
Abstract
Background:
Prior studies have suggested that inhibited temperament may be associated with an increased risk for developing anxiety or mood disorder, including bipolar disorder. However, the neurobiological basis for this increased risk is unknown. The aim of this study was to examine temperament in symptomatic and asymptomatic child offspring of parents with bipolar disorder (OBD) and to investigate whether inhibited temperament is associated with aberrant hippocampal volumes compared with healthy control (HC) youth.
Methods:
The OBD group consisted of 45 youth, 24 of whom had current psychiatric symptoms (OBD+s) and 21 without any psychiatric symptoms (OBD−s), and were compared with 24 HC youth. Temperament characteristics were measured by using the Revised Dimensions of Temperament Survey. Magnetic resonance imaging was used to measure hippocampal volumes. The association between temperament and hippocampal volumes was tested by using multiple regression analysis.
Results:
Compared with the OBD−s group, the OBD+s group had significantly more inhibited temperament traits, less flexibility, more negative mood, and less regular rhythm in their daily routines. In contrast, the OBD−s group was more likely to approach novel situations compared with OBD+s or HC groups. Within the OBD+s group, a more inhibited temperament was associated with smaller right hippocampal volumes.
Conclusions:
In this study, symptomatic OBD were characterized by an inhibited temperament that was inversely correlated with hippocampal volume. Additional longitudinal studies are needed to determine whether inverse correlations between hippocampal volume and inhibited temperament represent early markers of risk for later developing bipolar disorder.
Introduction
O
Prior research has shown that temperament is heritable (Rothbart and Ahadi 1994; Meyer-Lindenberg 2010), manifests early in life, and is stable over the life course (McCrae et al. 2000). Consequently, key temperament traits may contribute to early risk for BD, may predate disorder onset, and may be less affected by shifting mood symptoms. If certain temperament features increase the possibility that a child may develop BD, they may be used for identifying high-risk children, who may be followed prospectively or targeted for preventive interventions (Singh et al. 2008).
Recent research suggests that inhibited temperament may be a useful predictor for the development of mood disorders, including characteristics such as harm avoidance (HA), behavioral inhibition, or neuroticism (Hirshfeld-Becker 2003; Kemner et al. 2015; Fountoulakis et al. 2016). Inhibited temperament is broadly defined as a tendency to withdraw from novel stimuli, has been linked to higher stress reactivity, behavioral inhibition, and other measures of emotionality, and is reported to have links to both unipolar and bipolar mood disorders (Hirshfeld-Becker 2003; Ormel et al. 2004; Rothen 2009; Whalley et al. 2011; Fountoulakis et al. 2016). Indeed, patients with BD report more HA and neuroticism compared with healthy individuals, even during periods of euthymia (Engstrom et al. 2004; Christensen and Kessing 2006; Olvera et al. 2009). Some individuals with BD have exhibited high levels of inhibited temperament, whereas others have exhibited high novelty-seeking and impulsivity (Savitz and Ramesar 2006; Loftus et al. 2008; Olvera et al. 2009; Jylha et al. 2011; Zaninotto et al. 2016).
In youth who are offspring of parents with BD, studies have shown decreased flexibility, high distractibility, increased activity, less regular rhythm in daily routine or sleep, and an inhibited temperament (Chang et al. 2003; Singh et al. 2008). Indeed, these traits commonly coincide with psychiatric disorders such as anxiety and attention deficit hyperactiviy disorder (ADHD) (Bernardi et al. 2010; Graham et al. 2015), which may independently place youth at risk for BD. Although some studies have found that temperament is not a risk factor for BD (Spittlehouse et al. 2010; Ratheesh et al. 2015), a recent meta-analysis of 57 studies has suggested that inhibited temperament or HA is among the most commonly associated temperament traits in patients with major mood disorders (both bipolar disorder and major depressive disorder) and their unaffected siblings (Zaninotto et al. 2016).
Taken together, it is not yet known whether certain temperament traits are present before the onset of mood and other psychiatric symptoms, and what neurobiological features might be associated with temperament characteristics in youth at risk for BD.
Studies in individuals with BD have demonstrated volumetric changes in cortical and subcortical structures of the brain that may, in part, be explained by individual variations in temperament (Fusar-Poli et al. 2012; Lim et al. 2013; Phillips and Swartz 2014). Most consistently, youth with BD show evidence of decreased amygdalar and hippocampal volumes (Frazier et al. 2005; Pfeifer et al. 2008). In contrast, researchers have not found any structural abnormalities in non-symptomatic first-degree relatives of individuals with BD (Singh et al. 2008; Hajek et al. 2009), raising the possibility that structural abnormalities may not occur until high-risk youth have already developed significant symptoms of BD (Fusar-Poli et al. 2012; Lim et al. 2013). It is not yet known whether temperament traits might be associated with key neuroanatomical abnormalities that represent early markers for the development of BD. The hippocampus is activated in response to novel stimuli, is well-known for its roles during stress response and in the pathophysiology of mood disorders, and is strongly associated with approach and withdrawal behaviors (Oler et al. 2010; Blackford et al. 2013) and inhibited temperament (Clauss et al. 2015). Thus, the hippocampus may be an important region to investigate in relation to inhibited temperament in symptomatic and asymptomatic youth at risk for BD.
Thus, we aimed at characterizing the temperament and the neuroanatomical underpinnings of temperament in offspring of bipolar parents (OBD) who may be at high risk for developing BD. Specifically, we compared the temperament and hippocampal neuroanatomy of OBD with psychiatric symptoms (OBD+s), with those OBD without any psychiatric symptoms (OBD−s), and with healthy controls (HC). Based on prior studies (Rottig et al. 2007), we hypothesized that OBD+s youth will have higher levels of inhibited temperament compared with OBD−s and HC groups and hippocampal volume might be associated with inhibited temperament in high-risk offspring of parents with BD.
Methods
Participant recruitment and assessment
The study protocol was approved by the Stanford University Panel of Medical Research in Human Subjects. Written informed consent was obtained from at least one parent, and assent was obtained from the youth.
Participants were drawn from two ongoing studies of child and adolescent offspring of parents with BD. Participants ranged in age between 8 and 17 years, and only one child per family was included. Participants were included in the OBD+s group if they had a biological parent with bipolar I or II disorder, and if the children themselves had past or current major depression or ADHD, and also had moderate mood symptoms (Young Mania Rating Scale [YMRS] Score >12) (Young et al. 1978) or Children's Depression Rating Scale (CDRS) score >30 on the day of assessment (Poznanski et al. 1979). Symptoms of anxiety were assessed by using the Multidimensional Anxiety Scale for Children (MASC) (March et al. 1997). Twenty-one OBD−s youths had at least one biological parent diagnosed with bipolar I disorder but themselves had no psychiatric symptoms, and 24 HC youths had no personal or family history in first- or second-degree relatives of any Axis I disorder. Exclusion criteria for all subjects included a diagnosis of bipolar I and II disorder (which would render youth no longer at risk for BD), the presence of a pervasive development disorder (such as autism or Asperger's disorder), a neurological condition (such as a seizure disorder), a substance use disorder, an intelligence quotient (IQ) less than 80, presence of metallic implants or braces that would not permit magnetic resonance imaging (MRI), or current hospitalization.
Parental diagnosis of BD I or II was confirmed in OBD by using the Structured Clinical Interview for DSM-Disorders (SCID) (Spitzer et al. 1992). Youth were assessed by the affective module of the Washington University Kiddie Schedule for Affective Disorders and Schizophrenia (WASH-U-SADS) (Geller et al. 2001) for assessment of mood disorder, and the Kiddie Schedule for Affective Disorders and Schizophrenia-Present and Lifetime version (KSADS-PL) (Kaufman et al. 1997) for all other psychiatric disorders. Board-certified psychiatrists or masters-level clinicians with high inter-rater reliability (kappa >0.9) interviewed parents and children separately; final diagnoses were reviewed at consensus conferences attended by the principal investigators (MKS, KDC). The Wechsler Abbreviated Scale of Intelligence was used to estimate IQ. Lifetime exposure to psychotropic medications was gathered via family and participant self-report and was reviewed by study clinicians.
The Revised Dimensions of Temperament Survey (DOTS-R) (Windle 1992) was used to assess temperament in participants (overall k = 0.54–0.81 in school-age children) (Windle 1986). One parent, self-identified as the primary caregiver, in each family completed the DOTS-R for their offspring. In most (90%) of the OBD families, the parent with BD responded to the questionnaire and was euthymic at the time they completed the DOTS-R as established by the SCID. Parents answered 54 items that assessed the following 9 temperament characteristics on a continuous scale: Activity Level-General (higher scores indicate higher levels of energy and motor activity), Activity Level-Sleep (higher scores indicate higher motor activity during sleep), Flexibility-Rigidity (higher scores indicate greater ability to adapt to new situations), Approach-Withdrawal (higher scores indicate a greater tendency to approach new situations, things, or people and lower scores index inhibited temperament), Rhythmicity-Sleep (higher scores indicate greater ability to follow the same daily sleeping patterns), Rhythmicity-Eating (higher scores indicate a greater ability to follow the same daily eating patterns), Rhythmicity-Daily Habits (higher scores indicate greater regularity in daily timing of habits such as toileting, and consistent peaks and dips in energy levels), Task Orientation (higher scores indicate greater persistence on tasks without easy distraction), and Mood (higher scores indicate consistently greater positive moods).
Analysis of variance (ANOVA) was used to compare demographic variables, mean DOTS-R, YMRS, and CDRS scores among OBD+s, OBD−s, and HC subjects, using IBM SPSS Statistics Version 20. Pearson correlations were conducted to explore the within-group relations between temperament and manic and depressive symptom severity, as assessed by the DOTS-R subscale scores, the YMRS, and the CDRS, respectively. A p-value of 0.006 (two-tailed) was chosen as the Bonferroni-corrected significance threshold to adjust for multiple comparisons in nine subscales of DOTS-R scale. Temperament subscales with significant group differences after adjusting for multiple comparisons were then explored for relations to hippocampal volume by using multiple regression. To assess the independent effects of mood and anxiety symptoms at the time of scan, relations between hippocampal volumes and measures of depression (CDRS) and anxiety (MASC) were examined.
MRI acquisition and imaging analysis
Magnetic resonance images of each subject's brain were all acquired at the Lucas Center of Radiology at Stanford University by using two GE 3T scanners (GE Medical Systems, Milwaukee) with a 16-channel head coil. Coronal images were acquired with a three-dimensional volumetric radio frequency spoiled gradient echo with the following scan parameters: OBD+s group and its respective controls: TR = 3.5 msec, TE = 6 msec, flip angle = 45, number of excitations = 1, image matrix = 256 × 192 pixels, field of view = 24 cm, slice thickness = 1.5 mm, 124 slices, acquired resolution = 1.5. OBD−s group and its respective controls: TR = 8.528 msec, TE = 3.396 msec, flip angle = 15, number of excitations = 1, image matrix = 256 × 192 pixels, field of view = 22 cm, slice thickness = 1.5 mm, 124 slices, acquired resolution = 1.5. Images acquired from the two different scanners were not directly compared with each other. Rather, neuroanatomical comparisons were made with respective control groups at each scanner. Volumetric segmentation was performed with the FreeSurfer image analysis suite (single machine with OS X Mountain Lion with version 5.3), which is documented and freely available for download online (
As stated earlier, the associations between DOTS-R approach-withdrawal score and the hippocampal volume were tested by using multiple regression analysis, with hippocampal volume as a dependent variable and DOTS-R approach-withdrawal score, total brain volume (TBV), sex, CDRS and MASC scores (to investigate the effect of depression and anxiety symptoms on hippocampal volume) in OBD+s group and DOTS−R approach-withdrawal score, and TBV and sex in OBD−s group as predictor variables. To explore whether specific sex differences were driving the results, analyses were repeated by comparing female and male subsamples in each group.
Results
Demographic, clinical, and temperament characteristics of participants
Demographic and clinical characteristics of the participants are presented in Table 1. Twenty-four OBD+s (mean age: 13.8 [3.1], M = 14, F = 10), 21 OBD−s (mean age: 13.4 [2.4], M = 7, F = 14), and 24 HC (mean age: 13.0 [2.4], M = 11, F = 13) were included in all analyses. There were no significant differences among these three groups in age (p = 0.577) or IQ (p = 0.722), but there were more female subjects in the OBD−s group than in the OBD+s or HC groups. As expected, CDRS and MASC scores were significantly higher in the OBD+s, compared with HC and OBD−s groups. Twelve (50%) of OBD+s subjects were diagnosed as having mood disorder, including depressive disorder NOS and major depressive disorder; eight OBD+s youth had a diagnosis of ADHD; and four OBD+s had co-occurring depressive disorder and ADHD.
OBD+s, offspring of bipolar disorder with psychiatric symptoms; OBD−s, offspring of bipolar disorder without psychiatric symptoms; HC, healthy controls; YMRS, Young Mania Rating Scale; CDRS, Children's Depression Rating Scale; MASC, Multidimensional Anxiety Scale for Children; SD, standard deviation; IQ, intelligence quotient.
There was a significant main effect of group in eight out of nine subscales of DOTS-R, as determined by one-way ANOVA (Table 2). Bonferroni post hoc comparisons revealed that the OBD+s group had a significantly increased mean activity level-general score, a significantly lower flexibility-rigidity (p = 0.003), and mood (p < 0.005) scores, and showed trends for decreased task orientation (p = 0.036) and rhythm in daily habits (p = 0.047) compared with the HC group. Compared with OBD−s youth, OBD+s youth scored significantly lower on the approach-withdrawal, flexibility-rigidity, mood, and rhythm in daily habits subscales, indicating increased withdrawal from the new environment, less flexibility, less positive mood, and less regular rhythm in daily activities. The HC and OBD−s group showed essentially similar temperament profiles across most subscales of DOTS-R, but the OBD−s group showed a trend for higher score than the HC group (p = 0.021) in the approach-withdrawal subscale. This approach-withdrawal subscale was selected as the primary temperament trait of interest for the subsequent investigation for neuroanatomical correlates, because it was the subscale that showed significant group differences between symptomatic and asymptomatic OBD, and in which the OBD−s group showed a trend for greater approach scores than the HC group. Further, to test our hypotheses regarding approach-withdrawal related traits (i.e., HA and novelty seeking) as risk factors for the development of BD, and to investigate whether these traits show related abnormalities in hippocampal volumes in high-risk youth, we selected approach-withdrawal related traits as ideal for further investigation in our study.
Post hoc analysis.
ANOVA, analysis of variance; OBD+s, offspring of bipolar disorder with psychiatric symptoms; OBD−s, offspring of bipolar disorder without psychiatric symptoms; DOTS-R, Revised Dimensions of Temperament Survey; HC, healthy controls.
Neuroimaging results
As shown in Table 3 and Figure 1, DOTS-R approach-withdrawal scores were positively associated with hippocampal volumes in the OBD+s group (total volume: β = 0.51, F [5, 23] = 3.71, p = 0.018) and this association was mainly driven by results from right hippocampus volume (β = 0.55, F [5,18] = 4.61, p = 0.007). No significant association was found between hippocampal volume and anxiety symptoms (MASC scores) or depressive symptoms (CDRS scores).
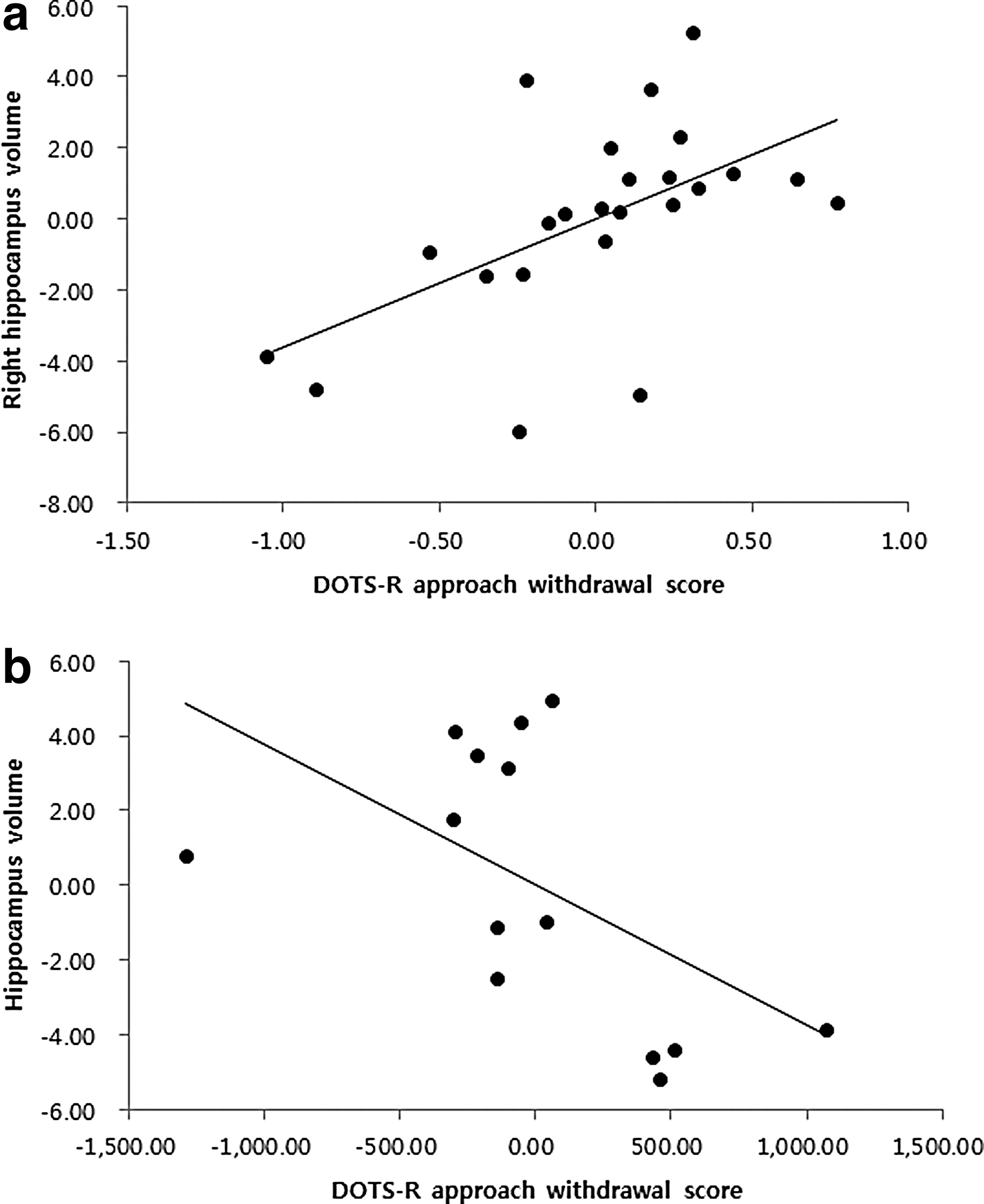
Relation between hippocampus volume and DOTS-R approach-withdrawal (AW) score. x-axes are based on calculated residuals from regressing DOTS-R AW scores on TBV, sex, MASC, and CDRS that were used in OBD+s group
Significant results are reported as *(p < 0.05).
TBV, total brain volume; DOTS-R AW, Revised Dimensions of Temperament Survey Approach-Withdrawal subscale; CDRS, children's depression rating scale; MASC, multidimensional anxiety scale for children; OBD+s, offspring of bipolar disorder with psychiatric symptoms; OBD−s, offspring of bipolar disorder without psychiatric symptoms.
There were no significant associations within either the OBD−s or the HC group. However, exploratory analyses by gender demonstrated a trend for an inverse association between hippocampal volume and approach-withdrawal scores in women in the OBD−s group (β = −0.50, p = 0.05, F [2,11] = −2.17, p = 0.05). Further, the direction of association between DOTS-R approach-withdrawal score and hippocampus volume in OBD−s women was opposite to that in the OBD+s group, demonstrating a more inhibited temperament (lower approach-withdrawal scores) with larger hippocampal volumes.
Discussion
In this study, we found significant temperament differences in symptomatic (OBD+s) compared with asymptomatic (OBD−s) offspring of bipolar parents and HC youths. Further, more inhibited temperament was positively associated with smaller right hippocampal volumes in OBD+s youth and separately, larger hippocampal volumes in female OBD−s youth. This study suggests a potential link between temperament and neuroanatomical morphometry within youth at high risk for BD.
Temperament characteristics of OBD+s, OBD−s, and HC
Our study found that the OBD+s group had a more inhibited temperament (less novelty-seeking), less adaptability to new situations, more negative moods, and less regular rhythm in their daily routines compared with the OBD−s group. These temperament traits in the OBD+s group may represent premorbid risk factors for various types of psychopathology in OBD. Such combinations of temperaments in the OBD+s group have been previously described to constitute a “difficult temperament” with low approach, adaptability, rhythmicity, and negative affect, which may increase risk for various kinds of psychopathology (Chess and Thomas 1977). In contrast, we found no significant temperament difference between OBD−s and HC, suggesting that OBD−s have similar temperament traits to those of HC, with the exception of a higher approach to a new situation. Our finding that the OBD−s group showed a trend for higher scores than the HC group (p = 0.021) in the approach-withdrawal subscale indicates a possible higher tendency of OBD−s to approach new situations and less inhibited temperament.
Our results are consistent with those of previous studies using DOTS-R (Chang et al. 2003; Singh et al. 2008), with some noted exceptions. Chang et al. previously found that offspring of bipolar parents had lower levels of energy and motor activity (Activity Level-General), higher tendencies to approach new situations (Approach-Withdrawal), and higher predictability in daily sleeping patterns (Rhythmicity-Sleep), compared with normative DOTS-R data in a U.S. population sample (Chang et al. 2003). Offspring with no psychiatric diagnoses (similar to OBD−s group in our study) showed these temperament characteristics to an even greater degree than bipolar offspring with a psychiatric diagnosis. Further, studies published on OBD with mood disorders showed a similar profile of temperament to our OBD+s group, showing trends for decreased approach, flexibility-rigidity, and rhythmicity-sleep, compared with OBD without mood disorders (Singh et al. 2008). Subtle differences across studies may be attributed to sampling characteristics and analyses conducted. For example, our study used an age- and IQ-matched HC group rather than a normative U.S. population sample that may have included some individuals with psychopathology. Our HC group might represent a “supernormal” group of youth that may not represent a generalizable sample. In contrast to prior studies, we sampled more even distributions of symptomatic and asymptomatic OBD to examine dissociable temperament traits among these subgroups, especially given the considerable item-overlap between symptom scales and temperament measures, and the potential that mood states may contribute to an inhibited temperament.
We examined the effects of mood and anxiety symptoms in the OBD+s group by conducting bivariate correlational analysis between symptom severity ratings of depression (CDRS) and anxiety (MASC) and the DOTS-R subscale scores. DOTS-R approach-withdrawal scores were not significantly correlated with either of these symptom scores. Consistent with prior studies, these findings suggest that inhibited temperament may be a trait feature that is independent of mood or anxiety state (Sato et al. 2001). Further, our temperament findings correspond with previously characterized temperament traits in euthymic BD subjects (Engstrom et al. 2004; Evans et al. 2005), and by examining healthy offspring of parents with BD without any mood or other psychopathology symptoms, we were able to characterize temperament traits that may precede mood symptom onset.
The association between inhibited temperament and hippocampal volume
To date, few studies have examined the neural correlates of specific temperaments among youth. Some prior studies have demonstrated the involvement of cortical structures in the temperament of healthy youth, including orbitofrontal (DeYoung et al. 2010), occipital, parietal, and left anterior prefrontal cortices (Gardini et al. 2009), and decreased microstructure in widely distributed WM tracts, including cortico-limbic pathways (Westlye et al. 2011). Our results suggest that right hippocampal volume might be associated with an inhibited temperament in high-risk offspring of parents with BD. These results are consistent with a prior study demonstrating that smaller right hippocampal volumes are a premorbid risk factor for mood disorder (Chen et al. 2010; Serafini et al. 2014; Inal-Emiroglu et al. 2015). Inhibited temperament is inversely correlated with hippocampal volume, but this relation may not be specific to youth with or at risk for BD. Indeed, smaller hippocampal volumes may be a premorbid risk factor for unipolar depression (Chen et al. 2010; Serafini et al. 2014; Inal-Emiroglu et al. 2015), posttraumatic stress disorder (Bremner 2001; Mueser et al. 2002), and panic disorder (Schwartz et al. 2015).
As with the temperament findings, the degree to which variations in hippocampal morphometry reflect a temperament trait versus a psychopathology is unclear. Cortisol administration has been associated with depression-like states and neuronal atrophy in the hippocampus, leading to decreases in hippocampal volume, implicating an important link between stress hormone response, depression, and hippocampal volume (Nakagawa et al. 2002). Our group has previously demonstrated that hippocampal volume correlates with anxiety scores in youth who have already developed BD (Simeonova et al. 2009). To better delineate the separate contributions of temperament and psychopathology on hippocampal morphometry, we investigated the effect of depression and anxiety symptom severity on hippocampal volume. Importantly, neither CDRS nor MASC scores in the OBD+s group correlated with hippocampal volume, whereas trait measures of inhibited temperament did correlate with hippocampal volume, in both symptomatic and asymptomatic offspring of parents with BD. This finding is in contrast to our prior work, which is likely due to the fact that symptoms in our high-risk youth were not as severe as those in youth with BD, and were unlikely severe enough to influence temperament (Compas et al. 2004). Inhibited temperament in high-risk offspring may represent an early risk for anxiety and hippocampal atrophy, suggesting that variations in hippocampal volume are associated with temperament traits and precede rather than are a consequence of current psychiatric symptoms in youth at high risk for BD.
There are a few limitations to our study. First, this study is cross-sectional with a relatively small sample size. Information about progression toward a bipolar diagnosis among the OBD groups would verify whether inhibited temperament is an early risk marker for developing BD. Second, scans in OBD+s and OBD−s youth are acquired on two 3T GE scanners, although at the same MRI center and with their own respective control groups. Third, we used a parental report of temperament rather than a child's self-report or clinical assessment of temperament. However, several studies have found that parents can reliably assess a child's temperament (Luby and Steiner 1993), and to ensure that parental mood state did not influence this assessment, parents completed an assessment of their child's temperament during a period of euthymia. Fourth, we were underpowered to examine the effect of medication exposure to antidepressants and mood stabilizer exposure in our symptomatic OBD+s youth, which may have accounted for some variability in hippocampal morphometry in that group. Finally, FreeSurfer image analysis that we used may overestimate subcortical structures, but this overestimation will occur across all subjects and should have little impact on group-level comparative analyses. Indeed, hippocampi were visually inspected for validity by experienced raters who were previously trained to achieve an inter-rater reliability of >0.95.
Conclusion and Clinical Significance
Despite these limitations, our study suggests that youth at risk for BD are characterized by key temperament traits that are present even preceding the onset of psychiatric symptoms and may be associated with early variations in hippocampal morphometry. This line of research is important for early identification and preventive intervention in high-risk youth. Additional larger and longitudinal studies are needed to investigate mechanisms by which temperament-related risk factors contribute to the development of BD.
Although the association between hippocampus volume and inhibited temperament may not be exclusive to BD, our study found that key temperament features, such as inhibited temperament, may increase the possibility that a child may develop BD, and they may be used for identifying high-risk children, who may be followed prospectively or targeted for preventive interventions.
Footnotes
Acknowledgments
The authors gratefully acknowledge funding from the NIMH (RO1 MH077047 and K23 MH064460 to KDC and K23 MH085919 to MKS). They thank the participants who dedicated their time for this study.
Disclosures
Dr. Chang is a consultant for GlaxoSmithKline, Bristol-Myers Squibb, Merck, Actavis, and Sunovion. The other authors have nothing to disclose.