
Abstract
Objectives:
Beta-blockers relieve the autonomic symptoms of exam-related anxiety and may be beneficial in exam-related and performance anxiety, but knowledge on related psychiatric outcomes is unknown. We hypothesized that beta-blocker therapy for exam-related anxiety identifies young students at risk of later psychiatric events.
Methods:
Using Danish nationwide administrative registries, we studied healthy students aged 14–30 years (1996–2012) with a first-time claimed prescription for a beta-blocker during the exam period (May–June); students who were prescribed a beta-blocker for medical reasons were excluded. We matched these students on age, sex, and time of year to healthy and study active controls with no use of beta-blockers. Risk of incident use of antidepressants, incident use of other psychotropic medications, and suicide attempts was examined by cumulative incidence curves for unadjusted associations and multivariable cause-specific Cox proportional hazard analyses for adjusted hazard ratios (HRs).
Results:
We identified 12,147 healthy students with exam-related beta-blocker use and 12,147 matched healthy students with no current or prior use of beta-blockers (median age, 19 years; 80.3% women). Among all healthy students, 0.14% had a first-time prescription for a beta-blocker during the exam period with the highest proportion among students aged 19 years (0.39%). Eighty-one percent of the students filled only that single prescription for a beta-blocker during follow-up. During follow-up, 2225 (18.3%) beta-blocker users and 1400 (11.5%) nonbeta-blocker users were prescribed an antidepressant (p < 0.0001); 1225 (10.1%) beta-blocker users and 658 (5.4%) nonbeta-blocker users were prescribed a psychotropic drug (p < 0.0001); and 16 (0.13%) beta-blocker users and 6 (0.05%) nonbeta-blocker users attempted suicide (p = 0.03). Exam-related beta-blocker use was associated with an increased risk of antidepressant use (adjusted HRs, 1.68 [95% confidence intervals (CIs), 1.57–1.79], p < 0.0001), other psychotropic medication use (HR, 1.93 [95% CI, 1.76–2.12] p < 0.0001), and suicide attempts (HR, 2.67 [95% CI, 1.04–6.82] p = 0.04).
Conclusion:
In healthy students, use of beta-blockers during the exam period was associated with an increased risk of psychiatric outcomes and might identify psychologically vulnerable students who need special attention.
Introduction
D
Anxiety disorders in childhood or adolescence are associated with an increased risk of developing severe psychiatric disorders in adulthood (Kim-Cohen et al. 2003; Maibing et al. 2015), especially depression (Watson 2005; Moffitt et al. 2007a, 2007b; Lahey et al. 2008; Copeland et al. 2014; Meier et al. 2015), and there is also evidence of a genetic contribution to the comorbidity between anxiety and later depression (Franic et al. 2010; Silk et al. 2012). However, little is known on the short- and long-term psychiatric outcome of exam-related anxiety of the intermediate use of beta-blockers for such difficulties, and data on utilization are sparse. We hypothesized that students who use beta-blockers for this purpose are at higher risk of later psychiatric events.
To address this, we conducted a nationwide retrospective cohort study to examine the prevalence of first-time use of beta-blockers during the exam period (May–June) among healthy students and compare the risk of antidepressant use, other psychotropic drug use, and suicide attempts with matched controls without beta-blocker therapy.
Method
Data sources
The assignment of a unique and permanent civil registration number to all residents in Denmark allows linkage of nationwide administrative registries at an individual level. The registries include information on sociodemographic characteristics, hospitalizations, outpatient visits, prescribed medication, and education. For this study, we used five different registries. The Danish National Patient Registry contains information on all admissions to Danish hospitals since 1977. Each admission is registered by one primary diagnosis and, if appropriate, one or more secondary diagnosis according to the International Classification of Diseases (ICD-8 and ICD-10 until and from 1994, respectively) (Lynge et al. 2011). The Danish Registry of Medicinal Product Statistics holds detailed information on all claimed drug prescriptions dispensed from pharmacies in Denmark since 1995. The drugs are classified according to the international Anatomical Therapeutic Chemical (ATC) system with information on dispensing date, strength, and quantity dispensed. Due to partial reimbursement of drug expenses by the healthcare system, pharmacies in Denmark are, by legislation, obliged to register all dispensed prescriptions, ensuring complete registration (Kildemoes et al. 2011). The Danish Student Registry contains information on enrolment, progression, graduation, and discontinuation in educational programs for each resident and is updated annually with reports from educational institutions. All public-recognized educational programs in Denmark, from preschool to graduate studies at university level, are included in the registry (Jensen and Rasmussen 2011). The educational programs are divided into five categories in accordance with the International Standard Classification of Education: Basic school; high school; vocational education; short-/medium-length higher education; and long higher education or research. Information on vital status was obtained from the Danish National Population Registry, in which information on all deaths is registered within 2 weeks after their occurrence (Pedersen 2011). Causes of death based on death certificates according to the ICD-10 were obtained from the Danish Registry of Causes of Death (Helweg-Larsen 2011).
Study population
For this study, we obtained information on all Danish residents born between January 1, 1972 and December 31, 1998 (2.37 million individuals). We identified all Danish residents aged 14–30 years with a first-time claimed prescription for a beta-blocker (ATC-code C07) during the exam period between January 1, 1996 and December 31, 2012. The date of the first-time claimed prescription for a beta-blocker was defined as the index date. In Denmark, exams are held from December to January (only students enrolled in a long higher education) and May to June (all students regardless of education level). As the vast majority of exams are held from May to June, we defined the exam period as the calendar months of May and June. Supplementary Figure S1 (Supplementary Data are available online at
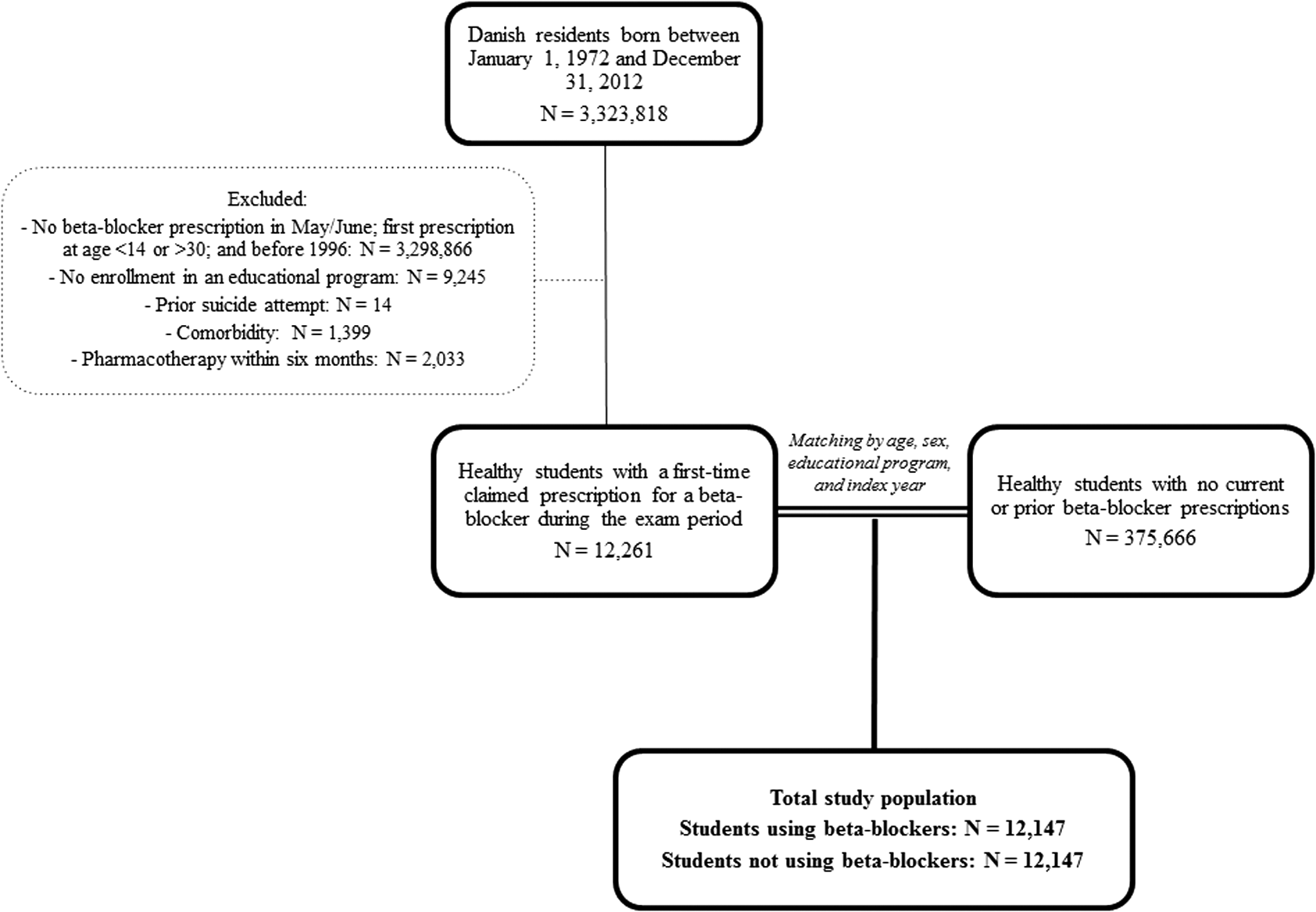
Flowchart of the study population selection process.
Retrospective registry-based studies do not require ethical approval in Denmark. This study was approved by the Danish Data Protection Agency (reference no: GEH-2014-013, I-suite no: 02731) and data were anonymized so that individuals could not be identified. Due to the Act on Processing of Personal Data, we cannot report any number less than four observations.
Outcomes
The following outcome measures of psychiatric consequences were studied in healthy students with a first-time claimed prescription for a beta-blocker during the exam period and no current or prior use of beta-blockers: (1) incident use of antidepressant medications (ATC-code N06A); (2) other psychotropic drug use defined as incident use of antipsychotics (ATC-code N05A), ADHD medications (ATC-code N06BA), or benzodiazepines (ATC-code N05BA); and (3) suicide attempts and suicide (ICD-10 codes X60-X84 as primary code on hospital admission discharge and death certificate, respectively).
Subgroup analyses
We performed a number of subgroup analyses, including (1) students with propranolol only as the class of beta-blocker at the first-time claimed prescription; (2) men; (3) women; (4) students enrolled in basic school; (5) students enrolled in high school; (6) students enrolled in a vocational education; (7) students enrolled in a short-/medium-length higher education; and (8) students enrolled in an long higher education or research.
Statistical analysis
The prevalence of beta-blocker use was calculated as a simple proportion in the data sample and differences in use per age and sex were examined. Outcomes were examined by cumulative incidence curves for unadjusted differences between groups using Gray's test accounting for the competing risk of death. Multivariable cause-specific Cox proportional hazard models adjusted for age, sex, and education level were used to analyze the association between beta-blocker use versus no beta-blocker use and outcomes. Model assumptions were tested and found valid. Important interactions were tested and found statistically not significant unless otherwise indicated.
All statistical analyses were performed with SAS statistical software (SAS 9.4, SAS Institute, Cary, NC). A two-sided p-value <0.05 was considered statistically significant.
Sensitivity analysis
To test the robustness of our results, we compared the risk of fractures among students with exam-related beta-blocker use with those who did not use beta-blockers. This was to examine whether beta-blocker use was associated with an unexpected outcome. In addition, we compared the risk of psychiatric outcomes among students with exam-related beta-blocker use to unmatched students with no use of beta-blockers.
Results
A total of 12,147 students aged 14–30 years with a first-time claimed prescription for a beta-blocker during the exam period between January 1, 1996 and December 31, 2012 were identified. We matched these cases with 12,147 healthy controls (students with no current or prior use of beta-blockers) (Fig. 1). The median age was 19 years (interquartile range: 18–22), and 80.3% were women.
A total of 0.14% of all healthy students in Denmark had a first-time prescription for a beta-blocker during the exam period; 81% of these students filled only that single prescription for a beta-blocker. Throughout the study period, exam-related beta-blocker use remained constant (0.13% in 1996, 0.12% in 2004, and 0.14% in 2012).
Education level characteristics of the identified students are presented in Table 1. The majority of the students were enrolled in high school accounting for 6289 (51.8%) of the total numbers of students using beta-blockers and correspondingly for students not using beta-blockers.
BB, beta-blocker; IQR, interquartile range; ISCED, International Standard Classification of Education.
Figure 2 shows the proportion of healthy students with a first-time claimed prescription for a beta-blocker during the exam period to all healthy students according to age. The proportion increased with increasing age, with the highest proportion observed in students aged 18 and 19 years (0.29% and 0.39%, respectively). The proportion then declined and remained fairly constant in students aged 21 to 30 years.
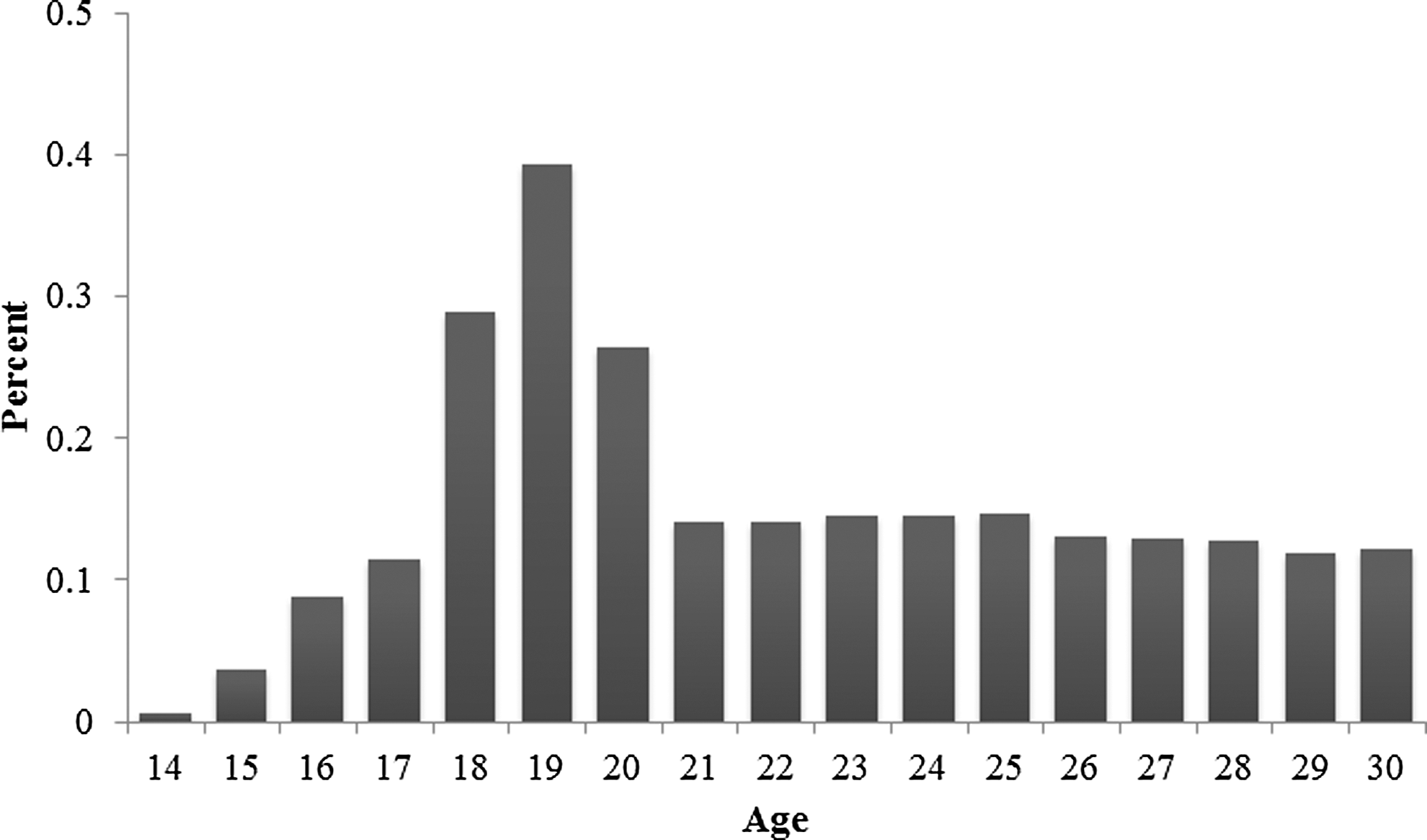
Percentage of healthy students with a first-time claimed prescription for a beta-blocker during the exam period to all healthy students according to age.
The utilization pattern of beta-blockers according to individual drugs is illustrated in Figure 3. Propranolol and metoprolol were the most frequently used beta-blockers accounting for 10,022 (82.5%) and 1189 (9.8%) of the total amount of all beta-blockers prescribed, respectively.
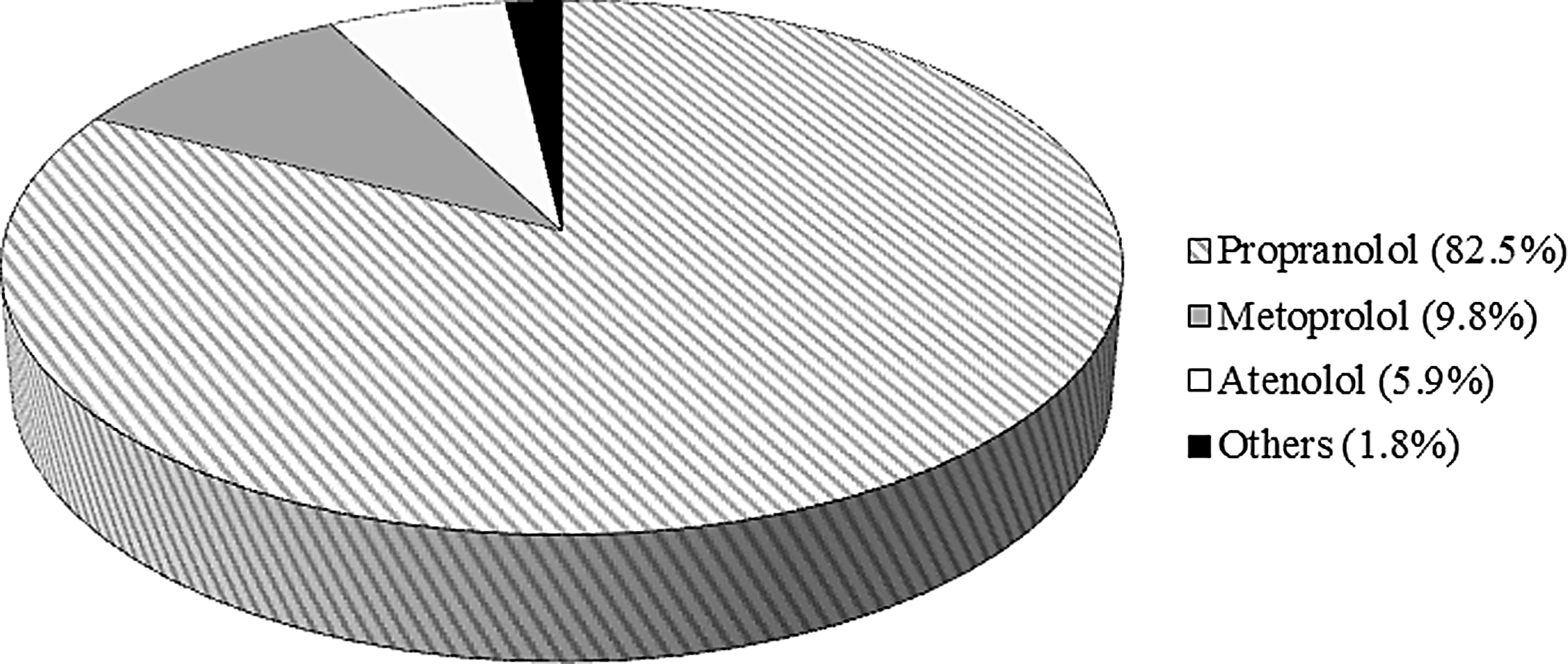
Class of beta-blocker at the first-time claimed prescription during the exam period.
58.8% of the students were prescribed beta-blockers with a pack size of 100 or above. The most frequently prescribed doses were 10 and 40 mg, accounting for 54.6% and 27% of the students, respectively.
Figure 4 illustrates the unadjusted cumulative incidence curves for use of antidepressants (Fig. 4a), use of other psychotropic medications (Fig. 4b), and suicide attempts (Fig. 4c). The results from the multivariable cause-specific Cox proportional hazard analysis for psychiatric outcomes are shown in Figure 5.
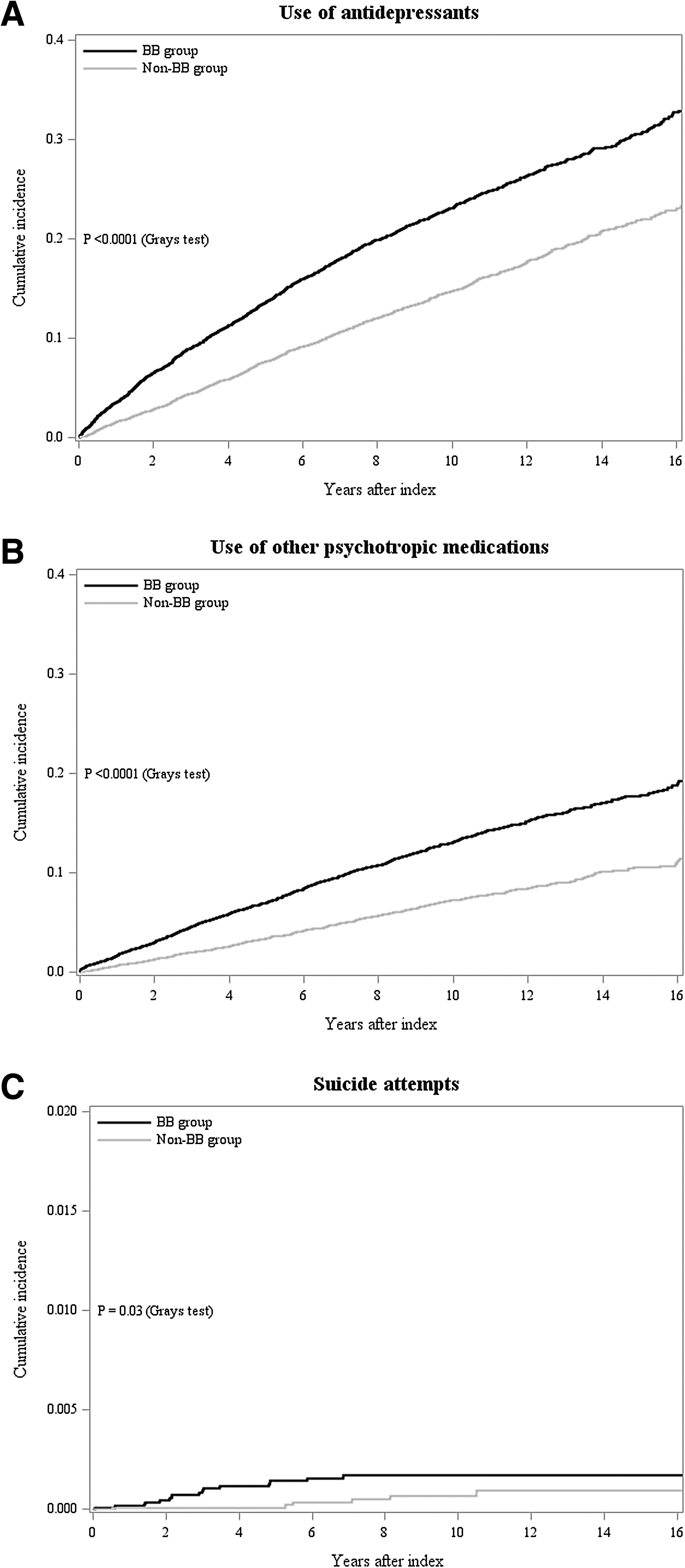
Cumulative incidence curves for
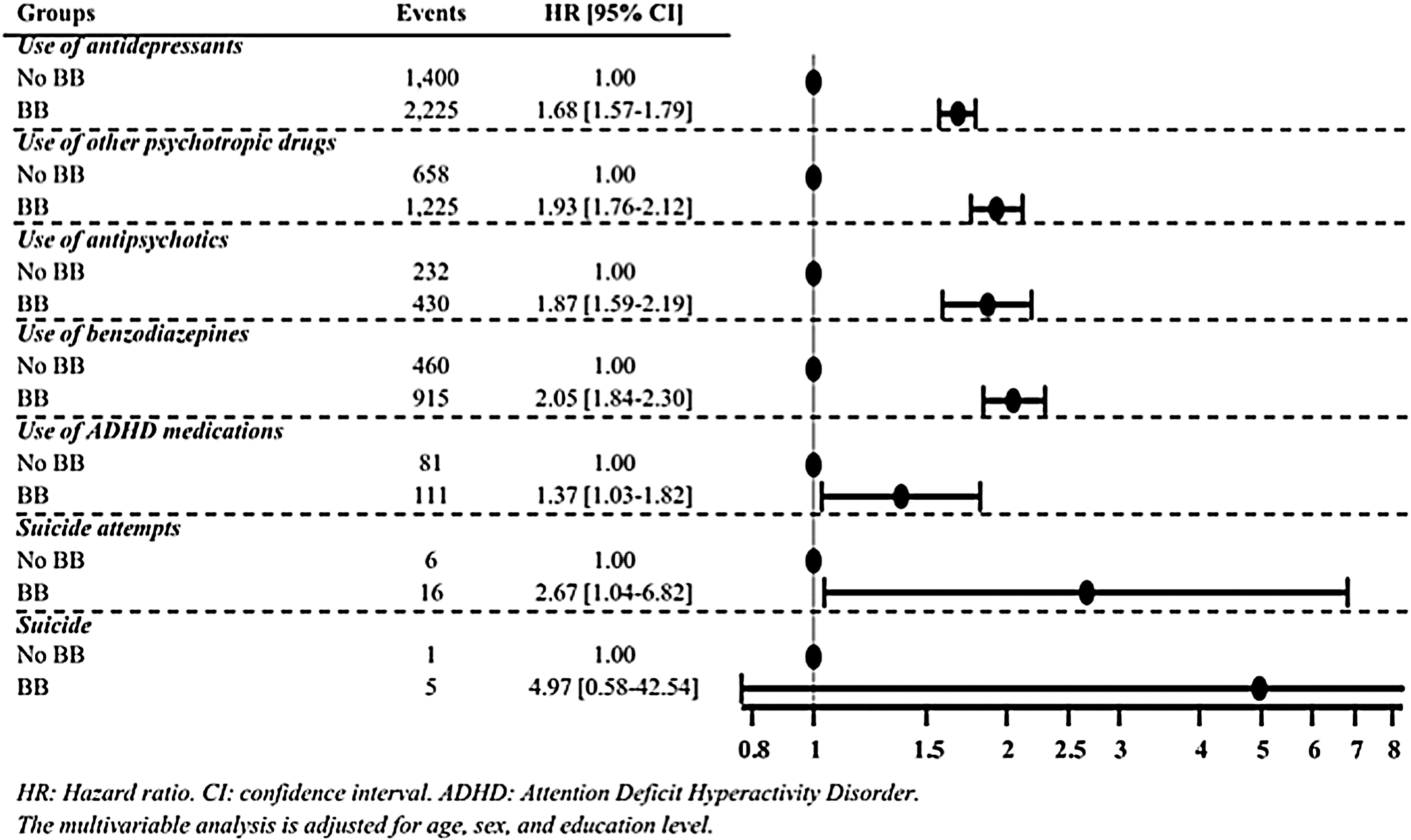
Cox proportional hazard analysis of risk of adverse psychiatric outcomes in healthy students with a first-time claimed prescription for a beta-blocker during the exam period and no current of prior use of beta-blockers.
Antidepressant use
A total of 2225 (18.3%) students using beta-blockers and 1400 (11.5%) students not using beta-blockers had a claimed prescription for antidepressants during follow-up. The mean follow-up period for use of an antidepressant was 4.5 and 5.4 years for students using beta-blockers and students not using beta-blockers, respectively. Students using beta-blockers had a significantly higher cumulative incidence of use of antidepressants compared with students not using beta-blockers (p < 0.0001 [Gray's test]). In multivariable cause-specific Cox proportional hazard analysis adjusted for age, sex, and education level, the risk of antidepressant use was significantly increased with beta-blocker use versus no beta-blocker use during the exam period (HR, 1.68 [95% confidence intervals (CIs), 1.57–1.79], p < 0.0001).
Other psychotropic medication use
During follow-up, 1225 (10.1%) students using beta-blockers and 658 (5.4%) students not using beta-blockers had a claimed prescription for other psychotropic medication. The mean follow-up period for use of other psychotropic medication was 4.8 and 5.5 years for students using beta-blockers and students not using beta-blockers, respectively. The unadjusted cumulative incidence curve showed a significantly higher cumulative incidence of psychotropic drug use in students using beta-blockers compared with students not using beta-blockers (p < 0.0001 [Gray's test]). The multivariable cause-specific Cox proportional hazard analysis adjusted for age, sex, and education level found a significantly increased risk of psychotropic drug use with first-time prescription of beta-blockers during the exam period (HR, 1.93 [95% CI, 1.76–2.12], p < 0.0001).
Psychotropic drug use was defined as the incident use of antipsychotic medications, ADHD medications, and benzodiazepines. The risk of utilizing each of these medication groups was significantly increased with beta-blocker use versus no beta-blocker use during the exam period in multivariable cause-specific Cox proportional hazard analysis adjusted for age, sex, and education level (Fig. 5).
Suicide attempts and suicide
Suicide was attempted by 16 (0.13%) students using beta-blockers and 6 students (0.05%) not using beta-blockers related to the exam period. The mean follow-up period for a suicide attempt was 2.9 and 6.2 years for students using beta-blockers and students not using beta-blockers, respectively. Students using beta-blockers had a significantly higher cumulative incidence of suicide attempts compared with students not using beta-blockers (p = 0.03 [Gray's test]). In multivariable cause-specific Cox proportional hazard analysis adjusted for age, sex, and education level, the risk of suicide attempts was significantly increased with first-time prescription for beta-blockers during the exam period (HR, 2.67 [95% CI, 1.04–6.82], p = 0.04).
Five students using beta-blockers and less than four students not using beta-blockers committed suicide. In multivariable cause-specific Cox proportional hazard analysis adjusted for age, sex, and education level, the risk of suicide did not differ significantly with first-time prescription for beta-blockers during the exam period (HR, 4.97 [95% CI, 0.58–42.54], p = 0.14).
Subgroup analyses
Men using beta-blockers were at a higher risk of using antidepressants (HR, 2.14 [95% CI, 1.55–1.79], p < 0.0001), whereas the association for women was weaker, although still significantly increased versus women who did not use beta-blockers (HR, 1.62 [95% CI, 1.50–1.74], p < 0.0001) (p for interaction 0.006). We found no statistically significant interaction between gender and beta-blocker use for the remaining outcomes. Looking at age, we found a significant interaction showing that older students using beta-blockers had an increased risk of using antidepressants (p for interaction 0.03) and other psychotropic drugs (p for interaction 0.002). Students aged > median age were associated with higher risk of using antidepressants (HR, 1.81 [95% CI, 1.64–1.99], p < 0.0001) and other psychotropic drugs (HR, 2.33 [95% CI, 2.02–2.68], p < 0.0001). The associations for students aged ≤ median age were weaker, although still significantly increased, versus young students who did not use beta-blockers (HR, 1.57 [95% CI, 1.44–1.72], p < 0.0001 for use of antidepressants; HR, 1.64 [95% CI, 1.44–1.87], p < 0.0001 for use of other psychotropic drugs). In addition, beta-blocker use at higher levels of education was associated with a higher risk of psychiatric outcomes relative to lower levels of education (statistically significant p-values for interaction). Please see Supplementary Table S3 for the full results.
Sensitivity analysis
We compared the risk of specific fractures among healthy students with exam-related beta-blocker use to those who did not use beta-blockers. Beta-blocker use was not associated with an increased risk of fractures (HR, 1.06 [95% CI, 0.96–1.18], p = 0.25). In addition, we compared the risk of psychiatric outcomes among healthy students with exam-related beta-blocker use to unmatched healthy students with no use of beta-blockers (N = 375,666). The results were similar as exam-related use of beta-blockers was significantly associated with an increased risk of later use of antidepressants, use of other psychotropic medications, and suicide attempts (data not shown).
Discussion
In this nationwide cohort study, we examined psychiatric outcomes associated with first-time use of beta-blockers during the exam period among healthy students. Our analysis yielded three major findings. First, beta-blocker use during the exam period was low, but highest among high school students, those aged 18–19, and women. Second, exam-related use of beta-blockers was associated with an increased risk of later use of antidepressants, use of other psychotropic medications, and suicide attempts. Third, although the vast majority of beta-blocker users were women, men seemed at higher risk of psychiatric illness on the long term. We believe that our results should raise an increased awareness of the fact that exam-related beta-blocker use might identify young individuals in the need of special attention.
To our best knowledge, this is the first study to examine psychiatric outcomes in healthy students with exam-related anxiety treated with beta-blockers. These students have a significantly higher risk of use of antidepressants, use of other psychotropic medications, and suicide attempts, subsequently, compared with their peers who do not use beta-blockers for exams. In addition, the use of antipsychotics, ADHD-medications, and benzodiazepines individually is significantly associated with prior exam-related anxiety treated with beta-blockers. Overall, our results suggest that seemingly healthy students, who have exam-related anxiety so impairing that they are prescribed a beta-blocker, in general, are more psychologically vulnerable than students with no beta-blocker use. These students probably represent a group of individuals more susceptible to developing a psychiatric disorder, requiring an antidepressant, antipsychotic, stimulant, or anxiolytic drug and who may have a genetic disposition to, for instance, depression (Franic et al. 2010; Silk et al. 2012).
Our results demonstrate that students between 18 and 20 years have the highest prevalence of first-time use of beta-blockers during the exam period. These students are mainly enrolled in high school and are preparing for their upper secondary school exams. The academic results (the grades) are of great importance for the students' future opportunities in the education system, as it plays a vital role for admission to higher education. Hence, pressure to perform well in exams to enable enrolment to the preferred graduate program may exacerbate existing psychological difficulties or trigger new ones (Suicide Prevention Resource Center 2014). Thus, to perform to the best of their abilities, students, in particular those who are psychologically vulnerable, may feel tempted to resort to beta-blocker therapy to relief exam-related anxiety. However, older students were significantly more likely than younger students to be started on antidepressant medications as well as other psychotropic drugs. This relationship was also demonstrated by a dose–response-like association with the level of education; the risk of psychiatric illness was attenuated by enrolment into higher levels of education.
In addition to age differences in exam-related use of beta-blockers, our study also demonstrates differences between genders. Women constitute the majority of students prescribed beta-blockers during the exam period. A part of the explanation may be that young women consult their general practitioner more often than men (Sayer and Britt 1996; Wang et al. 2013) and are therefore more likely to receive beta-blocker therapy, thereby introducing observation bias. Another reason may also be that more women than men are enrolled in higher education in Denmark. Interestingly, men using beta-blockers were more likely than women using beta-blockers to initiate antidepressant medications. Hence, our results suggest that men who seek a doctor for the prescription of a beta-blocker in the exam period are more susceptible to developing a psychiatric disorder. This may also be explained by men's infrequent use of their general practitioner.
We also found that 81% of the students filled a single prescription for a beta-blocker. Although the majority filled a single prescription only, these students consulted their doctors and were prescribed antidepressants and other psychotropic drugs later on in their lives. It is plausible to assume that the students did not have any positive effect of beta-blockers. However, the majority of the students were prescribed quite large pack sizes and was therefore likely covered with beta-blockers for more than one exam period. In view of this, it is difficult to say anything about the perceived effect of the drug.
Guidelines do not recommend the use of beta-blockers for treatment of anxiety disorders, as studies have not been able to show efficacy of these drugs in patients suffering from anxiety (Bandelow et al. 2008; Katzman et al. 2014); more specifically, the scientific evidence to support the use of beta-blockers for exam-related anxiety is modest (Brewer 1972; Brantigan et al. 1982; Neftel et al. 1982; James and Savage 1984; Drew et al. 1985; Gates et al. 1985; Bourgeois 1991; Faigel 1991; Elman et al. 1998). Despite clear guidelines, young and seemingly healthy students are prescribed beta-blockers, although these drugs are not approved for such indications. Under which circumstances physicians prescribe beta-blockers for exam-related anxiety are unknown. Thus, it is not unthinkable that these physicians are not representative for general practitioners as a group, but rather represent a subgroup of physicians.
Strengths and Limitations
The main strength of this study is the completeness of data from nationwide registries avoiding selection bias with a follow-up of several years. Due to partial reimbursement of drug expenses by the Danish healthcare system, pharmacies are required to register all dispensed prescriptions, which ensure complete registration. In Denmark, all beta-blockers can be purchased only through prescription.
The main limitation of this study is inherent in its observational nature. Information about the precise indication for initiation of beta-blocker treatment was not available; thus the possibility that some of these students may have a medical reason for initiation of beta-blocker therapy (e.g., hypertension) and are followed by their general practitioner is present, although we tried as best possible to exclude such cases. Importantly, the vast majority of the patients did not claim multiple prescriptions for beta-blockers as would be expected for treatment of for example, hypertension. Another limitation is that we only included students with a first-time claimed prescription for a beta-blocker in May and June, thus leaving out students with a potential exam-related beta-blocker use in other months. However, this has little effect on our results as the majority of exams in Denmark are held in May and June. We excluded students with a prescription for antidepressants and other psychotropic drugs only 6 months before the index date. However, excluding students with any use of these medications before the index date did not change our results (data not shown). Moreover, suicide attempts in both groups may have been underestimated. Some suicide attempts do not result in a hospital admission, and we have only data from suicide attempts resulting in a hospital admission. However, we do not expect that this fact differs between our exposure groups. Furthermore, we cannot rule out that students with a beta-blocker prescription may offer this drug to other students with no prescriptions (Fishbein et al. 1988); however, this would only dilute the study sample and hence pull the studied association toward the null. In addition, some individuals among the earliest cohorts may have been treated with beta-blockers before 1995, and we have no available information on drug prescriptions before 1995. The mechanism behind the anxiolytic effects of propranolol may be an attenuation in the neural responses to fear in the dorsal medial prefrontal cortex (Kroes et al. 2015), thereby attenuating a conditioned response to fear-relevant stimuli, as shown in studies of animals (Shannonhouse et al. 2014), healthy controls (Kindt et al. 2009; Kindt and Soeter 2013), and patients (Brunet et al. 2008). However, this would not be expected to explain the association found in our study as most of the beta-blocker users only filled one prescription for a beta-blocker and therefore were only exposed to short-term transient beta-blocker use. Likewise, although depression may be a less common side effect of beta-blocker use, the beta-blocker users in our study were exposed only to short-term transient use of this drug.
Conclusions and Clinical Implications
In this nationwide cohort study, students who used beta-blockers during the exam period were associated with significantly higher risk of later psychiatric events such as use of antidepressants, other psychotropic drug use, and suicide attempts compared with their peers who did not use beta-blockers. Although beta-blocker therapy may relieve exam-related anxiety, the need for treatment might indicate individual psychological vulnerability and need for special attention. Healthcare providers, in particular general practitioners, should be aware that although severe exam-related anxiety is rare, it is not merely an isolated phenomenon, but may be associated with a higher risk of later psychiatric outcomes. Beta-blocker prescriptions during the exam period may therefore be accompanied by a follow-up by the prescribing doctors to ensure the well-being of the students and explore any underlying psychological or psychiatric difficulties. Our findings should not be used to infer any causal effects of the use of beta-blockers. Rather, in line with results from previous studies of childhood anxiety (Kim-Cohen et al. 2003; Maibing et al. 2015), our findings suggest that exam-related anxiety is associated with an increased risk of developing more severe and impairing psychopathology.
Clinical Significance
Our findings suggest that exam-related anxiety is associated with an increased risk of developing more severe and impairing psychopathology in adulthood. Although beta-blocker therapy may relief exam-related anxiety, the need for treatment may indicate individual psychological vulnerability and need for special attention. Thus, healthcare providers, in particular general practitioners, should be aware that severe exam-related anxiety may be associated with a higher risk of later psychiatric outcomes. Beta-blocker prescriptions during the exam period may therefore be accompanied by a follow-up by the prescribing doctors to ensure the well-being of the students and to explore any underlying psychological or psychiatric difficulties.
Footnotes
Disclosures
Dr. C.T.-P. has received speaker fees from Bayer, Merck, and Bristol-Meyers Squibb and research grants from Bayer; Dr. L.K. has received speaker fees for presentation at a symposium; and Dr. G.H.G. is supported by an unrestricted research scholarship from the Novo Nordisk Foundation. All authors declare no support from any organization for the submitted work; no financial relationship with any organization that might have an interest in the submitted work in the previous 3 years, and no other relationships or activities that could appear to have influenced the submitted work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.