QoL in HRO (Gomes et al. 2016).
The objective of the current study was to determine the current and lifetime prevalence of Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5) diagnoses in the group of children with one parent suffering from BD. We also evaluated the self-reported QoL across a number of domains.
Methods
Sample
High-risk offspring
Subjects were enrolled in the study between January 2012 and November 2015. An invitation letter was sent to the patients on the clinical register of adults with BD (CZ-BDCR) of the National Institute of Mental Health, Klecany, the Czech Republic, who registered offspring within an age range of 6 to 17 years. In addition, we contacted three psychiatric hospitals with outpatient services in rural and urban regions of the country. Psychiatrists of these facilities were requested to ask adults treated for BD if they were interested in participating in the project. After a complete description of the study and a brief interview, the families were selected according to inclusion and exclusion criteria.
Inclusion criteria: (1) parent diagnosed with bipolar I or II disorder, (2) signed informed consent by the parent/caregiver and offspring, and (3) the offspring aged 6–17. Exclusion criteria: (1) intellectual or major physical disability in offspring, (2) noncompliance with the study protocol, and (3) the second parent with a major mood or psychotic disorder.
Controls
The controls were recruited by advertising in schools. Parents were asked to contact the research team only if they were not diagnosed with a psychiatric disorder, were not treated with psychotropic drugs, and there were no severe health complications during pregnancy potentially impairing the intrauterine development of the offspring. From the families interviewed, we selected those with an offspring matching with those from the high-risk group by sex and age.
Instruments
Both the high-risk group and control group underwent the same set of assessment.
Parental assessment
Parents were assessed in the National Institute of Mental Health, Klecany, the Czech Republic. The majority of parents with BD (proband parents) were recruited from the Czech Bipolar Disorder Case Registry (CZ-BDCR) (N = 24; 71%). Briefly, CZ-BDCR is a database of patients with BD confirmed by Schedule for Affective Disorders and Schizophrenia—Lifetime Version (SADS-L) (Endicott and Spitzer 1978) interview when entering and then their course of illness is annually reassessed. Patients with BD from the CZ-BDCR have participated in several genetic and neuroimaging studies of BD (Lachman et al. 2007; Hajek et al. 2010, 2013).
The other bipolar parents were those who contacted the study team after they received information about the project from their treating psychiatrist. The diagnosis of BD in CZ-BDCR nonparticipants was confirmed using SADS-L by an adult psychiatrist who also performed interviews during the creation of CZ-BDCR. The parents of the control offspring were interviewed by a board-certified psychiatrist to exclude families with mentally ill parents or those who were treated with psychotropic medication.
Offspring assessment
Semistructural psychiatric interviews
Semistructural psychiatric interviews following the Kiddie-Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version (K-SADS-PL) (Kaufman et al. 1997) were performed independently with child and parent by a board-certified child psychiatrist. The K-SADS-PL is an interviewer-oriented diagnostic interview designed to assess current and past psychiatric symptoms by interviewing the parent(s) and child separately. First, we conducted interviews with parents about the child and then with the children themselves. If parents and child disagreed on the presence of a symptom, greater weight was typically given to parents' reports of observable behavior and children's reports of subjective experiences (Kaufman et al. 1997). The interviewer was blinded to rating scale results since the scales were administered and evaluated after the interview.
Assessment of mood symptoms
For the general screening of mood symptoms, we used the General Behavior Inventory (GBI). The GBI was designed as a self-report measure for use by adults to identify bipolar and unipolar mood disorders across the full spectrum of severity. It contains 73 questions reflecting both the intensity and duration of symptoms (Depue et al., 1989). The GBI is composed of three sets of items, which can be scored on two scales: a Depression scale with 46 items and a Hypomania/Biphasic scale with 21 hypomanic and 7 biphasic items. Each item is rated on a four-point scale of intensity, 0 = “hardly ever,” 1 = “sometimes,” 2 = “often,” and 3 = “very often.” Till the age of 12, the GBI was read to children and the older offspring completed instrument by themselves.
In addition to self-report, a parent/caregiver version (Parent-GBI [P-GBI]) of this questionnaire was administered. GBI was adapted for use by primary caregivers as shown in a study Youngstrom et al. (2001) and contains the same set of items as the self-assessment version. The caregiver report on the P-GBI manifested an excellent discriminative validity among youths with formally diagnosed Axis I mood disorders and those without an Axis I diagnosis.
Assessment of anxiety symptoms
The Screen for Child Anxiety-Related Emotional Disorders (SCARED) (Birmaher et al. 1997) was used. SCARED is a self-report and parent report multidimensional instrument that was developed as a screening tool for childhood anxiety disorders. It contains 41 questions assessing symptoms of panic, generalized anxiety, separation anxiety disorders, and social phobia, as well as simple phobia and school phobia. SCARED demonstrated a satisfactory internal consistency and discriminant validity (both between anxiety and depressive and disruptive disorders and within-individual anxiety disorders) (Birmaher et al. 1999).
IQ was assessed using Raven's progressive matrices.
Assessment of the QoL
We used the 52-item version of the self-report questionnaire KIDSCREEN (Ravens-Sieberer et al. 2005, 2008) developed by European pediatric researchers for use in epidemiologic public health surveys, clinical intervention studies, and research projects. KIDSCREEN is based on the definition of QoL as a multidimensional construct covering physical, emotional, mental, social, and behavioral components of well-being and functioning as perceived by patients and other individuals.
Statistics
The demographic and clinical characteristics between the high-risk and control groups (parents and offspring) were compared using the unpaired t-test, Mann–Whitney U test, chi-square, and Fisher's exact tests as appropriate. Between-group differences in rates of K-SADS/DSM-5 diagnoses were assessed by Fisher's exact tests followed by logistic regressions to adjust for confounding factors (living with both biological parents, non-BP disorders in parents, education of parents, trauma in child's history, and more children from one family).
While taking into account the age at onset of the mood disorder, we applied the Kaplan–Meier survival analysis with the log-rank test. Kruskal–Wallis ANOVA followed by Mann–Whitney U tests as a post hoc test with a corrected level of significance and chi-square tests were used for comparisons of subgroups within HRO. Between-group differences in parental and self-assessment were controlled for co-occurring conditions (DSM-5 disorders) with the use of logistic regression. Cross-informant (parent–child) agreement in the assessment of symptoms of mood and anxiety disorders was calculated as Kendall's rank correlation coefficient (tau) and concordance correlation coefficient (CCC) for an ordinal rating and Cohen's kappa for a dichotomous rating.
To compare the KIDSCREEN (QoL) between groups, the raw scores were converted to the T scores (The KIDSCREEN Group Europe 2006) and unpaired t-tests were conducted followed by Cohen's d calculation and least-square multiple regression to control for between-group differences for current psychopathology and family status. Statistical analyses were performed using STATISTICA (data analysis software system) version 9.1 and MedCalc Statistical Software version 13.1.2.
Results
Parents
Parental characteristics are presented in Table 1. With respect to demographic differences, there were fewer intact bipolar families compared to controls (47% vs. 76%; p = 0.02). Moreover, mothers in bipolar families were less well educated than mothers in the control families (p = 0.001). Substance abuse was more frequent in the bipolar families (p = 0.05) than in controls, while no significant difference between families was found for anxiety disorders. BD I was diagnosed in 74% of proband parents, 1/3 of whom were treated with lithium. Lifetime psychotic symptoms accompanying BD were present in 25% of the proband parents.
Fisher's exact test.
Pearson chi-square test.
Includes alcohol, marijuana, and amphetamines.
BD, bipolar disorder; E/H/U, Elementary/High school/University; F, female; M, male; n/a, nonapplicable; SD, standard deviation.
Offspring
We enrolled 43 offspring from 34 families with 1 parent with confirmed BD (HRO) (mean age 12.5 ± 3.1; range 6.7–17.9 years). We also enrolled 43 offspring from 33 families in which neither parent met lifetime criteria for a major mood or psychotic disorder (controls). The demographic characteristics of the offspring are shown in Table 2. The HRO were sex and age matched with the offspring from control families. There were no significant differences in IQ between high-risk and control groups (115 ± 16 vs. 116 ± 14; p = 0.68).
Fisher's exact test.
Unpaired t-test.
Mann–Whitney test.
Estimated by Raven's Progressive Matrices.
GAF, Global Assessment of Functioning; n/a, not applicable; PPCC, pedagogical–psychological counseling center; SD, standard deviation.
DSM-5 diagnoses in offspring
Lifetime mental disorders
Thirty-seven HRO (86%) and 18 controls (42%) met the criteria for at least one lifetime diagnosis (Fisher's exact test, p < 0.001; adjusted OR = 7.20; 95% CI 2.27–22.81) (Table 3).
Includes alcohol, marijuana, and amphetamine.
p < 0.05, ** p < 0.01, *** p < 0.001; Fisher's exact test.
ADHD, attention-deficit/hyperactivity disorder; BD II, bipolar disorder second type; BD NOS, bipolar disorder not otherwise specified; CD, conduct disorder; dis., disorder; GAD, generalized anxiety disorder; LD, learning disabilities; MDD, major depressive disorder; OCD, obsessive–compulsive disorder; ODD, oppositional defiant disorder; PTSD, posttraumatic stress disorder.
Anxiety disorders were the most frequent lifetime diagnoses in both groups. However, HRO showed a significantly higher risk for anxiety disorder compared with controls (60% vs. 14%; p < 0.001; OR = 9.69; 95% CI 2.75–34.31) with the generalized anxiety disorder being the most frequent.
Any lifetime mood disorder was found in 33% of HRO and in 2% of controls (p < 0.001; OR = 13.05; 95% CI 1.41–120.60). When age at onset of mood disorder was taken into account in survival analysis, the risk ratio remained similar (log-rank test, χ2 = 10.61, df = 1, p = 0.001, hazard ratio = 13.40; 95% CI 4.29–41.66, Fig. 1).
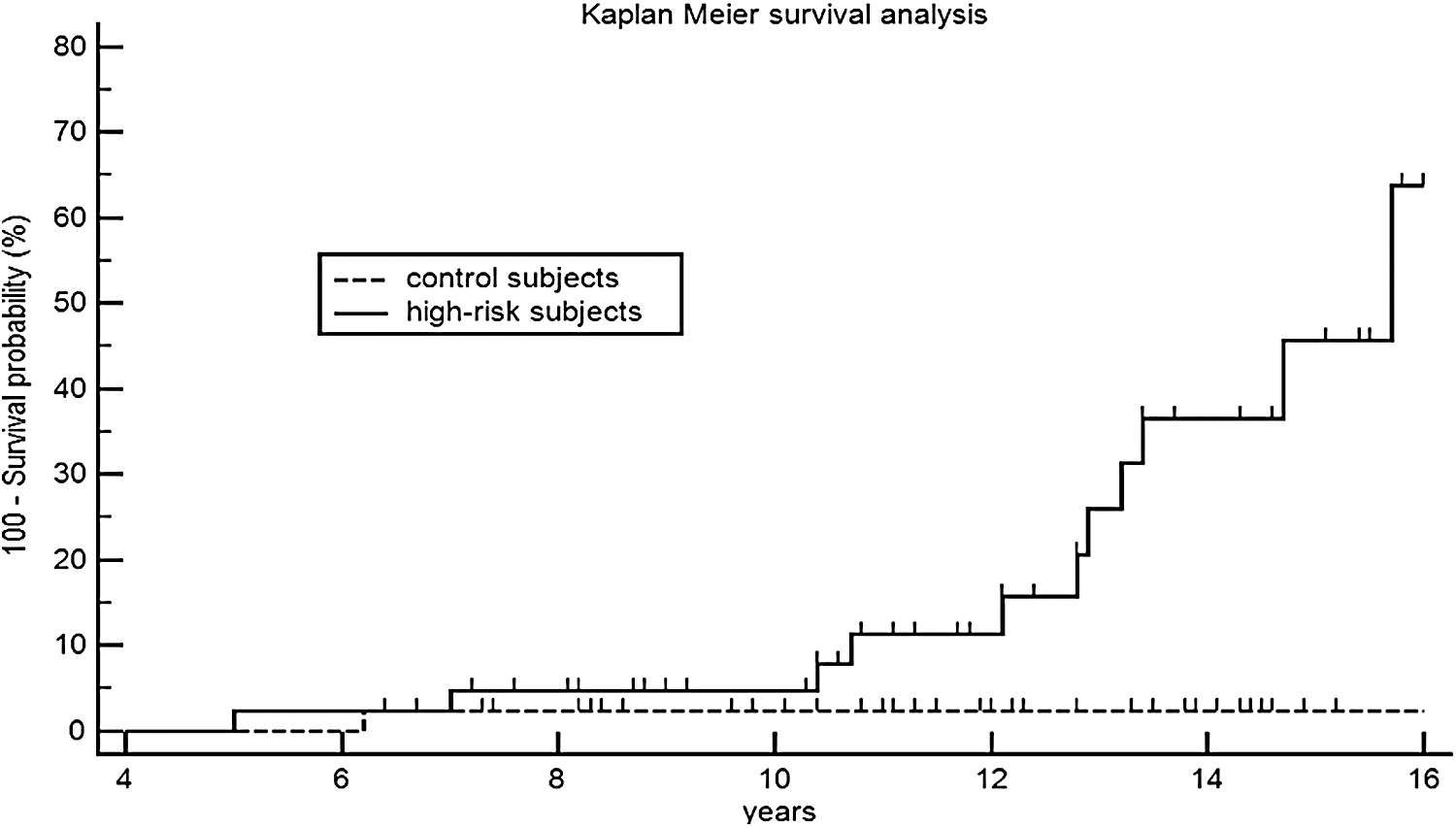
Comparison of survival curves for mood disorders between high-risk offspring and controls.
In Table 4, we report details on age of onset for psychiatric disorders and comorbidity for HRO meeting DSM-5 lifetime criteria for mood disorder.
Current disorder.
ADHD, attention-deficit/hyperactivity disorder; BD II, bipolar disorder second type; BD NOS, bipolar disorder not otherwise specified; CD, conduct disorder; F, female; GAD, generalized anxiety disorder; LD, learning disabilities; M, male; MDD, major depressive disorder; NA, not applicable; NOS, not otherwise specified; OCD, obsessive–compulsive disorder; ODD, oppositional defiant disorder; PD, panic disorder; PTSD, posttraumatic stress disorder.
We found five cases of bipolar spectrum disorder, all of them had lifetime comorbidity of anxiety disorders, adolescents had also comorbidity of substance use, lifetime ADHD (inattentive type) was present in two cases. Three offspring who were diagnosed with BD NOS and fulfilled the criteria for a major depressive episode did not meet the duration criterion for a manic episode. They had several 2–3 days of lasting episodes of an elevated level of energy, euphoric mood, a markedly increased goal-directed behavior, a decrease in the need for sleep, unusual talkativeness, diminished anxiety, and uncharacteristically increased sociability. In all bipolar subjects, the first mood episode had depressive polarity. The average age of onset of first depression was 10.4 ± 3.7 years and 13.4 ± 3.0 of the first hypomania.
Significant differences between HRO and control offspring were found for lifetime ADHD (26% vs. 5%; p = 0.01), but the difference did not survive after adjustment for living with both biological parents, non-BP disorders in parents, education of parents, trauma in child's history, and more children from one family (OR = 5.23; 95% CI 0.90–30.24; p = 0.06). Out of 11 cases with ADHD in the high-risk group, majority (7) were diagnosed with lifetime inattentive type, others had a combined subtype. In the control group, both children with ADHD suffered from a combined subtype.
Fourteen HRO (33%) reported a lifetime history of suicidal ideation, no case was found in the control group (p < 0.001). While children reported the occurrence of suicidal thoughts in association with anger (n = 6), adolescents (n = 7) reported having suicidal thoughts when feeling depressed. Four high-risk adolescents (9%) had a history of suicidal attempts; no case was found among the group of control children. Self-injurious behavior was found in eight cases in the high-risk group (19%) and one case (2%) in controls (p = 0.03).
Lifetime comorbidity
The lifetime comorbidity in HRO was high. Only seven offspring (16%) suffered from just one lifetime mental disorder. Up to 3 diagnoses were present in 23 subjects (54%), up to 6 in 11 (25%), and finally, 2 HRO (5%) had more than 6 lifetime DSM-5 diagnoses. The majority of HRO who were diagnosed with mood disorder also suffered from anxiety disorders in their lifetime. Table 5 shows the comorbidity within the sample.
Including bipolar disorder II, bipolar disorder not otherwise specified, cyclothymia, major depressive disorder, depression not otherwise specified, and dysthymia.
Including panic attack, generalized anxiety disorder, school phobia, specific phobia, social anxiety, and separation anxiety.
ADHD, attention-deficit/hyperactivity disorder; CD, conduct disorder; LD, learning disabilities; N, number; ODD, oppositional defiant disorder.
Current diagnoses
Thirty-three of HRO (77%) and 10 controls (23%) met the criteria for at least one current DSM-5 diagnosis at the time of the interview (p < 0.001; OR = 8.10; 95% CI 2.74–24.01). Out of five cases with BD, one boy was euthymic and four of them were currently depressed. In total, 12 cases in the high-risk group (28%) were diagnosed as having current mood disorder (for details see Tables 3 and 4).
No case of major mood disorder was diagnosed in the control group (p < 0.001). Significant differences between groups were also found in current frequency of anxiety disorders (51% in HRO vs. 12% in controls; p < 0.001), ADHD (26% in HRO vs. 5% in controls; p = 0.01), and oppositional defiant disorder (21% in HRO vs. 2% in controls; p = 0.02).
High-risk children and adolescents in comparison with controls had significantly higher total scores on anxiety symptoms (SCARED) according to parental assessment (HRO mean 18.3 ± 14.1 vs. controls 8.1 ± 6.3, p < 0.001) as well as in self-assessments (19.6 ± 11.5 vs. 14.4 ± 7.9, p = 0.02). When compared to controls, significantly more HRO exceeded the SCARED cutoff score (≥25) (parental assessment 23% vs. 2%, p = 0.005; self-assessment 41% vs. 14%, p = 0.007).
Groups differed significantly also in subscales for symptoms of particular anxiety disorders, including Somatic/panic (HRO mean 2.6 ± 3.7 vs. controls 0.4 ± 0.7, p < 0.001), Generalized anxiety (4.2 ± 3.6 vs. 2.3 ± 2.3, p = 0.01), Separation anxiety (3.8 ±3.7 vs.1.4 ± 1.8, p = 0.001), School phobia (2.1 ± 2.4 vs. 0.4 ± 0.6, p = 0.001), but not for Social phobia (4.4 ± 3.3 vs. 3.6 ± 3.4, p = 0.19) in parental assessment. In self-assessments, significant differences were found for Generalized anxiety (5.1 ± 3.4 vs.3.3 ± 2.7, p = 0.02) and School phobia (1.7 ± 1.8 vs. 1.0 ± 1.3, p = 0.04) but not for Separation anxiety (3.5 ± 2.8 vs. 2.9 ± 2.2, p = 0.40), Social phobia (4.5 ± 2.8 vs. 4.7 ± 3.2, p = 0.73), and Somatic/panic symptoms (3.5 ± 4.2 vs. 2.3 ± 2.3, p = 0.36).
The parent–child correlation of the scores of symptoms in the HRO group for the total anxiety score was significant with a moderate agreement (Kendall's tau = 0.54; p < 0.001; CCC = 0.67). A similar agreement was found when the cutoff scores for anxiety disorders were applied (Cohen's kappa of 0.55). On the contrary, the parent–child agreement in the control group was unsatisfactory low.
When compared to controls, high-risk children and adolescents had significantly higher total scores on symptoms of depression (HRO mean 16.0 ± 15.2 vs. controls 2.2 ± 3.3, p < 0.001) as well as higher hypomanic/biphasic scores (7.3 ± 10.0 vs.1.2 ± 1.4, p < 0.001) on the GBI scale according to parental assessment. Significant differences between self-assessment scores were found only for depression scores (HRO mean 24.3 ± 26.8 vs. controls 12.3 ± 15.2, p = 0.027), but not for hypomanic/biphasic scores (15.3 ± 15.6 vs. 10.1 ± 10.2, p = 0.13).
The HRO with mood disorder differed significantly from the controls but also from healthy HRO not only in scores for symptoms of mood disorder but also in scores for symptoms of anxiety. They also had lowest scores of functioning (for more details see Table 6). An additional regression analysis revealed that the only predictor for exceeding the cutoff score in SCARED is current mood disorder (OR = 9.32; 95% CI 1.58–55.03; p = 0.01) but not risk status (HRO vs. controls: OR = 1.66, 95% CI 0.44–6.33, p = 0.46) or presence of other co-occurring conditions (ADHD, and even anxiety disorders).
High-risk offspring (HRO) with current DSM-5 mood disorder (may be comorbid with other disorders).
HRO with DSM-5 anxiety disorder (may be comorbid with other disorders with exception of mood disorder).
HRO with DSM-5 behavioral and neurodevelopmental spectrum disorder (no anxiety or mood disorder comorbidity).
Kruskal–Wallis ANOVA.
Significant difference compared to controls (Mann–Whitney U test or χ2 test with corrected p < 0.005).
Significant difference to healthy HRO (p < 0.005).
χ2 test.
GAF, Global Assessment of Functioning; GBI, General Behavior Inventory; HRO, high-risk offspring; N, number; SCARED, Screen for Child Anxiety-Related Emotional Disorders; SD, standard deviation.
Quality of life
Compared to controls, HRO scored lower in 5 out of 10 specific domains in KIDSCREEN-52. These domains were as follows: physical well-being (Cohen's d = 0.60; p = 0.01); psychological well-being (d = 0.46; p = 0.05); social support and relationship with peers (d = 0.91; p < 0.001); parent relationship and home life (d = 0.67; p = 0.004), and self-perception (d = 0.55; p = 0.02). After adjustment for current psychopathology (mood and anxiety symptoms), only three domains remained significant: social support and relationship with peers (p = 0.003); parent relationship and home life (p = 0.008), and self-perception (p = 0.04). The latter variable was not found significant after additional adjustment for family status (complete/incomplete family) (for details see Table 7).
KIDSCREEN-52 = Multidimensional Quality of Life Questionnaire, SD, data are presented as T scores.
Unpaired t test.
p-Value after adjustment for mood and anxiety symptoms (GBI and SCARED scores) using multiple regression analysis.
p-Value after adjustment for mood and anxiety symptoms (GBI and SCARED scores) and family status (complete/incomplete) using multiple regression analysis.
GBI, General Behavior Inventory; SCARED, Screen for Child Anxiety-Related Emotional Disorders; SD, standard deviation.
Discussion
The current study evaluated a sample of child and adolescent offspring at risk for BD because of confirmed illness in one parent. We found that 86% of HRO suffered from at least one lifetime axis-I DSM-5 diagnosis. Reported rates of lifetime mental disorders in bipolar offspring studies vary substantially from 44% to 92% (Hammen et al. 1987; Todd et al. 1996; Chang et al. 2000; Wals et al. 2001; Birmaher et al. 2009; Nurnberger et al. 2011; Vandeleur et al. 2012; Duffy et al. 2014). A major factor contributing to reported differences in the frequency and spectrum of mental disorders may relate to methodology, including the process of family ascertainment, assortative mating, and the assessment of parents and offspring (Duffy et al. 2011). However, despite differences in absolute risk, there is convergence across all studies that offspring of bipolar parents manifest a range of lifetime disorders. This likely reflects both the genetic risk and the environmental context.
Specifically, the findings of the frequency of ADHD in samples of bipolar offspring differ markedly across studies: 5% (Hillegers et al. 2005), 9% (Duffy et al. 2014), 8%, 8% (Vandeleur et al. 2012) versus 25%, (Birmaher et al. 2009), 28% (Chang et al. 2000), 31% (Singh et al. 2007). However, in some studies, including our own, the risk of ADHD is comparable between HRO and controls when other confounders such as socioeconomic status (SES) and assortative mating are adjusted for. Interestingly, this is not clear-cut, as in some subtypes of BD such as more psychotic spectrum/lithium nonresponsive, ADHD may represent an antecedent of BD in HRO (Duffy 2012; Sanchez-Gistau et al. 2015). Our results indirectly support this finding, as the majority of bipolar parents in our sample were not treated with lithium.
Similarly, variable combinations of anxiety disorders have been reported in offspring studies, which predict for subsequent mood disorder (Nurnberger et al. 2011; Duffy et al. 2013; Park et al. 2015) and do not appear to be associated with a higher familial risk of comorbid anxiety in these high-risk families.
Anxiety disorders were among the most frequent lifetime and current diagnoses in the HRO in our study. Although lifetime presence of anxiety disorder was also common in the control group, there were substantial differences between groups in the frequency of particular subtypes of anxiety disorders. Especially generalized anxiety was markedly more frequent in the high-risk group compared to controls, and panic disorder was present only in the HRO group. Specifically, panic attacks were found to be associated with earlier onset of BD. Our results are consistent with this finding. Out of four children and adolescents from our sample who were diagnosed with disorder from bipolar spectrum, three subjects had a comorbidity of panic disorder.
Nurnberger et al. (2011) found that among subjects manifesting major affective disorders (n = 33) in their HRO study, there was an increased risk of anxiety disorder compared with cases without mood disorder. We found that HRO with current mood disorder had the highest scores for symptoms of anxiety in comparison with HRO with other than mood disorder. This differentiated them not only from controls but also from healthy HRO. Furthermore, a current mood disorder increased the risk for exceeding the cutoff score for diagnosis of anxiety disorder in anxiety disorder questionnaire nine times. It was suggested that there might be shared genetic factors between bipolar spectrum and anxiety disorders (Gatt et al. 2015). Trait anxiety is considered an endophenotype of bipolar I disorder (Contreras et al. 2010). In adult patients with BD, anxiety disorders are markedly manifested even in the euthymic period (Pavlova et al. 2015).
Interestingly, anxiety disorders in the HRO were not significantly associated with a higher familial risk of anxiety disorders (Duffy et al. 2013). Also in our study, the rate of anxiety disorders in the bipolar parent was surprisingly low compared to the high frequency of anxiety disorders in their offspring. It may very well be that anxiety is a nonspecific presentation of psychopathology risk in vulnerable children or a general indicator of reactivity or sensitivity to stress, which itself may contribute to the risk of various disorders together with more disease-specific risk factors.
Lifetime rate of mood disorders was 33% in our sample. In already published studies, the frequency of mood disorders grows with an increase of average age of the sample. Thus, among offspring of bipolar parents, mood disorder rates of 2.5% were found for preschool offspring (Birmaher et al. 2010); in school age children the rate was 21% (Wals et al. 2001; Birmaher et al. 2009), 27% in adolescent sample, and 51% and 55% in adults (Hillegers et al. 2005). However, some studies, including our own, included also Depression NOS, while other studies did not. On the contrary, Vandeleur et al. (2012) included subthreshold depression, which corresponds with Depression NOS and their reported frequency of any mood disorder was 34.5%, as in our sample. Again risks would be expected to vary as the penetrance across families for BD is highly variable and affected by the nature of assortative mating and environmental context of the family (i.e., cohesion, SES).
The rate of manic symptoms in our sample of HRO was low. While in Longitudinal Assessment of Manic Symptoms (LAMS) study. (Horwitz et al. 2010), the average score in the 10-item mania subscale score in positive screen group was 18.6 ± 4.7, the average score in our mood disordered HRO was only 5.5 ± 3.9, which is below the screening positive cutoff in LAMS (≥ 12).
It prompted us to compare our GBI scores with those reported by Reichart et al. (2004) in their bipolar offspring study. While in the Reichart's study, their HRO (N = 32) with mood disorder had an average score in the depression subscale of 31.75, we had 48.1 and for mania/biphasic score, Reichart et al. reported an average score of 16.6 while we had 29.4. This could be explained by the differences between ours and Reichart's sample. We report scores in the HRO with current mood disorder, while Reichart et al. reported GBI of offspring with lifetime mood disorder. However, GBI scores in HRO with no disorder were pretty much the same in both samples (8.46 vs. 8.0 for depression and 5.96 vs. 5.0 for mania and biphasic).
We found five cases of bipolar spectrum. Manic symptoms in these offspring were mild and did not interfere markedly with functioning. No case of full-blown mania in prepubertal children occurred in our sample. This is not surprising as also other research teams consider prepubertal or early adolescent mania rare even in high-risk samples (Hillegers et al. 2005; Duffy et al. 2009). However, judging by other studies, rates will increase significantly by late adolescence and young adulthood. Out of our five offspring with BD spectrum, three were diagnosed with BD NOS. Although some authors have not assessed diagnoses of BD NOS, we consider this category clinically meaningful. Conversion from BD NOS to BD I or II was found in 38% of children during 4 years in the Course and Outcome of Bipolar Youth Study (Birmaher et al. 2014) and 33% over 18 months in the Multifamily Psychoeducational Psychotherapy study (Martinez and Fristad 2013).
A frequent finding of depressive and anxiety psychopathology in HRO opens the debate about the treatment approaches for this population. The dilemma in high-risk and symptomatic (but not clearly manic or hypomanic) children is whether to treat preventatively symptoms that might happen later (i.e., begin mood stabilizer), treat what is happening now (anxiety and/or depression), or do nothing if the symptoms are not impairing. Pragmatic clinical approach probably should suggest discussing this with the family and treating the present condition that impairs functioning and QoL appropriately. Being unduly preoccupied by the potential risk of uncertain mania may not be the best clinical strategy, particularly as we do not have consistent data on the risk and benefits of pharmacologic treatment (Carlson et al. 2000; Tillman and Geller 2006; Chang et al. 2010; MacKenzie et al. 2016).
In the self-assessment of the QoL, HRO reported lower satisfaction than controls in 5 out of 10 domains, including physical health, psychological well-being, family and peer functioning, and self-perception. This might partially be explained by higher frequency of psychopathology from mood and anxiety spectrum in the high-risk group compared to controls.
Gomes et al. (2016) found that in comparison to healthy HRO and controls, children and adolescents with BD reported lower satisfaction self, relationship, environment, and general domains in Youth Quality of Life Instrument-Research version (YQoL-R). However, differences in parent relationship and home life, peer functioning, and self-perception remained significant even after controlling for mood and anxiety symptoms. This means that other factors are involved.
Family environment plays a crucial role in QoL in the pediatric population. Families with BD parents have lower cohesion, organization, and higher levels of conflict (Chang et al., 2001; Ferreira et al., 2013). Families with BD parent were significantly more often divorced than families of control offspring in our sample. We found that family status is significantly involved in most domains, however, even this factor failed to explain the differences in peer relationships as well as parent relationship and home life domains entirely. We did not collect data on current status of parental mood disorder, therefore we can only speculate that this might represent another factor involving HRO QoL especially in family domain.
Prospective evaluation of the sample will bring more clarification as to the relationship between a course of emotional symptoms, maturation of the subjects in the study, course of parental disorder, and awareness of the particular domains of QoL. These interactions are probably very complex and deserve further research attention.
Limitations
The current study possessed several limitations that must be taken into consideration. The willingness of parents to participate in the study might reflect their concerns about their offspring mental health, increasing the risk of a reporting bias. Furthermore, due to scarce funding, we could not make the interviewers blind to the parent status (control vs. bipolar). We did not have reports from schools of all children and adolescents included in our study, therefore, our insight into the manifestation and severity of psychopathology is only partial. Finally, data on lifetime psychopathology are based on retrospective assessment. Therefore, there might be a recall bias.
Conclusions
In agreement with other studies, we found a high prevalence of multiple lifetime mental disorders in offspring at specific familial risk of developing bipolar and related disorders and they reported lower QoL in several domains than the offspring of healthy parents. Furthermore, while for most HRO in our study, the research assessment was the first ever psychiatric assessment, they had a long history of mental problems.
Clinical Significance
Our study described offspring of bipolar parent as a group at high risk for a wide range of anxiety and mood psychopathology and also having impaired QoL across a number of domains. It clearly implicates the need for proactive and complex care about families of parents with mental disorder. This could be achieved with regular communication and bridging between adult and youth psychiatric services, with adult services inquiring about children of affected parents and readily referring them to engaging and available specialized child and adolescent services.
Footnotes
Acknowledgments
This study was supported by research grant AZV (Agency for the Czech Republic health research) 17-32478A and by the project (Ministry of Health, Czech Republic) for conceptual development of research organization 00064203 (University Hospital Motol, Prague, Czech Republic). This study is also a result of the research funded by the project Nr. LO1611 with a financial support from the MEYS under the NPU I program (NIMH-CZ). The study was presented at the 61 Annual Meeting of the American Academy of Child and Adolescent Psychiatry; October 20–25, 2014; San Diego, CA. We thank Paul Grof and Anne Duffy for their helpful comments on this manuscript preparation.
Disclosures
Dr. Goetz has received research support from Charles University in Prague and Czech Ministry of Health. He served as a speaker for Eli Lilly CR in the last 3 years. Dr. Sebela has nothing to disclose. Dr. Mohaplova has nothing to disclose. Dr. Ceresnakova has nothing to disclose. Dr. Ptacek has nothing to disclose. Dr. Novak has received research support from Charles University in Prague, Czech Ministry of Health, and Czech Ministry of Education, Youth and Sports. He worked as a statistical consultant in the National Institute of Mental Health, Klecany, Czech Republic.