
Abstract
Objectives:
The goal of this study was to estimate the association between use of second generation antipsychotics (SGAs) and type 2 diabetes (T2DM) among commercially insured children and young adults 6–24 years compared to users of non-SGA psychotropic medications.
Methods:
Using the Truven MarketScan Commercial Claims and Encounters Database, new users of SGA and non-SGA psychotropic medications (anxiolytics, antidepressants, hypnotics, and mood stabilizers) between July 1, 2009 and December 31, 2013 who were 6–24 years of age and had continuous coverage ≥180 days before their index date (i.e., date of first fill of SGA or non-SGA psychotic) were identified. SGA users were propensity score (PS) matched to non-SGA psychotropic users at a 1:1 ratio. Individuals were followed until diabetes diagnosis, discontinuation or switch from index medication, end of continuous coverage, or end of the study period. The Cox proportional hazards model was used to estimate the hazard ratio (HR) for incident T2DM for SGA users compared to non-SGA users.
Results:
A total of 45,289 SGA users and 932,336 non-SGA psychotropic users met inclusion criteria. In the PS matched sample, there were 102,028 patient-years of follow-up and median time to event was 202 days for SGA users (n = 43,407) and 290 days for non-SGA psychotropic users (n = 43,407). A total of 141 SGA users (33 cases per 10,000 patient-years) and 110 of the non-SGA psychotropic users (18 cases per 10,000 patient-years) developed T2DM. The SGA users had a 1.7 times higher risk of T2DM (HR 1.71, 95% confidence intervals [CI] 1.33–2.20) compared to non-SGA psychotropic users.
Conclusion:
Risk of T2DM should be considered when evaluating the risk/benefit of SGA use among children and young adults. Future studies aimed at evaluating risk factors, diabetes prevention strategies, and effective management of the long-term consequences of T2DM in this vulnerable population are needed.
Introduction
T
A 2016 meta-analysis reported a pooled 1.79 and 3.02 times higher risk of developing T2DM when comparing antipsychotic-exposed youths to psychiatric controls and healthy controls, respectively; however, there is significant heterogeneity among the included studies with respect to methodology, comparator groups, and study population (Galling et al. 2016). Seven U.S. studies using data from 1996 to 2009 reported results ranging from no increased risk to over a fourfold increased risk (incidence rate ratio [IRR] 0.987–4.25) (Galling et al. 2016). Four studies were conducted among Medicaid-insured children (McIntyre and Jerrell 2008; Morrato et al. 2010; Bobo et al. 2013; Rubin et al. 2015) who are more likely to use antipsychotics and have a higher prevalence of diabetes (type 1 diabetes [T1DM] or T2DM) and mental health conditions (Crystal et al. 2009; Bethell et al. 2011).
The other three studies were conducted among commercially-insured youths: one found a nonstatistically significant increase in risk of T1DM or T2DM when comparing SGA users to antidepressant users (IRR 3.58, 95% CI 0.92–20.30) (Andrade et al. 2011); one compared FGA or SGA use versus no antipsychotic use (nonactive comparator group) among adolescents with bipolar disorder or schizophrenia and risk of T1DM or T2DM (hazard ratio [HR] 1.76, 95% CI 1.15–2.72) (Enger et al. 2013); and the last compared SGA users to a healthy nonactive comparator group (HR 2.18, 95% CI 1.45–3.29) (Sohn et al. 2015).
To extend current knowledge, this study evaluated whether U.S. commercially insured children and young adults 6–24 years old who initiate SGAs have an increased risk of new-onset T2DM compared to those who initiate non-SGA psychotropic medications (antidepressants, anxiolytics, hypnotics, and mood stabilizers). We hypothesized a priori that SGA initiators are at higher risk of developing T2DM.
Methods
Data source
This study used the Truven MarketScan® Commercial Claims and Encounters (CCAE) Database, which contains patient-level clinical utilization and enrollment information across inpatient, outpatient, and prescription claims obtained from a selection of employer-sponsored commercial plans in the United States from January 1, 2009 to December 31, 2013 (Hansen and Chang 2011). The eligibility file provides demographic information about each patient, including age, gender, type of health plan, U.S. census geographic location, as well as enrollment dates.
The outpatient database includes encounters rendered in a doctor's office, hospital outpatient facility, emergency room, or other outpatient facility and includes International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9CM) codes, current procedural terminology (CPT) codes, and dates of service. The inpatient claims database includes service records derived from Uniform Billing form and also contain ICD-9CM, CPT codes, and hospital admission and discharge dates. The pharmacy claims database provides the National Drug Code (NDC) of drugs dispensed, date dispensed, co-pay, quantity, and days' supply. The University of Illinois at Chicago Institutional Review Board determined this study as exempt from human subjects research review.
Study design and study population
This was a propensity score (PS) matched retrospective cohort study that used a new-user design. Children and young adults 6–24 years of age who filled a new prescription for a SGA (aripiprazole, asenapine, iloperidone, lurasidone, olanzapine, paliperidone, quetiapine, risperidone, or ziprasidone) or non-SGA psychotropic (antidepressant, anxiolytic, hypnotic, or mood stabilizer) between July 1, 2009 and December 30, 2013 and who had continuous medical and pharmacy insurance coverage for at least 180 days before initial SGA or initial non-SGA psychotropic were eligible for inclusion (Supplementary Table S1; Supplementary Data are available online at
The date of the first prescription dispensed for one of the study medications was defined as the index date. The 180-day baseline period was used to assess patients' medical and treatment history before SGA or non-SGA psychotropic initiation. To ensure a new user cohort, those with any prescription for a SGA, non-SGA psychotropic, or clozapine during the baseline period were excluded. Given that FGAs may also increase the risk of diabetes and is not the focus of this study, patients on these drugs at baseline were also excluded. In addition, we excluded those who initiated both a SGA and non-SGA psychotropic on the same day. To ensure that patients did not have preexisting diabetes, those with a history of T1DM or T2DM or any antidiabetic medication use within the 180 days before cohort entry were excluded.
Given that acromegaly, Cushing's syndrome, and polycystic ovary syndrome (PCOS) were risk factors for diabetes or diabetes drug use, those with a diagnosis for these conditions at baseline were excluded. We also excluded patients who were pregnant since gestational diabetes is a different topic of study. As chronic steroid use is a risk factor for diabetes, patients with at least 28 days of oral or intravenous steroid use within the 60 days before cohort entry were also excluded (Supplementary Table S2). We did not require a mental health diagnosis for study entry in our primary analysis as this may exclude many patients using SGAs for off-label indications that may not be documented in medical claims. In sensitivity analysis, we excluded patients without a mental health diagnosis at baseline.
Follow-up and censoring
Individuals were followed from the day after their index date until the earliest occurrence of: (1) discontinuation of index prescription (60-day medication gap), (2) switch or addition of a medication from the alternative exposure drug class, (3) initiation of a FGA, (4) development of diabetes, (5) end of the study period, or (6) insurance coverage termination. Therefore, the at risk period for a SGA initiator started the day after the first SGA prescription fill and ended when the first of the following occurred: diabetes developed, 60 days after the end of the supply of SGA medications, filled a non-SGA psychotropic or a FGA, lost insurance coverage, or on December 31, 2013.
This risk window was chosen because current evidence suggests that the impact of SGAs on glycemic control is highest during early therapy (as early as 4 days) and may be attenuated or potentially reversible upon drug discontinuation (Jin et al. 2002; Lipscombe et al. 2009, 2011; Guenette et al. 2013; Calarge et al. 2014). Patients were allowed to switch within exposure groups (e.g., aripiprazole to quetiapine, or fluoxetine to buspirone) but not across exposure groups (e.g., exposure ended for a SGA user if an anxiolytic was added) during follow-up. We censored patients who switched from one exposure group to the other exposure group as it would be difficult to determine whether risk of T2DM was associated with current drug or due to residual effects from the previous drug.
Outcome definition
Patients were deemed to have met the case definition of T2DM if they met either of the following criteria: (1) at least two inpatient or outpatient T2DM diagnosis codes identified by ICD-9-CM codes 250.x0 or 250.x2 within a 120-day period on separate days or (2) at least one drug claim for a noninsulin antidiabetic medication (metformin, sulfonylureas, thiazolidinediones, alpha-glucosidase inhibitors, meglitinide analogs, amylin analogs, glucagon-like peptide-1 agonists, and dipeptidyl peptidase-4 inhibitors and combinations).
We conducted four sensitivity analyses to test the robustness of results. First, we used Sohn and colleagues' case definition for T2DM: a hospital discharge with a primary diagnosis code for T2DM (ICD-9CM codes 250, 250.0, 250.1, 250.2, 250.3, or 250.9) or a combination of at least two diabetes-related medical and/or pharmacy claims, and when only prescription claims indicated diabetes, those with an insulin prescription with no prescriptions for oral antidiabetic medication were excluded.
Second, females who had a diagnosis code for PCOS (ICD-9-CM 256.4) and a metformin drug claim but no diagnosis code for T2DM were deemed to not have met the case definition for T2DM, since metformin may also be used to treat PCOS (Legro et al. 2013; Goodman et al. 2015). Third, patients with a drug claim for metformin but no corresponding inpatient or outpatient T2DM diagnosis were assumed not to have met the definition of having T2DM. Fourth, we restricted the sample to patients who had a mental health diagnosis during the 180-day period before cohort drug initiation.
Demographic and clinical characteristics
Baseline patient demographics were determined using information from index prescription and enrollment files. Mental health related diagnoses, amphetamine drug use, cardiovascular-related diagnoses and medication use, oral or intravenous corticosteroid use, glucose and lipid screening, as well as frequency of mental health and nonmental health related resource use, were determined during the 180-day period before index prescription. The Agency for Healthcare Research and Quality Clinical Classifications Software ICD-9-CM (Agency for Healthcare Research and Quality Healthcare Cost and Utilization Project 2014) codes were used to identify diagnoses, and NDCs (RED BOOK 2013) were used to identify prescription medications.
Statistical analyses
To address the potential for selection bias and confounding, SGA-initiators were matched to non-SGA psychotropic initiators by their PS, which is the predicted probability of receiving treatment conditional on observed patient characteristics (Austin 2011). SGA initiators were matched to non-SGA psychotropic initiators in a 1:1 ratio using a 1 to 8 digit greedy matching algorithm without replacement (Parsons 2004; Austin 2011). This matching algorithm matches individual patients from the SGA initiators to the comparison group on PS beginning at eight significant digits and moving to fewer significant digits until a match for the patient is identified and the process is repeated for each patient in the SGA initiators group. This method is intended to balance the two groups on the measured baseline characteristics.
The PSs were estimated using a nonparsimonious multivariable logistic regression model where all potential confounders and covariates related to the outcome were included based upon literature review and empirical selection (Supplementary Table S3) (Brookhart et al. 2006). Balance of the match was evaluated by visualizing the PS distributions before and after matching by exposure group, as well as using absolute standardized differences (ASD), which compares the difference in means between groups over the pooled standard deviation (Austin 2009, 2011). ASD are commonly used to assess balance of individual covariates before and after PS matching and by convention, ASD <0.1 represent good balance between groups (Austin 2009, 2011).
The Kaplan–Meier method and the log-rank test were used to estimate and compare the cumulative incidence of developing T2DM among the SGA-initiator and non-SGA psychotropic initiator groups. The Cox proportional hazards regression model was used to compare the HR of incident T2DM among the two cohorts. The proportional hazards assumption was evaluated using Schoenfeld residuals plotted over time, as well as modeling exposure to SGA as a time-varying covariate. Statistical analyses were conducted using SAS Version 9.4, Cary, NC, and figures were created using STATA Version 14 (College Station, TX).
Results
Baseline characteristics of patients before PS matching
A total of 45,289 SGA users and 932,336 non-SGA psychotropic users met inclusion criteria before PS matching (Fig. 1). Compared to non-SGA psychotropic users, SGA initiators were younger, more likely to be male, and had higher prevalence of cardiovascular drug use, attention-deficit/hyperactivity disorder diagnoses and amphetamine drug use, bipolar disorder, schizophrenia-spectrum disorders, developmental disorder, learning disorder, tic disorder, conduct disorder, impulse disorder, alcohol and substance abuse disorders, and suicide related diagnoses. SGA initiators also had more frequent mental health related hospitalizations and outpatient visits (Table 1).
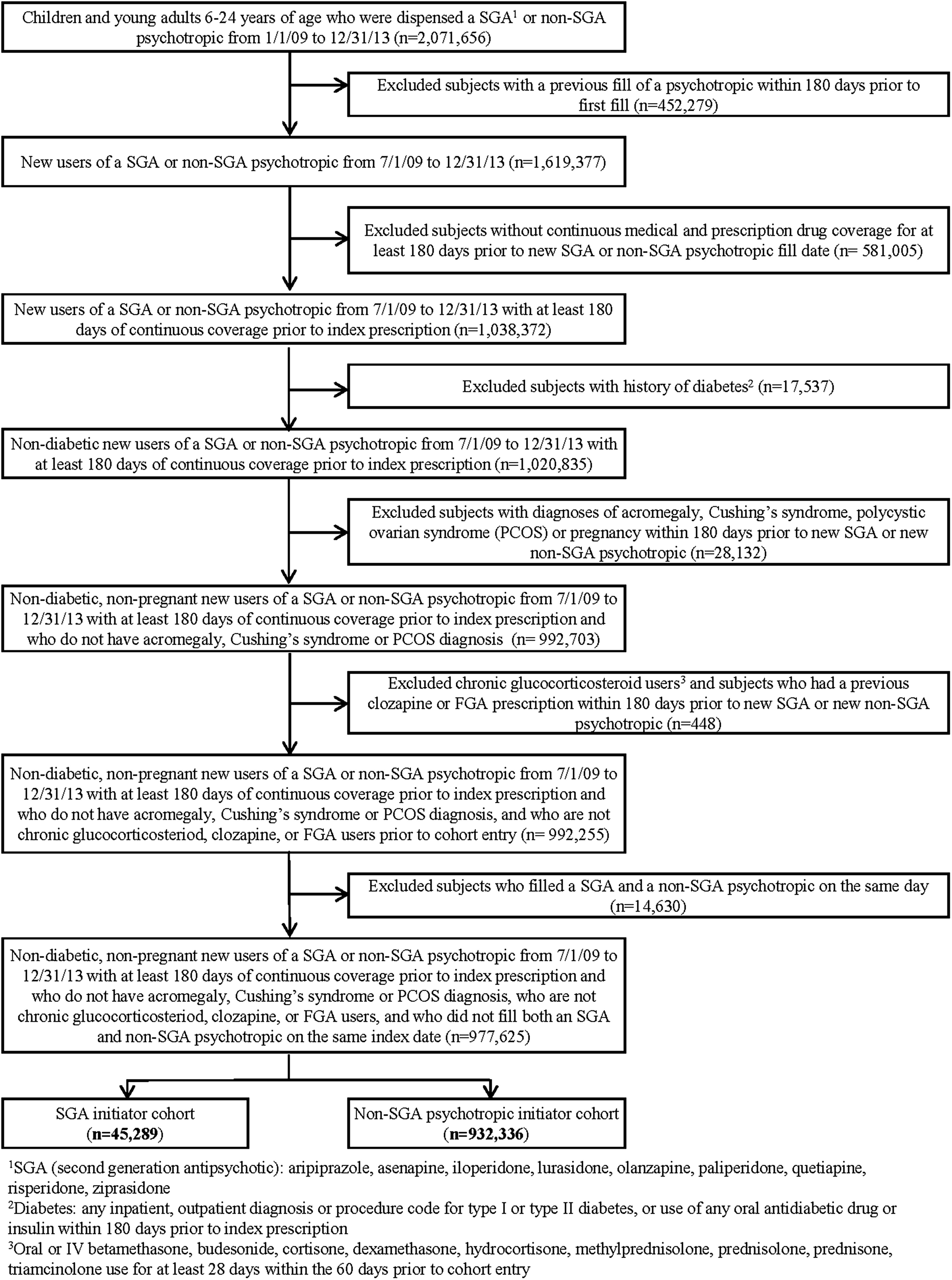
Identification of cohort by inclusion and exclusion criteria. Of the 2,071,656 patients who received either a SGA or a non-SGA psychotropic (anxiolytics, antidepressants, hypnotics, and mood stabilizers), 977,625 patients met inclusion and exclusion criteria before propensity score matching. Of those, 45,289 were SGA initiators, while 932,336 were non-SGA psychotropic initiators. SGA, second generation antipsychotic.
Propensity score based on baseline covariates within the 180 days before date of first dispense of SGA or non-SGA psychotropic.
Absolute standardized difference (SD) ≥0.10 indicates imbalance (*indicates SD ≥0.10).
Includes anxiolytics, hypnotics, antidepressants, and mood stabilizers.
U.S. Region per regional divisions by the U.S. Census Bureau (
Other = comprehensive (1.5%), consumer driven (5.8%), exclusive provider organization (1.2%), high deductible (4.4%), and point of service (6.21%) and point of service with capitation (0.7%) insurance plans.
Cardiovascular drugs include alpha antagonists (α-blocker), beta blockers (BB), calcium channel blockers (CCB), angiotensin converting enzyme inhibitors (ACE inhibitors), and angiotensin receptor blockers (ARB).
ADHD, attention-deficit/hyperactivity disorder; HbA1C, hemoglobin A1C; SD, standard deviation; SGA, second generation antipsychotic.
Baseline characteristics of patients after PS matching
A total of 43,407 SGA initiators (95.8% of original SGA initiator sample) were matched to 43,407 non-SGA psychotropic initiators, totaling 102,028 patient-years of follow-up. The non-SGA cohort had longer total follow-up time compared to the SGA cohort (59,540 and 42,488 patient-years, respectively), and median follow-up time was 384 and 223 days, respectively. Figure 2a and b shows the distribution of PS before and after matching. Post-match, the ASD for all covariates were smaller than 0.1, indicating that there was good balance after matching (Table 1).
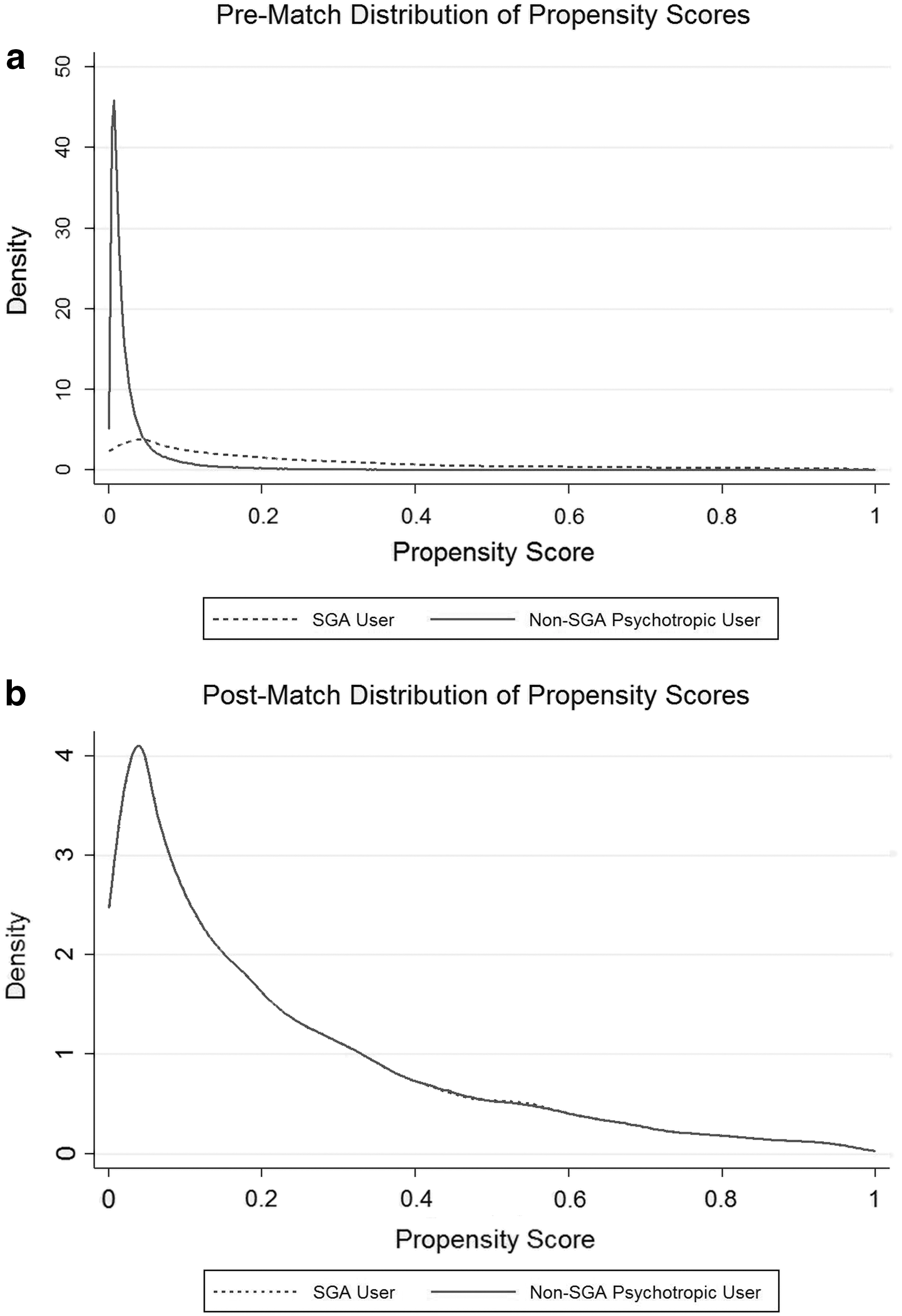
Propensity score distributions before and after matching.
Risk of T2DM
A total of 141 SGA initiators (33 cases per 10,000 patient-years) and 110 of the non-SGA psychotropic initiators (18 cases per 10,000 patient-years) met the case definition for T2DM. The median time to T2DM diagnosis was 202 days for SGA initiators (interquartile range [IQR] 358, first event at 3 days of follow-up) and 290 days for non-SGA psychotropic initiators (IQR 511, first event at 1 day of follow-up) (p = 0.002). SGA initiators had a 1.7 times higher hazard of developing T2DM compared to non-SGA psychotropic users (HR 1.71, 95% CI 1.33–2.20) (Table 2 and Fig. 3).
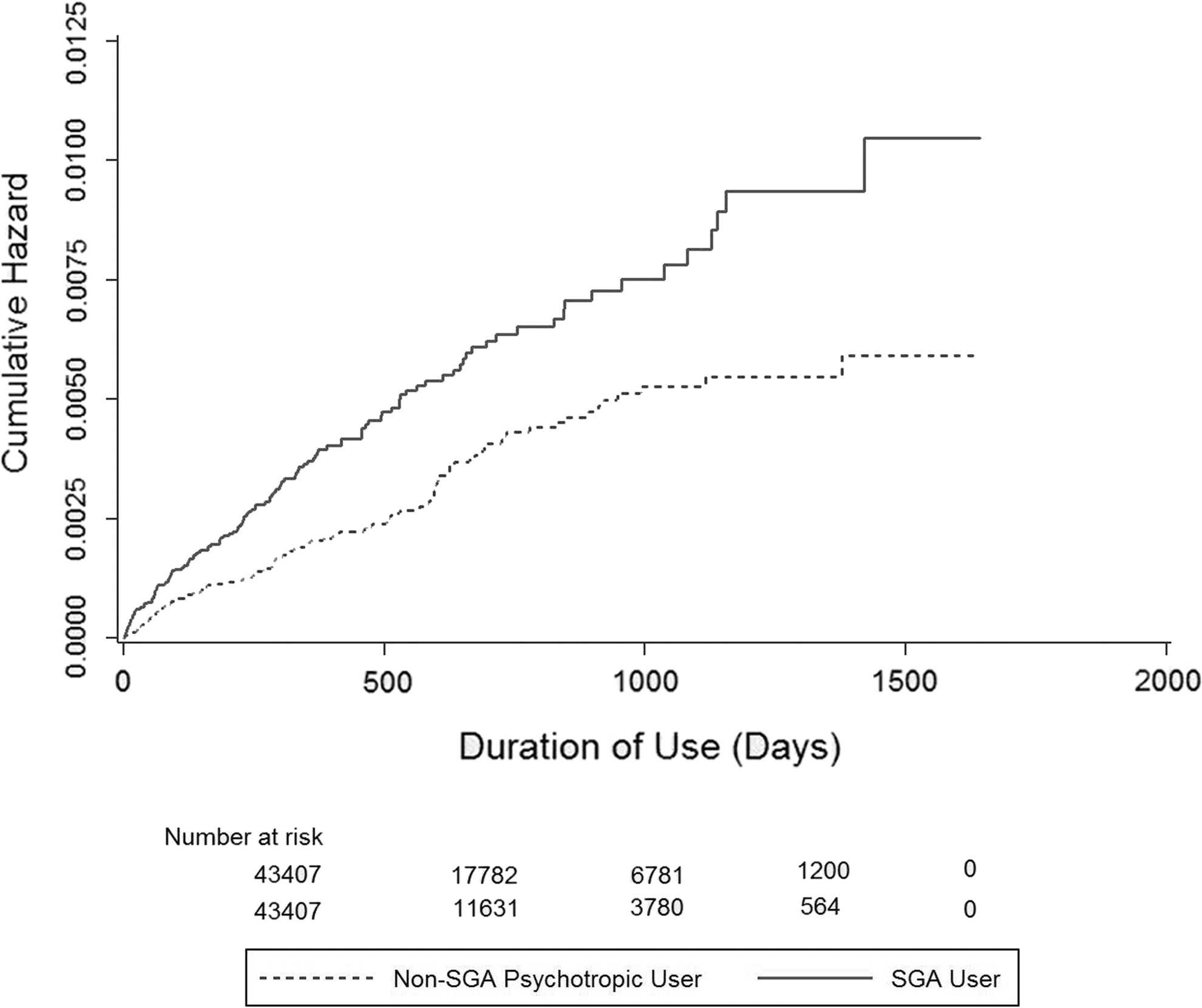
Cumulative incidence of type 2 diabetes mellitus comparing second generation antipsychotic (SGA) initiators versus non-SGA psychotropic initiators after propensity score matching.
T2DM defined as (1) at least two inpatient or outpatient T2DM diagnoses identified by International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes 250.x0 or 250.x2 within a 120-day period on separate days, or (2) drug claim for a noninsulin antidiabetic medication.
T2DM defined as (1) a hospital discharge with a primary diagnosis code for T2DM identified by ICD-9CM codes 250, 250.0, 250.1, 250.2, 250.3, or 250.9 or (2) a combination of at least two diabetes-related medical and/or pharmacy claims and (3) when only prescription claims indicated diabetes, those with an insulin prescription with no oral diabetes prescriptions were excluded.
T2DM defined as above in primary analysis with the additional criteria that patients with a drug claim for metformin and a ICD-9 code for polycystic ovary syndrome but no T2DM diagnosis were excluded.
T2DM defined as above in primary analysis with the additional criteria that patients with metformin drug claims but no corresponding ICD-9 code for T2DM diagnosis (250.x0 or 250.x2) were excluded.
Excluded patients without a mental health diagnosis during the preindex period. This analysis is restricted to 39,079 patients in the SGA initiator group (90.0% of the original 43,407 patients in the propensity-matched SGA initiator group) and 37,972 patients in the non-SGA initiator group (87.5% of the original 43,407 patients in the propensity-matched non-SGA initiator group).
SGA, second generation antipsychotic; T2DM, type 2 diabetes.
In sensitivity analysis using Sohn et al.'s case definition for T2DM, SGA initiators had 1.4 times higher hazard for T2DM compared to non-SGA psychotropic initiators (HR 1.43, 95% CI 1.05–1.94). In the second sensitivity analysis, when the case definition for T2DM was modified to exclude patients with a PCOS diagnosis (11 in the SGA initiator group and 33 in the non-SGA psychotropic initiator group), the HR was 2.24 (95% CI 1.69–2.97) for SGA initiators compared to non-SGA initiators. In a third sensitivity analysis, when patients with metformin but no corresponding inpatient or outpatient T2DM claim were excluded (98 SGA initiators and 70 non-SGA initiators), the HR was 1.44 (0.93–2.22). Finally, when we restricted the population to only patients who had a mental health diagnosis at baseline, the HR was 1.64 (1.25–2.14).
Discussion
This study found that among commercially insured children and young adults 6–24 years of age, new SGA users had a 1.7 times higher hazard for developing T2DM compared to new users of non-SGA psychotropics. Importantly, the median time to event was less than 1 year. These results are directionally consistent with most other studies that have investigated the risk of T2DM among young SGA users and very similar to the results of the recent meta-analysis (Galling et al. 2016). Some of the interstudy heterogeneity of risk may be explained by differences in study population, sample size, and comparison group.
For instance, Bobo and colleagues' study reported a three times higher risk of T2DM comparing FGA and SGA users to non-SGA psychotropic users among Medicaid-insured children 6–24 years (Bobo et al. 2013). Unlike their study, we did not compare SGA users to patients taking psychostimulants since stimulants have been associated with weight loss and may artificially inflate the risk of diabetes among SGA users (Vanina et al. 2002). Instead, we adjusted for stimulant use in both groups. The HR from our study was similar to the results from Rubin's study, which found a 1.5 times higher risk of T2DM among Medicaid children 10–18 years old initiating SGA compared to non-SGA initiators; however, their study used an intent-to-treat analysis that also allowed patients to reenter the cohort in a sequence of nonrandomized trials (Rubin et al. 2015). In contrast, follow-up ended in our study when a patient switched from a SGA to a non-SGA psychotropic.
Among commercially insured children, Sohn et al. found a 2.2 times higher risk of T2DM when comparing children 4–18 years who were SGA users to a nonactive comparison group. In our analysis, the risk was lower (HR 1.43) when using Sohn and colleagues' definition (Sohn et al. 2015); however, our comparison cohort may have had a higher baseline risk of T2DM given that certain antidepressants and antimanic medications have also been associated with the risk of T2DM (Vanina et al. 2002). Andrade's study among commercially insured children 5–18 years also found a numerically but nonsignificantly higher risk of diabetes when comparing SGA initiators to PS matched antidepressant users (IRR 3.58, 95% CI 0.92–20.30) (Andrade et al. 2011).
These nonsignificant findings may be due to the lack of power owing to the smaller sample size (n = 8012 in each group) and shorter follow-up period compared to the present study. Enger and colleagues' study reported a 2.3 times higher risk of diabetes when comparing use of FGAs or SGAs to no treatment among patients with bipolar disorder or schizophrenia (HR 2.34; 95% CI 1.43–3.82) but only adjusted for gender, geographic region, and use of mood-stabilizing medications (Enger et al. 2013).
This is the most recent and largest study that evaluated the relationship between SGA use and the risk of diabetes among commercially insured population of children and young adults. In addition, we used an active comparator group since psychotropic users may be inherently different from nonpsychotropic users in ways that administrative data are unable to capture.
However, these results should be interpreted in the context of study limitations. First, insurance claims only serve as a proxy for actual diagnosis. Second, PS analysis only adjusts for measured confounding but does not account for unobserved confounding from variables that are not present in claims data (e.g., race, family history, smoking, and so on). Third, there is a potential for surveillance bias, where SGA initiators may be more likely screened for T2DM compared to non-SGA psychotropic initiators. However, metabolic screening rates are typically low among youths who initiate SGAs, and we matched patients on whether they had received a blood glucose or HbA1C test within the 90 days before drug initiation. Among commercially insured children 5–18 years, average metabolic screening rates within 6 months of initiating a SGA between 2003 and 2011 were 16% for glucose tests and 1.5% for HbA1C tests, with no significant differences pre- and postinitiation (Connolly et al. 2015).
Fourth, the follow-up duration for this study may not be long enough to adequately assess the risk of T2DM over longer term use of SGAs, although the highest risk period is thought to occur during the first 6–18 months of therapy with cases of diabetic ketoacidosis (DKA) reported within days of SGA initiation (Bobo et al. 2013; Guenette et al. 2013; Rubin et al. 2015; Sohn et al. 2015). In a review of 69 case reports of DKA associated with SGA use, two adolescents (12 and 16 years of age) developed DKA after approximately 6 months of SGA use (Guenette et al. 2013). The other case reports were among adults, where DKA occurred within 4 days to 4 years (median 9 months) of SGA treatment (Guenette et al. 2013). Given that patients were censored when they switched or added a medication from the alternative drug class (35.4% of SGA initiators and 14.8% of non-SGA psychotropic initiators), we were unable to evaluate the impact of SGA and non-SGA polypharmacy on risk of T2DM.
An important issue with administrative claims data is the potential misclassification of T2DM. Unlike Bobo's study (Bobo et al. 2013), we did not require both an oral diabetes medication and a diagnosis code to meet the case definition for T2DM, nor did we classify all insulin users as patients with T1DM since this algorithm has been criticized for resulting in too many false negatives (Samaras et al. 2014). According to the Search for Diabetes in Youth Study, 13.1% of youths 20 years and younger with T2DM were managed with lifestyle only, 33% used both insulin and an oral diabetes medication, 11% were on insulin-only regimens, and the rest were on metformin and/or other oral hypoglycemic agents (Badaru et al. 2013).
Pediatric T2DM treatment guidelines also recommend the use of insulin for T2DM when the distinction between T1DM and T2DM is unclear, which may be common upon first presentation (Copeland et al. 2013). Therefore, if we required that patients must have used an oral antihyperglycemic medication and must not have used insulin to meet the case definition of diabetes, it is likely that many patients with a true diagnosis of T2DM would have been misclassified as not having T2DM. In this case, if the magnitude and direction of misclassification were the same in both the SGA initiator and the non-SGA psychotropic initiator cohorts, the HR would be biased toward the null of no effect. In contrast, if lead time bias occurred and SGA initiators were more often screened for T2DM than non-SGA psychotropic initiators (surveillance bias), this would have led to differential misclassification where there is no way to predict the direction of the bias.
To address the possibility that some patients taking metformin may have been misclassified as having PCOS instead of T2DM (or both), we conducted a sensitivity analysis that resulted in a higher HR of 2.24. However, given that patients with PCOS diagnosis were excluded from cohort entry and that PCOS and T2DM share common risk factors (excess weight and hyperinsulinemia), by excluding these patients, we may inadvertently misclassify these patients as not having T2DM when they did but were just not given a diagnosis. In our primary analysis, we did not exclude patients with an insulin prescription fill but no oral antidiabetic prescription as in Sohn and colleagues' study (Sohn et al. 2015) since we were concerned that this definition may exclude patients with T2DM treated with insulin. Taking these factors into consideration, we elected to use a broader case definition with sensitivity analysis using Sohn's definition for comparability of results.
In a third sensitivity analysis, we assumed that patients who received metformin but had no corresponding inpatient or outpatient claim for T2DM did not have T2DM, since there is evidence for using metformin to treat SGA-associated weight gain (Klein et al. 2006). Of the 251 T2DM cases in our primary analysis, 181 (SGA = 105; non-SGA = 76) were identified using ≥2 metformin drug dispenses, meaning that these patients did not have at least two inpatient or outpatient claims for T2DM within 120 days on separate dates. Of these, 98/105 SGA initiators (93.3%) and 70/76 (92.1%) of non-SGA initiators had no corresponding inpatient or outpatient T2DM claim; thus the proportion of patients having metformin but no corresponding T2DM claim was similar between the two groups. The resulting HR was nonsignificant but still higher in the SGA group (HR = 1.44, 95% CI 0.93–2.22).
It is unclear from claims data whether these metformin patients actually had T2DM but were miscoded, were using metformin to prevent diabetes, or had preexisting T2DM. Since our objective was to compare the impact of SGA versus non-SGA therapies on the risk of T2DM regardless of indication, we did not restrict our primary analysis to patients with a mental health diagnosis but adjusted for indications at baseline through the use of PS matching. Therefore, patients may have been using psychotropic medications for nonpsychiatric indications. In sensitivity analysis when restricting analysis to patients with a mental health diagnoses, results were similar to our primary analysis (HR 1.64, 95% CI 1.25–2.14).
Our research has also led us to identify other critical areas of research for this vulnerable population of young people taking SGAs. First, the pathophysiology of SGAs' effect on hyperglycemia is not well understood. It is commonly thought that the risk of T2DM is entirely mediated by weight gain caused by SGAs; however, recent evidence suggests that SGA's effects on glucose metabolism and insulin dysregulation can occur in the absence of any weight gain (Scheen and De Hert 2007; Teff et al. 2013; Ebdrup et al. 2014; Raebel et al. 2014). In a recent meta-analysis of 69 cases of DKA, hyperosmolar coma, or death associated with SGA use, one-third of cases had no weight gain or even experienced weight loss (Guenette et al. 2013).
Second, blood glucose screenings among children who use SGAs are suboptimal and interventions to improve this are needed. In our study, 22.9% of SGA users in the unmatched sample had a blood glucose screening within 90 days before index prescription, which is improved in comparison to previous studies (Raebel et al. 2014; Connolly et al. 2015), but is still suboptimal. Third, the effect of earlier onset of T2DM in children is unknown. Based on adult studies, patients with early-onset T2DM (18–44 years) versus patients with normal onset T2DM (45 years and older) have a two times higher hazard of developing myocardial infarction (Hillier and Pedula 2003).
Conclusions
Risk of T2DM should be considered when evaluating the risk and benefits of SGA use among younger people. Future studies aimed at identifying patients at highest risk for developing T2DM and effective prevention strategies are much needed. In addition, studies should also evaluate how to effectively manage the long-term consequences of T2DM in this vulnerable population of children and young adults.
Clinical Significance
Children and young adults using SGAs are at increased risk of developing T2DM even with short-term use of less than 1 year. Risk of diabetes should be considered when evaluating the risk and benefits of SGAs among younger people.
Footnotes
Disclosures
S.X.'s education was supported by the 2014–2016 University of Illinois in Chicago/Takeda Pharmaceuticals USA, Inc. Fellowship in Medication Adherence Fellowship. Takeda Pharmaceuticals had no input or influence on design, results, or interpretation of this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.