
Abstract
Objectives:
The clinical presentation of pediatric obsessive–compulsive disorder (OCD) is heterogeneous, which is a stumbling block to understanding pathophysiology and to developing new treatments. A major shift in psychiatry, embodied in the Research Domain Criteria (RDoC) initiative of National Institute of Mental Health, recognizes the pitfalls of categorizing mental illnesses using diagnostic criteria. Instead, RDoC encourages researchers to use a dimensional approach, focusing on narrower domains of psychopathology to characterize brain–behavior relationships. Our aim in this multidisciplinary pilot study was to use computer vision tools to record OCD behaviors and to cross-validate these behavioral markers with standard clinical measures.
Methods:
Eighteen youths with OCD and 21 healthy controls completed tasks in an innovation laboratory (free arrangement of objects, hand washing, arrangement of objects on contrasting carpets). Tasks were video-recorded. Videos were coded by blind raters for OCD-related behaviors. Children's Yale-Brown Obsessive Compulsive Scale (CY-BOCS) and other scales were administered. We compared video-recorded measures of behavior in OCD versus healthy controls and correlated video measures and clinical measures of OCD.
Results:
Behavioral measures on the videos were significantly correlated with specific CY-BOCS dimension scores. During the free arrangement task, more time spent ordering objects and more moves of objects were both significantly associated with higher CY-BOCS ordering/repeating dimension scores. Longer duration of hand washing was significantly correlated with higher scores on CY-BOCS ordering/repeating and forbidden thoughts dimensions. During arrangement of objects on contrasting carpets, more moves and more adjustment of objects were significantly associated with higher CY-BOCS ordering/repeating dimension scores.
Conclusion:
Preliminary data suggest that measurement of behavior using video recording is a valid approach for quantifying OCD psychopathology. This methodology could serve as a new tool for investigating OCD using an RDoC approach. This objective, novel behavioral measurement technique may benefit both researchers and clinicians in assessing pediatric OCD and in identifying new behavioral markers of OCD.
Clinical Trial Registry:
Development of an Instrument That Monitors Behaviors Associated With OCD. NCT02866422.
Introduction
O
Given this heterogeneity, using Diagnostic and Statistical Manual of Mental Disorders (DSM)-based diagnostic categories in research designs have been a stumbling block to understanding the pathophysiology of OCD and to developing new treatments. A recent major shift in psychiatry, embodied in the Research Domain Criteria (RDoC) initiative (Insel et al. 2010) of the National Institute of Mental Health, has recognized this problem and encourages researchers to use a dimensional approach to analyses, focusing on narrower domains of psychopathology, rather than diagnostic categories. The ultimate goal of RDoC is to tease apart heterogeneity and allow clinicians to make more precise assessments and to tailor treatment based on the biology of each patient. RDoC challenges researchers to characterize brain–behavior relationships using multiple units of analysis. Moving forward, the field is in need of advanced measures that can be integrated to understand the biology underlying psychopathology that links behavior all the way to cellular and molecular functioning.
Our work focuses on developing tools to objectively characterize OCD behavior using video recording and to cross-validate these behavioral markers with standard clinical measures. Computer vision is a means of acquiring, processing, analyzing, and understanding images and videos (Forsyth and Ponce 2011). A computer vision approach was used to acquire and process the videos in our study. To our knowledge, no published studies to date have used computerized video analysis to assist in identification and quantification of OCD behaviors in youths. However, virtual reality or computerized technology has been used to quantify the severity of OCD behaviors in adults. Virtual reality uses real-time computer graphics technology, sounds, and sensory input to create a computer-generated world in which users interact (Kim et al. 2009).
Kim et al. (2010) studied 30 adults with OCD and 27 healthy controls using a virtual reality-based behavioral task that was designed to elicit checking behavior, a common compulsion in OCD (Geller and Williams 2016). OCD participants compared with controls exhibited significantly greater frequency of checking behaviors and spent more time checking. In OCD, greater time spent checking was positively correlated with higher scores on the Yale-Brown Obsessive Compulsive Scale (Goodman et al. 1989). Subsequently, the same research team evaluated 35 healthy college students as they participated in a computer-simulated arranging task (Roh et al. 2013). There were significant positive correlations between time spent arranging objects and OCD symptom severity and between frequency of manipulations of objects and symptom severity.
The primary aim of this multidisciplinary pilot study was to identify and quantify behavioral markers in youths with OCD compared with healthy controls. We developed an experimental paradigm that used video analysis to capture behaviors while children completed several tasks that involved interaction with the environment (e.g., arranging objects, hand washing). Videos were coded manually for OCD-related behaviors. To validate the relevance of the behavioral markers for OCD psychopathology, we compared these measures between children with OCD and healthy controls, and examined the relationships between behavioral markers and dimensional scores on the CY-BOCS and other clinical scales. In addition, since research in the area of autism spectrum disorders suggests that physical environmental factors (e.g., color, sound, seating arrangement) may influence the behavior of children (Schilling and Schwartz 2004; Mostafa 2008), we began investigating the role of the physical environment in increasing or decreasing compulsions in youths with OCD.
We hypothesized that observable behavioral markers in youth with OCD (e.g., spending a long time on arranging tasks or hand washing task; repetitive behaviors during tasks) would distinguish them from matched healthy controls. We also hypothesized that video measures of behavior would correlate with clinical measures (i.e., youths with higher scores on video measures of OCD behavior would show greater severity on clinical measures of OCD). Confirmation of these hypotheses would validate the use of video measures of OCD behavior as an objective tool for studying OCD, and would suggest behavioral markers that could be used in future research to integrate with other units of analysis (e.g., measures of brain circuitry, physiology, genetics, and cellular and molecular functioning). Furthermore, it was hypothesized that the physical environment would influence severity of OCD behaviors (i.e., engaging in a task on a patterned carpet compared with on a plain carpet would be associated with greater severity and increased frequency of compulsions in the OCD group).
Methods
Participants
Experiments were conducted with 18 youths with OCD and 21 matched healthy controls, ages 5–17. Mean age was 11.5 (SD = 3.2) years for OCD participants and 10.7 (SD = 3.3) years for controls. There were no significant differences between groups on age, gender, or ethnicity (Table 1). Children with OCD had a mean CY-BOCS score of 21.8 (SD = 10.3) (moderate severity) with range of 0 to 37. Seventy-eight percent of children with OCD were receiving psychotropic medications and 61% were receiving therapy for OCD (Table 1).
COIS-R not obtained in controls.
Scale scores that are significantly different between groups are included.
BASC-2, Behavioral Assessment System for Children, Second Edition; COIS-R, Child Obsessive–Compulsive Impact Scale-Revised; CY-BOCS, Children's Yale-Brown Obsessive Compulsive Scale; MASC-2, Multidimensional Anxiety Scale for Children-2; OCD, obsessive–compulsive disorder.
Procedure
The study was approved by the University of Minnesota Institutional Review Board. Participants were recruited by referral from child and adolescent psychiatrists, flyers in the Psychiatry Clinic and community, and Craig's List. After obtaining written informed consent from parents and written assent from children, the project coordinator administered the CY-BOCS to child and parent together. Parents completed the Child Obsessive–Compulsive Impact Scale-Revised (COIS-R) (Piacentini et al. 2007) and Behavioral Assessment System for Children, Second Edition (BASC-2) (Reynolds and Kamphaus 2010), and children completed the COIS-R and Multidimensional Anxiety Scale for Children-2 (MASC-2) (March 2013). Structured diagnostic interviews were not administered to subjects as part of this pilot study. The majority of OCD participants (n = 14, 78%) had previously been evaluated in the Child and Adolescent Anxiety Disorders Clinic and thus had been diagnosed with OCD as part of an outpatient evaluation. A small number (n = 3, 17%) had participated in another OCD research study and had been diagnosed with OCD based on the Anxiety Disorders Interview Schedule for DSM-IV, Child Version (Silverman and Albano 1996) as part of that study. Only one OCD subject (5%) was recruited via an advertisement. That subject did not have a psychiatric evaluation or diagnostic interview, but phone screen strongly suggested OCD and the CY-BOCS was 21 (moderate severity). Participants completed three video-recorded tasks designed by the research team (described below). Subjects were compensated with a $10 gift card for participation.
Measures
CY-BOCS: CY-BOCS is a 10-item, clinician-rated, semistructured instrument to measure severity of obsessions and compulsions. Psychometric properties are adequate (Storch et al. 2006; Yucelen et al. 2006). Interrater reliability data were collected in our sample. The measures of interrater reliability were based on four CY-BOCS interviews that were administered by the project coordinator with one or two trained members of the research team simultaneously rating the CY-BOCS interviews. Intraclass correlation coefficient for the CY-BOCS Obsessions score was 0.89, for the Compulsions score was 1.00, and for the Total score was 0.96. This indicates strong interrater reliability on the CY-BOCS. Dimensional scores were calculated based on number of current OCD symptoms on the CY-BOCS checklist (Bernstein et al. 2013). Contamination/cleaning dimension score included CY-BOCS items from the following categories: contamination obsessions, somatic obsessions, and cleaning compulsions. Ordering/repeating score comprised items from magical obsessions and checking, repeating, counting, and ordering compulsions. Hoarding score included hoarding obsessions and compulsions. Forbidden thoughts score comprised aggressive, sexual, and religious obsessions.
COIS-R: Parent Version and Child Versions measure functional impairment in daily life due to OCD and have good psychometric properties (Piacentini et al. 2007). MASC-2: MASC-2 is a 50-item self-report measure for youths 8–18 years. It comprises anxiety subscales (e.g., obsessions and compulsions). The MASC has adequate test–retest reliability and high convergent and divergent validities (March et al. 1997). BASC-2: BASC-2 screens for emotional and behavioral symptoms and psychometric properties are very good (Reynolds and Kamphaus 2010).
Video analysis: Five GoPro cameras were placed above looking down and in front of participants to record their behavior during tasks. Each video was cropped in time to include only the activity of interest and to spatially center the child engaging in activity.
Task 1: Free arrangement: Participants were given a box of school supplies (e.g., markers, tape, and pencils) and instructed to arrange the objects on a table in any way they wanted. Task 2: Hand washing: Participants were asked to wash and dry their hands at a portable sink in the presence of a nonfunctioning toilet. Soap and towels were provided. Task 3: Arrangement on contrasting carpets: Subjects organized school supplies on a plain carpet and also on a bold patterned carpet matching the arrangement provided on a sample card. Order of task completion on a plain versus patterned carpet was randomly assigned.
Rating of videos
One research assistant from each discipline (i.e., child and adolescent psychiatry, design, engineering and computer science) watched the videos and rated them on behavioral variables (Table 2). Evaluators were blind to OCD versus control status. Consensus meetings were held among raters and a child and adolescent psychiatrist (G.A.B.) to compare scores. The majority of ratings were congruent among raters. In these cases, final scores were calculated by computing the mean score of raters. Video ratings with a substantial degree of discrepancy between raters (minority of the ratings) resulted in watching those videos as a group. After discrepancies in initial scores were resolved for those cases, mean scores were calculated.
Analyzed via computer vision tools (Fasching et al. 2016).
Data analysis
T-tests for continuous variables and chi-square tests for categorical variables compared OCD and control groups on demographics, video measures, and clinical measures. Using Pearson correlations, video measures were correlated with scores on clinical measures in the OCD group. Repeated-measures analyses of variance (ANOVAs) were conducted on data obtained in Task 3 using the plain and patterned carpets. Main effects of group (OCD vs. control) and order of presentation of carpet (plain carpet first vs. patterned carpet first), within-subject effect of carpet (plain vs. patterned carpet), two-way interaction effects of carpet × group and carpet × order, and three-way interaction of carpet × group × order were tested in the models. Alpha level of <0.05 (two tailed) was used for all analyses. Corrections for multiple comparisons were not applied due to the exploratory nature of the study.
Results
Severity of symptoms
Children with OCD compared with healthy controls scored significantly higher on measures of OCD (Table 1). In addition, OCD participants were rated by parents as significantly higher than controls on the following BASC-2 scales: anxiety, depression, somatization, atypicality, hyperactivity, aggression, and attention problems.
Free arrangement of objects
While there was no significant difference between OCD and control groups on time spent completing the free arrangement task, there was a larger standard deviation (SD) and range for the OCD group. Mean duration of task was 3.2 ± 3.5 minutes with range of 0.4–11.5 minutes for OCD participants and 2.0 ± 1.8 minutes with range of 0.6–7.3 minutes for control group. Similarly, mean number of moves of objects during the free arrangement task was not significantly different between groups, but the OCD participants showed a larger SD and range. Average number of moves was 40.8 ± 29.4 with range of 13.7–115 in OCD group and 33.2 ± 12.4 with range of 21.7–79.3 in control group.
In the OCD group, higher ordering/repeating dimension scores on the CY-BOCS and higher anxiety scale scores on the MASC-2 were associated with longer time spent arranging objects (Table 3). Higher CY-BOCS ordering/repeating dimension scores were also associated with more moves of the objects. On the contrary, higher scores on BASC-2 hyperactivity, attention problems, and aggression were associated with fewer moves. Youths with OCD compared with controls were significantly more likely to use a smaller amount of space in completing the free arrangement task [χ2 (df = 1, 25) = 3.90, p = 0.048] (Fig. 1).
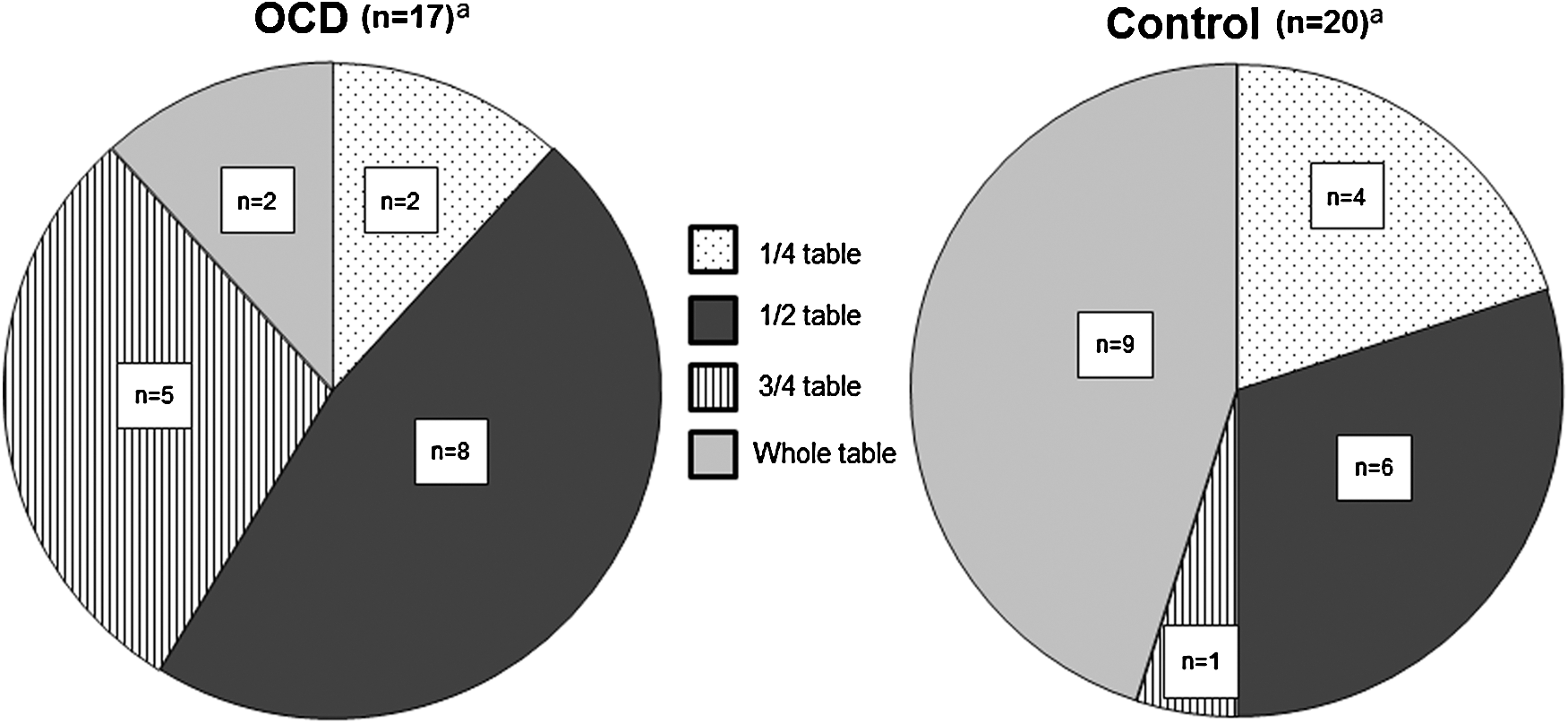
Amount of space used during free arrangement task. OCD group used less space for arrangement than control group (p = 0.048). aTwo participants (1 OCD, 1 control) excluded due to missing video data.
p < 0.05.
BASC-2, Behavior Assessment System for Children, Second Edition; CY-BOCS, Children's Yale-Brown Obsessive Compulsive Scale; COIS-R, Child Obsessive–Compulsive Impact Scale-Revised; FA, free arrangement; MASC-2, Multidimensional Anxiety Scale for Children-2.
Hand washing
OCD participants compared with controls were significantly more likely to exhibit “other” behaviors during hand washing (e.g., touching/tapping the sink, washing/drying the sink, drinking water, investigating the setup, rubbing the countertop) [χ2 (df = 1, 32) = 8.88, p = 0.003]. In OCD participants, longer duration of hand washing was positively correlated with greater severity on two CY-BOCS dimensions: ordering/repeating and forbidden thoughts. Longer duration of hand washing was also positively correlated with other measures of OCD severity (i.e., CY-BOCS total score, MASC-2 obsessions, and compulsions score), a measure of OCD functional impairment (COIS-R child score), and depression on BASC-2 (Table 3).
Arrangement of objects on plain versus patterned carpet
Repeated-measures ANOVAs showed no significant main effects or interactions on the dependent measures, including duration, number of times objects were moved, number of adjustments of objects, amount of space used, and number of times the subject checked the sample card. This indicated no significant effects of group, carpet pattern, order of carpet pattern presentation, and no significant interactions among these variables.
Since there were no differences in task performance based on whether participants were completing the task on plain or patterned carpet, data from the two conditions were combined and the mean scores were calculated for each participant. In the OCD group, correlations between video measures and clinical measures revealed that higher scores on the CY-BOCS ordering/repeating dimension were significantly associated with greater number of moves of objects and greater number of adjustments of objects (Table 4). In addition to significant findings on CY-BOCS dimensional scores, higher scores on general anxiety and OCD measures significantly correlated with behavioral measures (Table 4).
Mean score for performance of task on plain and patterned carpets.
Amount of space used during task.
p < 0.05.
p < 0.01.
BASC-2, Behavior Assessment System for Children, Second Edition; CY-BOCS, Children's Yale-Brown Obsessive Compulsive Scale; COIS-R, Child Obsessive–Compulsive Impact Scale-Revised; MASC-2, Multidimensional Anxiety Scale for Children-2.
Children with OCD who were rated by parents on BASC-2 as having greater severity of attention problems and greater conduct problems used significantly less space during the task (r = −0.48, p = 0.045, and r = −0.51, p = 0.045, respectively). A trend suggested that children with OCD who scored high on the CY-BOCS hoarding dimension used less space during the task (r = −0.46, p = 0.053). There were no significant correlations between severity scores on clinical measures and number of times the children with OCD checked the sample card during the task.
Discussion
We observed children with and without OCD while they completed everyday tasks in an experimental setting using video recording with the goal of identifying behavioral markers of illness that could be used to study OCD from a dimensional perspective. Analysis of the videos facilitated objective measurement of OCD-related behaviors (e.g., excessive hand washing and excessive arranging behaviors). Although there were few significant group differences on task performance, children with OCD showed greater within-group variability on behavioral measures. In the OCD group, these behavioral measures were significantly correlated with dimensional scores on the CY-BOCS. This supports the construct validity of video measures in quantifying dimensions of OCD. Our findings in children are consistent with those of Kim et al. (2010) and Roh et al. (2013) in adults, and confirm that observable behaviors in OCD are positively correlated with clinical measures of severity. This converging evidence is encouraging because it suggests that measurement of behavior as captured by video recording is a valid approach for measuring OCD psychopathology.
This complementary approach (measurement of behavioral markers on video) to traditional assessment could be used by RDoC researchers to examine psychopathology dimensionally. For example, researchers interested in understanding the biological underpinnings of the need for order and tendency to engage in repetitive compulsions (ordering/repeating symptoms) may select the free arrangement task and measure number of moves and duration, which were shown to be correlated with ordering/repeating, and integrate these measures with other units of analysis (e.g., assessment of brain circuitry implicated in this behavior, genetic markers) to allow for a deeper understanding of the biology underlying this domain of psychopathology. Advantages of video analysis include that it is objective rather than subjective and the data can be collected in nonclinical settings (e.g., home, school).
During hand washing, youth with OCD were significantly more likely than controls to exhibit “other” behaviors (p = 0.003) (e.g., cleaning or drying the sink, inspecting the sink, touching and tapping the sink, rubbing the countertop). Since this variable in our analysis was a collection of behaviors, rather than one narrow dimension, we view this interesting finding as a starting point rather than an end result. With a larger sample, we might be able to determine whether and how each of these individual behaviors relates to other aspects of OCD symptoms, behavior, and underlying biology. Without video recording, researchers and clinicians would not be able to glean this level of detail about behaviors associated with OCD. Furthermore, it illustrates how review of videos may help define additional behavioral markers and could add a new, complementary tool in the assessment of children with OCD.
In current standard practice, a comprehensive child psychiatric assessment includes psychiatric interviews with child and parents and measures of symptom severity, including self-report and clinician-administered ratings (King et al. 1998; Grabill et al. 2008). However, interviews and rating scales are unlikely to provide specific details about frequency, duration, types of compulsive behaviors, and associated behaviors due to retrospective reporting inherent with these measures (Kim et al. 2010). Furthermore, self- and clinician-reports are subject to several types of bias (e.g., expectancy bias). In addition, the video analytic approach described here could facilitate the identification of individualized target behaviors for tailored treatment, and these behavioral markers could be used to monitor treatment response.
Interestingly, children with OCD compared with healthy controls used significantly less space during the free arrangement task (p = 0.048). Perhaps youth with OCD compared with healthy controls are more cautious, constricted, and inhibited during activities. Their use of a small area of table during the free arrangement task may be related to a rigid style of thinking. Also, children may have been having obsessions that the table was dirty or contaminated. A common symptom of pediatric OCD is contamination obsessions, which are associated with excessive hand washing and avoidance of “contaminated objects” (Swedo et al. 1989).
There was a trend that youth with OCD who score high on the CY-BOCS hoarding dimension used less space when arranging objects on contrasting carpets (r = −0.046, p = 0.053). This might be explained by rigidity in problem solving or obsessional thoughts about wanting to hoard the objects and therefore keeping them in a small area. Hoarding has distinct clinical characteristics and is a separate disorder in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) (American Psychiatric Association 2013), no longer subsumed under OCD as in Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV-TR) (American Psychiatric Association 2000). Hoarding in youths is associated with lack of insight (Storch et al. 2007), pathological doubt on CY-BOCS (Mataix-Cols et al. 2008), ADHD (Sheppard et al. 2010), elevated depression (Mataix-Cols et al. 2008), and poor response to both cognitive-behavioral therapy and pharmacological interventions (Leckman and Bloch 2008). Hoarders are less likely to present to clinics for treatment. Thus, behaviors that assist in identifying children with hoarding behavior are important.
Analyses of videos also identified correlates with domains involving attention deficit and disruptive behavior; children with symptoms in these areas could represent an important subgroup of children with OCD. A review of studies showed that ∼26% (range of 3%–57%) of children with OCD meet criteria for a disruptive behavior disorder (Geller and Williams 2016). Children who were rated by their parents on BASC-2 as having problems with attention and conduct used less space while arranging objects on contrasting carpets. Children who are inattentive and hyperactive/impulsive often complete tasks quickly and without paying attention to detail. This may explain their use of a small area of the table. Similarly, children who were rated on BASC-2 as more hyperactive, aggressive, and inattentive completed the free arrangement task with significantly fewer moves of objects.
Another focus of our multidisciplinary research is to understand how elements of the physical environment may affect OCD behaviors. Multidisciplinary research in autism has illustrated the importance of considering interactions with the physical environment in understanding psychopathology. Researchers have explored aspects of physical environments and how they affect behavior in autistic children (Schilling and Schwartz 2004; Mostafa 2008). We found no difference between the behavior of OCD and control subjects during an arranging task based on whether they performed the task on a plain versus patterned carpet. Thus, our hypothesis that children with OCD would be “triggered” to engage in a greater frequency of compulsive behaviors when completing a task on a bold patterned carpet compared with on a mundane, monochromatic carpet was not supported. Other environmental factors may trigger or diminish compulsions in youths with OCD. Variables to explore in future studies include sound, lighting, spatial layout of the room, and setting (home, school, or laboratory).
Strengths of the study include the innovative study design developed by researchers in child and adolescent psychiatry, design, and computer and electrical engineering and the use of behavioral biomarkers to study OCD from a dimensional perspective. In addition, the range of CY-BOCS scores for OCD participants was 0 to 37 indicating a wide range of symptom severity. Some of the participants with OCD were in full remission and others were in severe exacerbation. Participants with all levels of severity were included, which makes the findings more generalizable to the entire population of youths with OCD symptoms.
Limitations of this investigation include the small sample size and large number of exploratory tests that were conducted without statistical correction for multiple comparisons. In addition, structured diagnostic interviews were not administered to confirm the diagnosis of OCD and to document the absence of psychiatric diagnoses in controls. Therefore, our findings should be viewed as preliminary to guide future investigations.
Future directions may include concurrent monitoring of physiological parameters such as heart rate, blood pressure, and skin conductance (Kim et al. 2009) and recording obsessional thoughts as they occur in real time with handheld computers (Herman and Koran 1998) while video recording behaviors. This would help define relationships between behavior, physiological responses, and children's obsessions. Furthermore, we are currently exploring the use of computer vision tools to automatically identify and quantify OCD behaviors in our videos (Fasching et al. 2016) and developing a computer-assisted virtual environment to facilitate assessment and treatment of youths with OCD.
Conclusions
Measurement of behavior using video recording appears to be a valid approach for quantifying OCD symptomatology. This methodology could serve as a new tool for investigation of OCD from a dimensional perspective. This objective, novel behavioral measurement technique may benefit both researchers and clinicians in the evaluation of children with OCD and serve as a complementary approach to traditional psychiatric behavioral assessment.
Clinical Significance
Computer vision tools may be used in the future to screen and identify children at-risk for OCD. For example, Go-Pro cameras could be placed in homes or schools to record children's hand washing behavior or sorting/organizing behaviors to assist in the identification of children with OCD or children who are at-risk for OCD. This approach could facilitate early identification and also guide individualized treatment of OCD and other mental health conditions.
Footnotes
Acknowledgments
The authors extend special thanks to the children and their parents who participated in the study. Parts of this article were presented at the Environmental Design Research Association Conference in Los Angeles, May 2015, and at the 62nd Annual Meeting of the American Academy of Child and Adolescent Psychiatry in San Antonio, October 2015.
Disclosures
Dr. Bernstein has received research support from the National Institute of Mental Health, National Science Foundation, and F. Hoffman-La Roche. Dr. Hadjiyanni has received research support from the National Science Foundation, University of Minnesota College of Design Agricultural Experiment Station, University of Minnesota IDEA Multicultural Research Award, University of Minnesota Imagine Fund, University of Minnesota Extension and College of Design Minnesota Housing Policy Tool Box, University of Minnesota College of Design DHA Research Investment, and University of Minnesota Grant-in-Aid. Dr. Cullen has received research funding from the National Institute of Mental Health, Marriott Foundation Award in Individualized Medicine Disease Risk Initiative, Ontario Mental Health Foundation of the University of Toronto, MNDrive Brain Conditions Innovations of the University of Minnesota/Minnesota Legislature, University of Minnesota Center for Translational Science Institute, University of Minnesota Academic Health Center Faculty Research Development Grant, Minnesota Medical Foundation, and University of Minnesota Medical School Dean's Office. Dr. Robinson has received research support from the National Science Foundation. Ms. Harris, Mr. Young, Mr. Fasching, and Mr. Walczak report no funding support. Dr. Lee has received research support from the National Institute on Drug Abuse, National Institute of Mental Health, and Conrad N Hilton Foundation. Dr. Morellas and Dr. Papanikolopoulos have received research support from the National Science Foundation and Federal Highway Administration/Minnesota Department of Transportation. Dr. Bernstein is the only author with research support from a pharmaceutical company (i.e., Hoffman-La Roche). All authors have no other financial relationships with any pharmaceutical company. All authors report no biomedical financial interests or potential conflicts of interest.