
Abstract
Objectives:
Risperidone is approved for the treatment of serious behavioral problems in children with autism spectrum disorder (ASD). This study examined the effects of risperidone on cardiac conduction in children with ASD.
Methods:
Data were collected from an 8-week, five-site trial conducted by the Research Units on Pediatric Psychopharmacology Autism Network. Children (age 5–17 years) were randomly assigned to risperidone (n = 49) or placebo (n = 52) under double-blind conditions. Risperidone was superior to placebo in reducing serious behavioral problems. A standard 12-lead, electrocardiogram (ECG) was obtained in most subjects at screening and week 8. A pediatric electrophysiologist blind to treatment assignment reviewed all available ECGs for readability, abnormalities, and cardiac conduction parameters, including QTc. The electrophysiologist measurements were compared to machine readings. A second blinded electrophysiologist examined all available ECGs for abnormalities and a 20% random sample for QTc.
Results:
Of the 101 randomized subjects in the trial, complete pretreatment and week 8 data were available on 65 subjects (placebo n = 30; risperidone n = 35). The electrophysiologist did not identify any cardiac conduction adverse effects of risperidone and there was no difference in mean change on the QTc compared to placebo. The Bland–Altman plot showed a systematic bias in QTc measurements by the electrophysiologist and machine. Machine readings produced higher values than the electrophysiologist for shorter QTc intervals and machine scoring was lower than electrophysiologist readings for longer QTc values (p = 0.001). Two electrophysiologists had overall percent agreements of 82.9% (95% CI: 76.3 to 89.6) on qualitative assessment and 88.6% (95% CI: 79.3 to 98.0) on QTc interval.
Conclusion:
Using conventional doses during acute treatment in children with ASD and serious behavioral problems, there was no difference in the mean change in QTc between risperidone and placebo. Compared to the electrophysiologist, the machine readings may miss elevated QTc measurements.
Introduction
A
Early interest in the SGAs was driven, in part, by the presumed lower risk of neuromotor adverse effects compared with the traditional antipsychotic drugs (Caroff et al. 2002). The risk of neuromotor adverse effects does indeed appear to be lower with risperidone compared with high-potency antipsychotics such as haloperidol (Sikich et al. 2003; Correll and Kane 2007). However, other SGA-related adverse events such as cardiac conduction abnormalities and weight gain have emerged as important concerns (Correll et al. 2009; Vieweg et al. 2013; Scahill et al. 2016). Concerns about cardiac conduction abnormalities such as QT prolongation with SGAs emerged in the 1990s amidst the registration trials of sertindole, which was implicated in 12 unexplained sudden deaths in adults (Karamatskos et al. 2012). A prolonged QT interval, also known as long QT syndrome (LQTS), has an estimated prevalence of 1 in 2500 adults and ∼1 in 2000 infants (Schwartz et al. 2009). The QT interval, which is measured from the beginning of the QRS complex to the end of the T wave, reflects the time of depolarization and repolarization during ventricular systole. QT prolongation increases the risk of ventricular arrhythmia and potentially fatal torsades de pointes (torsades) (Jensen et al. 2015). Because the QT is inversely related to heart rate, it is corrected for heart rate and expressed as the QTc. Commonly used approaches to QTc calculation include Fridericia or Bazett formulas. There is incomplete consensus on the defining threshold for QTc prolongation. When using the Bazett formula, most studies use 450 milliseconds, although others use 500 milliseconds (Jensen et al. 2015).
To date, few studies on the association of QTc prolongation and SGAs have focused on children. A meta-analysis of 64 randomized, double-blind trials of risperidone or paliperidone involving 11,000 adults reported one case of sudden death due to cardiovascular event in a 95-year-old woman with dementia (Gopal et al. 2013). A review of published case reports of QTc prolongation or torsades in risperidone-treated patients observed only two pediatric cases (Vieweg et al. 2013). In both cases, clear causal attribution of risperidone is equivocal due to disease state and possible drug interaction in one patient and unconventional dosing in the other (Vieweg et al. 2013). A sophisticated analysis of reports to the FDA Adverse Event Reporting System from 1997 to 2011 ranked ordered the available SGAs on the probability of prolonged QTc in children (Kimura et al. 2015). The top two in order were ziprasidone and risperidone with reporting odds ratios of 28 and 2, respectively. None of the other SGAs was significantly associated with LQTS events. The authors concluded that ziprasidone has the highest likelihood of prolonged QTc in children. Jensen et al. (2015) identified 23 clinical trials with risperidone across a range of psychiatric disorders that reported on cardiac conduction in children and adolescents. Of these, there was one open-label study of risperidone in children with ASD, and one placebo-controlled trial of aripiprazole. Across all available pediatric risperidone studies, there was a mean QTc increase from baseline of +1.68 milliseconds (CI: +0.67 to +2.70, p = 0.001), which was not significantly different from placebo. By contrast, ziprasidone had a significant mean increase in QTc (+8.74 milliseconds, CI: +5.19 to +12.30) compared to placebo (p = 0.020) (Jensen et al. 2015).
The current study used electrocardiogram (ECG) data from the placebo-controlled trial of risperidone in children with ASD conducted by the Research Units on Pediatric Psychopharmacology Autism Network (2002). In this study, we examine the effects of risperidone on QTc compared to placebo reviewed by a pediatric electrophysiologist, compare the accuracy of automated machine electrocardiographic interpretations to the pediatric electrophysiologist, and examine agreement between two pediatric electrophysiologists.
Methods
Design
The multisite, 8-week, double-blind trial randomized 101 children (82 males and 19 females; age 5–17 years) to risperidone or placebo in a 1:1 ratio between June 1999 and April 2001 (Research Units on Pediatric Psychopharmacology Autism Network 2002). The Institutional Review Board at each of the five participating sites (Indiana University, Johns Hopkins University, Ohio State University, University of California at Los Angeles, and Yale University) approved the study. Before data collection, written informed consent was obtained from a parent or guardian. The protocol was monitored through weekly conference calls by a steering committee of study investigators; annual site visits by investigators at the coordinating center (Yale University); and quarterly reviews by a data and safety monitoring board convened by the National Institute of Mental Health.
The design and primary results of the study have been reported elsewhere (Research Units on Pediatric Psychopharmacology Autism Network 2002, 2005a). Each subject received a comprehensive assessment that included medical history and physical examination, developmental and psychiatric histories, routine laboratory tests, and a 12-lead ECG (Research Units on Pediatric Psychopharmacology Autism Network 2002). Children with clinically significant findings on examination, laboratory tests, or ECG were excluded. Children with equivocal findings on these assessments were reviewed by a cross-site case panel. To be eligible for the study, the children had to meet the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) (American Psychiatric Association 2000) criteria for autistic disorder based on clinical assessment and supported by the Autism Diagnostic Interview–Revised (Lord et al. 1994). In addition, participants had to have serious behavioral problems as evidenced by a score of ≥18 on the Irritability subscale of the Aberrant Behavior Checklist (ABC) and a rating of moderate or higher on the Clinical Global Impressions—Severity (CGI-S) scale (Guy 1976; Aman et al. 1985; Brown et al. 2002). The Vineland Adaptive Behavior Scales (Vineland) were used to measure adaptive functioning (Sparrow et al. 1984). Subjects were required to be medication free with the exception of stable treatment (at least 4 weeks) with an anticonvulsant for seizure control. Furthermore, the child had to be seizure free for ≥6 months. Children with a history of psychosis, a coexisting psychiatric disorder requiring treatment (e.g., bipolar disorder, depression), IQ <35, or <15 kg of body weight were excluded.
Eligible subjects were randomized to risperidone (n = 49) or placebo (n = 52) under double-blind conditions.
The ECGs were reviewed by a pediatric cardiologist at each site. Automated machine ratings were also available. After the completion of the study, a pediatric electrophysiologist, who was blind to treatment assignment, study time point, and machine readings, reviewed all available pretreatment ECGs and those collected at the week-8 visit (or at early termination with at least 4 weeks in study). The blinded electrophysiologist reviewed ECGs for abnormalities and measured the QT interval using calipers and the Bazett equation (the cycle length of RR divided by the square root of the QT interval). The electrophysiologist interpretations were compared to machine readings on pretreatment ECGs. The machine measurements of the QT interval are based on the average QT interval from all leads. By contrast, the electrophysiologist's measurements were based solely on interpretations from the recommended leads (II or V5). A second blinded electrophysiologist reviewed all available ECGs (pre- and post-treatment) for qualitative abnormalities and a 20% random sample for QTc.
Statistical methods
Statistical analyses were conducted using SAS 9.3 (Cary, NC) and statistical significance was set at 0.05 level, unless otherwise noted. Descriptive statistics were calculated for all variables of interest using means and standard deviations (SDs) or counts and percentages, as appropriate. To determine the effect of risperidone on QTc, the change in QTc, as measured by the first electrophysiologist, was calculated from the screening visit to week 8 (or early termination) for each study participant. The change was then compared across treatment groups using two-sample t-tests. A paired t-test was used to compare the change in QTc within treatment groups. A prolonged QT interval was defined as a QTc ≥450 milliseconds. The proportion of subjects with prolonged QTc was compared between groups using a chi-square test (exact test was used when expected cell count <5%).
The prevalence of abnormal ECGs and QTc prolongations was low. Therefore, we used percent agreement between electrophysiologist and machine readings and between the readings of the two electrophysiologists with 95% confidence intervals rather than kappa. In addition, Bland–Altman plots were constructed to assess agreement on the continuous QTc measurements between the electrophysiologist and the machine. The Bland–Altman approach plots the difference between the measurements (electrophysiologist and machine) against the mean of the two methods for each subject. Bland–Altman plots graphically display the limits of agreement (i.e., whether values fall within the 95% upper and lower limits of agreement) and provide an estimate of bias for the test measure (machine readings) against the gold standard (electrophysiologist).
Results
To be included in this analysis, participants had to have a readable ECG at pretreatment and week 8 or early termination with at least 4 weeks exposure to risperidone or placebo. Of the 101 subjects in the randomized trial, 65 (n = 35 for risperidone and n = 30 for placebo) met these criteria (Fig. 1). At baseline, these 65 subjects were not significantly different on the proportion of males, participants with IQ below 70, mean age or mean scores on the ABC-I and Vineland than the 36 children who were not included in the analysis (Table 1). The demographic characteristics in the available risperidone and placebo treatment groups were well matched (Table 2). The mean age ± SD of participants was 8.7 ± 2.7 years.

Consolidated standards of reporting trials (CONSORT) diagram displaying the flowchart of electrocardiogram inclusion in the present study.
Overall chi square.
ABC, Aberrant Behavior Checklist; CGI, Clinical Global Impressions; ECG, electrocardiogram; SD, standard deviation.
Significant difference in Vineland Daily Living scale (t 61.3 = −2.03, p = 0.047).
ABC, Aberrant Behavior Checklist; CGI, Clinical Global Impressions; SD, standard deviation.
Assessment of risperidone on cardiac abnormalities and prolonged QTc
Qualitative results (normal vs. abnormal) and QTc measurements (n = 65) by the first electrophysiologist at screening and week 8 (or early termination) are presented in Table 3. Of the eight screening ECGs read as abnormal by the electrophysiologist, five (14%) were in the risperidone group and three (10%) were in the placebo group. At week 8 (or early termination), 5 ECGs of 30 (17%) in the placebo group and 10 of 35 ECGs (29%) in the risperidone group were read as abnormal by the same electrophysiologist. Four of five abnormalities in the placebo group were reported as not present at screening. In the risperidone group, 5 of the 10 abnormalities were reported as not present pretreatment. The remaining five abnormalities in the risperidone group were detected at screening and at endpoint (sinus tachycardia in four cases, right-sided ventricular hypertrophy in one). None was considered clinically significant.
Fisher exact p-value reported.
n = 64 (one subject from placebo group was missing QTc value at baseline).
Change in QTc was skewed right, a Wilcoxon rank sum test was used to compare change in QTc between groups.
n = 60 (29 placebo and 31 risperidone).
ECG, electrocardiogram; SD, standard deviation.
At screening, the mean QTc values were 404 ± 31 milliseconds and 404 ± 23 milliseconds in the placebo and risperidone groups, respectively (Table 3). From screening to week 8 (or early termination), neither group showed a statistically significant mean or median change in the QTc. At the individual level, three subjects (10%) in the placebo group and one (3%) in the risperidone group had a 60 millisecond or greater increase in the QTc compared to baseline. Using ≥450 milliseconds as the threshold, two (7%) subjects in the placebo group and one in the risperidone group (3%) had a prolonged QTc at pretreatment (range across these three subjects was 450–452 milliseconds). At week 8 (or early termination), the same two subjects and three additional subjects in the placebo group exceeded this threshold (range 450–473 milliseconds). In the risperidone group, the subject with ≥450 milliseconds at baseline had normal QTc at week 8 (QTc = 426 milliseconds); three subjects showed QTc ≥450 milliseconds at week 8 that had not been observed at screening (range 450–484 milliseconds). There was no significant difference in the percentage of new cases of prolonged QTc across treatment groups (p = 1.00).
Agreement between electrophysiologist and machine ECG readings
Sixty-four subjects had a pretreatment and week 8 (or early termination) machine and electrophysiologist ECG reading (machine reading at week 8 was missing for one subject). At screening, the machine and electrophysiologist read 55 ECGs (86%) as normal and 1 ECG (1.6%) as abnormal for an overall percent agreement of 87.5% (95% CI: 77.2 to 93.5). Seven (10.9%) machine-read normal ECGs were read as abnormal by the electrophysiologist. Although read as abnormal by the electrophysiologist, the abnormalities were not considered clinically significant. One (1.6%) machine-read abnormal ECG was read as normal by the electrophysiologist.
On the pretreatment ECGs, the machine QTc readings were 14.9 milliseconds higher on average than the electrophysiologist's (p < 0.001). The differences in the actual QTc values are presented in the Bland–Altman plot. As shown in Figure 2, most values fell within the 95% limits of agreement. Visual interpretation of the Bland–Altman plot, however, showed a systematic bias in QTc measurements by the electrophysiologist and machine. The difference (or bias) between machine and electrophysiologist QTc measurements was negatively correlated with the average of the QTc measurements for the machine and electrophysiologist (r = −0.39, 95% CI: −0.58 to −0.15, p = 0.001). The machine ECG readings were higher than the electrophysiologist's for shorter QTc intervals (e.g., <400 milliseconds). In contrast, the machine ECG readings were lower than the electrophysiologist readings for longer QTc values (e.g., values >420 milliseconds). The machine and the electrophysiologist agreed on QTc <450 milliseconds in 59 of 64 cases (92.2%) and agreed on prolonged QTc in one subject (1.6%) for an overall agreement of 93.8% (95% CI: 85.0 to 97.5). Nonetheless, the machine missed two electrophysiologist ECG readings ≥450 milliseconds. In these two cases, the electrophysiologist readings were 450 and 452 milliseconds compared to the machine reading of 373 and 422 milliseconds, respectively. The machine also incorrectly read two ECGs as ≥450 milliseconds with readings of 487 and 467 milliseconds compared to values of 412 and 440 milliseconds by the electrophysiologist.
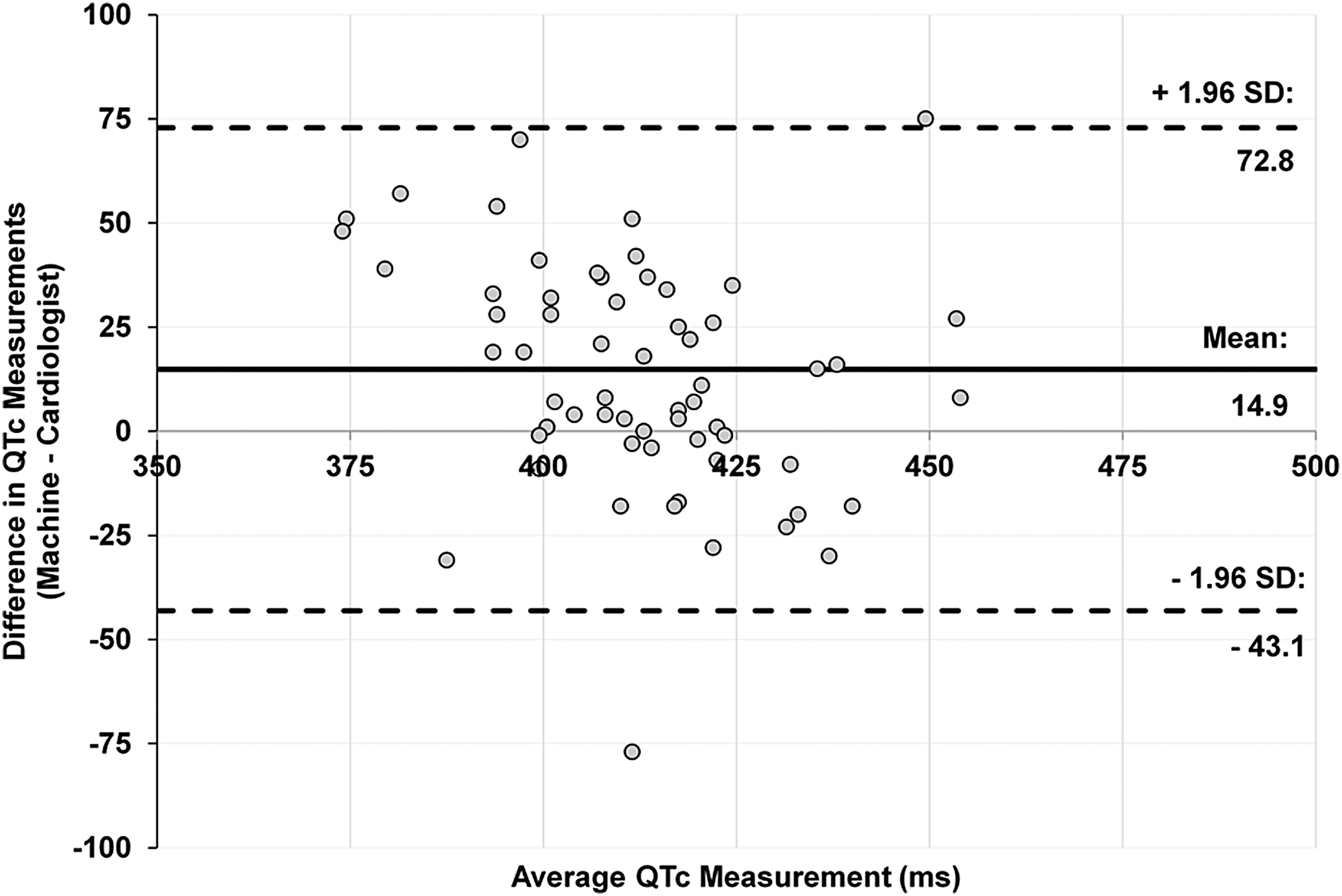
Bland–Atman plot for machine and electrophysiologist QTc measurement agreement (n = 65). There is a clear systematic bias with a negative linear correlation (r = −0.39; 95% CI: −0.58 to −0.15, p = 0.001) between the y-axis (difference between machine and electrophysiologist QTc readings) and the x-axis (average of the machine and electrophysiologist QTc measurements). If there were no systematic bias, there would be random scatter of QTc values. The difference was positive for lower QTc values, meaning the machine readings were higher than the electrophysiologist's. The difference was negative for longer QTc values, meaning the machine readings were lower than the electrophysiologist's. The machine readings misread QTc values in both directions.
Agreement between two electrophysiologists
The two electrophysiologists agreed that 61 pretreatment ECGs as well as 62 ECGs at week 8 (or early termination) were readable. Of these 123 ECGs, 89 (72.4%) were read as normal by both electrophysiologists and 13 (10.6%) ECGs were read as abnormal by both electrophysiologists. This overall percent agreement of 82.9% (95% CI: 76.3 to 89.6) on 123 ECGs is slightly lower than the percent agreement observed for the first electrophysiologist and the machine in the 64 baseline ECGs. Forty-four of the 123 available ECGs were randomly selected for QTc measurement by the second electrophysiologist. Thirty-nine of these 44 ECGs were read as normal (QTc <450 milliseconds) by both electrophysiologists for an overall agreement of 88.6% (95% CI: 79.3 to 98.0). The electrophysiologists disagreed on the QTc >450 milliseconds in five cases, with no clear pattern of disagreement. The highest measurement across the jointly read ECGs by either electrophysiologist was 454 milliseconds.
Discussion
Data from placebo-controlled trials on the cardiac conduction effects of risperidone in children with ASD are limited. Based on pediatric electrophysiologist measurement on the QTc, these results suggest that acute monotherapeutic treatment with risperidone at conventional doses has no clinically significant effect on QTc in this sample of children with ASD and serious behavioral problems. This finding is consistent in the 8-week, placebo-controlled trial with aripiprazole in children with ASD (Owen et al. 2009). In that study, there was no treatment group difference in the mean change on QTc from baseline to week 8. Three aripiprazole-treated participants exceeded QTc of 450 milliseconds using Bazett correction. Our findings are also consistent with the meta-analysis done by Jensen et al. (2015) that also showed no statistically significant change in QTc with risperidone-treated children compared to placebo. Alda et al. (2016) evaluated the effects of atypical antipsychotics (risperidone, olanzapine, or quetiapine) on QTc in an open-label study of 211 youth with various psychiatric disorders treated for 3–12 months. Of the 118 risperidone-treated subjects with ECG data at baseline, complete 1-year data were available on 34 subjects. On average, the mean QTc was slightly lower at 12 months compared to baseline. There is incomplete consensus on whether an absolute cutoff for QTc or a change in QTc from baseline is a better metric for tracking cardiac adverse events (Blair et al. 2005). In our study, there was no difference between risperidone and placebo in the percentage of subjects with a change of the QTc interval >60 milliseconds. This result is also consistent with Jensen et al. (2015).
Given the incomplete consensus on which cardiac conduction variables are reliable endpoints for predicting drug-induced torsades, there is increased interest in other variables such as QT dispersion (QTd) (Shah and Hondeghem 2005; Hondeghem 2006; Gopal et al. 2013). QTd is a general measure of ventricular recovery times and is calculated by subtracting the minimum QT interval from the maximum QT interval across ECG leads. A longitudinal epidemiological study of nearly 4000 men in Canada studied QTd and reported that heart rate and QTd predicted sudden cardiac death, but QT did not (Cuddy et al. 2009). This finding suggests that QTc prolongation probably should not be regarded as the sole predictor of cardiac events in psychopharmacological treatments (Shah and Hondeghem 2005; Hondeghem 2006; Gopal et al. 2013; Townsend and Brown 2013). To date, there are few studies that have examined the drug effects on QTd in children. In a prospective study of 60 children treated openly with risperidone or aripiprazole, there were no subjects with QTc prolongation or abnormal QTd with either drug (Germanò et al. 2014). In the current study, we did not systematically examine QTd.
In comparing machine to manual measurements, depending on the algorithm of the ECG machine or the method used in manual measurements, results can vary. Multiple studies across several machines and algorithms (Marquette Mac15 recorder, Mortara algorithm, GE Medical System's 12SL) have shown that automatic QTc readings, on average, were about 20 milliseconds longer than the QT intervals measured manually on the same ECG by different core laboratories (Pharmaceutical Research and Manufacturers of America QT Statistics Expert Working Team and Patterson 2005). Some ECG machines have difficulty determining the end of the T wave, which leads to miscalculation of the QT interval. The machines also average the QT across multiple ECG leads. By contrast, electrophysiologists most commonly use lead II for interpretation (Salvi et al. 2010). The present study found that the machine readings tended to overestimate shorter QTc and underestimate longer QTc values. The machine missed two cardiologist ECG readings of ≥450 milliseconds and read two ECGs as ≥450 milliseconds not so classified by the cardiologist.
The results of this study need to be considered in the light of several limitations. Our sample of 65 subjects with readable pretreatment and post-treatment ECGs was relatively small and the drug exposure was brief. As per protocol, these study participants had serious behavioral problems. In addition, many children with ASD exhibit sensitivity and aversion to foreign objects placed in contact with the skin. Thus, obtaining readable ECGs in this population can be challenging. Finally, children with ASD may be more vulnerable to adverse effects to psychotropic medications (Research Units on Pediatric Psychopharmacology Autism Network 2005b; Scahill et al. 2015). Taken together, the findings of the current study may not generalize to all children with ASD or the wider pediatric population.
Our results suggest that risperidone does not adversely affect cardiac conduction in children with ASD and serious behavioral problems. Nonetheless, there is continued concern about weight gain, dyslipidemia, and insulin resistance in children treated with SGA, including risperidone (De Hert et al. 2012; McClellan and Stock 2013). Our group conducted a subsequent trial of 124 children with ASD and serious behavioral problems that compared risperidone only to risperidone plus parent training. In that study we observed increased appetite, weight gain, and several adverse metabolic outcomes (Scahill et al. 2016). A 1–2-year post-treatment follow-up study of children who participated in this 8-week risperidone trial reported that 84 of the original 101 subjects were taking risperidone (Aman et al. 2015). Collectively, these findings indicate that appetite, diet, weight, waist circumference, and metabolic indices such as fasting glucose, lipids, and liver function tests warrant monitoring before and during risperidone treatment of children with ASD (Aman et al. 2015; Scahill et al. 2016).
Given the potential for rapid weight gain and adverse metabolic effects, the use of risperidone should be reserved for children with serious behavioral problems. The recent findings supporting the use of parent training in children aged 3–7 years with ASD and disruptive behavior suggest that parent training be considered first-line treatment for young children (Bearss et al. 2015).
Conclusion
In this sample of children with ASD and serious behavioral problems, there was no significant difference in the mean change in QTc from baseline to week 8 during monotherapy with risperidone compared to placebo. Noting that our study required children to be medication free, these results may not apply to children on concomitant medication—especially medications that potently inhibit CYP2D6 (Vieweg et al. 2013). Although the study showed high overall agreement on ECG readings between the electrophysiologist and machine, a systematic bias was detected in the machine reading. Compared to the electrophysiologist, the machine readings tended to overestimate shorter QTc and underestimate longer QTc values. This finding suggests that the machine readings, compared to electrophysiologist's, may miss elevated QTc measurements.
Clinical Significance
Our study supports the current clinical practice of monitoring ECG before and during risperidone treatment in children with a family history of arrhythmia, inherited QTc prolongation, sudden cardiac death, or a personal history of pre-existing heart disease, syncope, or type 1 diabetes (McNally et al. 2007; De Hert et al. 2012; McClellan and Stock 2013; Galli-Tsinopoulou et al. 2014). Children on multiple medications could be added to this list. In such cases, consultation with a pediatric electrophysiologist is recommended if treatment with risperidone is indicated. Respect for the limitations of automated machine readings is also warranted.
Footnotes
Acknowledgments
The authors acknowledge Phillip Maghen for assistance with literature search and Alexander Westphal, MD, PhD, for assistance with data compilation.
Disclosures
Dr. Arnold has received research funding from Curemark, Forest, Lilly, Neuropharm, Novartis, Noven, Shire, Supernus, and YoungLiving (as well as NIH and Autism Speaks) and has consulted with or been on advisory boards for Arbor, Gowlings, Ironshore, Neuropharm, Novartis, Noven, Organon, Otsuka, Pfizer, Roche, Seaside Therapeutics, Sigma Tau, Shire, Tris Pharma, and Waypoint and received travel support from Noven. Dr. McCracken reports receiving consultant income from Roche, Dart Neuroscience, Think Now, Inc, and Brightech International; he has received study drug from Shire and AstraZeneca. Dr. Aman has received research contracts, consulted with, served on advisory boards, or done investigator training for CogState, Inc.; Confluence Pharmaceutica; CogState Clinical Trials, Ltd.; Coronado Biosciences; Forest Research; Hoffman-La Roche; Lumos Pharma, MedAvante, Inc.; Novartis; Pfizer; ProPhase LLC; and Supernus Pharmaceuticals. Dr. Vitiello has received salary support from NIH and consultant fees from the American Physician Institute for advanced professional studies. Dr. Scahill has served as a consultant for Neuren, Coronado, Roche, MedAdvante, Bracket, and Supernus. Dr. Vo has received consultant fees from eClinicalWorks. No other authors have potential conflicts of interest to disclose.