
Abstract
Objective:
Bipolar disorder (BD) and attention-deficit/hyperactivity disorder (ADHD) have been associated with the use of cigarettes, but little is known about the impact of the subthreshold symptoms of BD or ADHD on the course of nicotine dependence. Identifying the links is essential for elucidating the pathway and supporting the development of nicotine prevention strategies for adolescents.
Methods:
Participants (n = 3322) aged 15–17 years completed the Chinese version of the ADHD Self-Report Scale and the Mood Disorder Questionnaire. The modified Fagerström Tolerance Questionnaire was completed to measure their nicotine use or dependence. Mediation analyses were performed to explore the relationship of two predictors.
Results:
The prevalence rates of cigarette smoking and nicotine dependence in this study were 14.4% and 2.3%, respectively. Male gender (odds ratio [OR] 2.30; 95% confidence interval [CI] 1.60–3.30), subclinical symptoms of ADHD (OR 1.34; 95% CI 1.04–1.71), clinical symptoms of ADHD (OR 1.69; 95% CI 1.08–2.66), and symptoms of BD (OR 1.59; 95% CI1.09 to 2.32) were associated with nicotine use. Male gender (OR 4.60; 95% CI 1.41–14.98) and symptoms of BD (OR 6.14; 95% CI 3.37–11.18), but not symptoms of ADHD, were associated with nicotine dependence. In mediation analyses, we found that the effect of ADHD symptoms was no longer significant after controlling for symptoms of BD, and the mediation ratio (PM) was 0.39.
Conclusions:
Our findings suggest that mood disturbances other than symptoms of ADHD are more likely to be a key predictor of nicotine dependence among adolescents. The conclusions may improve our understanding of the course of nicotine dependence and help to promote potential health policy for nicotine control among youths.
Introduction
S
According to the National Youth Tobacco Survey, almost 22% of adolescents in the United States use tobacco (Arrazola et al. 2014). Nearly half of them will transition to nicotine dependence over the following 20 years (Pierce and Gilpin 1996). The continuing high prevalence among adolescents implies that the strategies for tobacco control should consider the vulnerability of juveniles themselves, such as mood disturbances and attention-deficit/hyperactivity disorder (ADHD)-related behaviors (Wilens et al. 2000).
Different studies show that individuals with bipolar disorder (BD) were found to have a high prevalence rate of smoking of 40%–70%, which is double that of the general population (Lasser et al. 2000; McClave et al. 2010). The presence of BD symptoms such as unpleasant mood, irritability, depression, or hostility has already been associated with nicotine use (Mischel et al. 2014). Teenage students whose smoking escalated rapidly were more likely to have mood disturbances (Weinstein et al. 2008). Subsequent withdrawal symptoms and impaired self-regulation of emotions supported the concept that those negative reinforcements motivated adolescents toward maladaptive behavior, like turning to addictive drugs or nicotine in the developmental course of dependence (Baker et al. 2004).
ADHD is not only a developmental disorder but is also associated with prominent impairment of cognition and executive function. The relationship between dopamine deficit and cigarette use in patients with ADHD was evident in the increased dopamine signal in the striatum and the enhanced reward after the use of cigarettes (Kollins et al. 2005). Dopamine fluctuation as a result of nicotine use was also involved in the regulation effect (Wing et al. 2014). The prospectively predicted nicotine prevalence rate is doubled among adolescents with previous diagnosis of ADHD than their unaffected peers before adulthood, and rates of nicotine dependence are almost thrice as high (Lee et al. 2011). Moreover, previous studies also report that the more symptoms along the ADHD spectrum there are during the lifespan, the greater the difficulty in quitting nicotine will be (Pomerleau et al. 2003). Although the neuropathology still remains unclear, ADHD is not only a risk factor for the early initiation of tobacco use but also for progression to regular smoking and subsequent nicotine dependence (Milberger et al. 1997; Lambert and Hartsough 1998).
The studies mentioned also separately determined the relationship of ADHD and BD with nicotine use or dependence, but the natural course of BD tends to develop later than ADHD in the course of life. Previous research demonstrates that people with ADHD symptoms tend to exhibit greater problems with affect and are more likely to respond to stressful circumstances by smoking (Mitchell et al. 2012). Biederman et al. report data suggesting children with more severe problems with ADHD have more difficulties in emotional regulation, are more likely to develop BD, and tended to use nicotine earlier in the follow-up period (Biederman et al. 2009, 2012). Based on the theory of negative reinforcement, the emotional problems cannot be ignored, especially since the psychopharmacological effect of nicotine may be helpful in mood regulation (Pang et al. 2014). Thus, there is very high clinical importance in testing the hypothesis that the higher levels of mood symptoms may mediate the direct effects of ADHD symptoms on the level of nicotine dependence in adolescents. We therefore conducted a study of 3322 students from a high school in Taipei, Taiwan. Understanding the risk factors might help prevent such adolescents from developing further health or mental problems in the future.
Method
Sample
A total of 3322 students were recruited from a high school in Taipei. Respondents completed the modified Fagerström Tolerance Questionnaire (mFTQ), ADHD Self-Report Scale (ASRS), and Mood Disorder Questionnaire (MDQ). The response rate was 84.3%, and the final sample used for data analysis comprised 2799 adolescents who were 15–17 years old with a mean age of 16.43 (standard deviation = 1.1), as shown in Figure 1. All the participants and their parents provided signed informed consent before data collection. The protocol for this study was reviewed and approved by the Institutional Review Board of Tri-Service General Hospital, National Defense Medical Centre, Taipei, Taiwan.
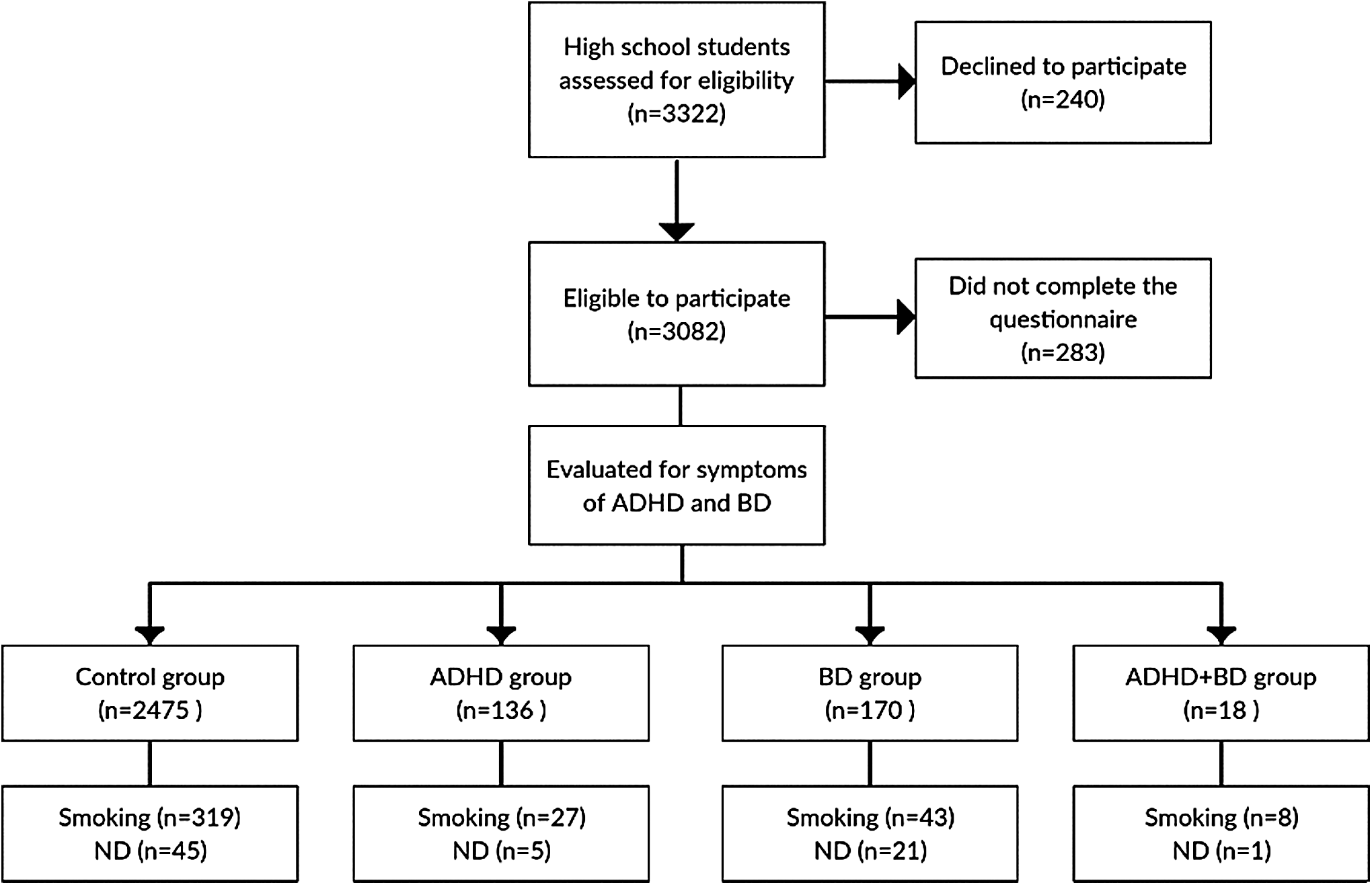
The recruitment and enrollment of participants. ADHD, attention-deficit/hyperactivity disorder; BD, bipolar disorder; ADHD + BD, the diagnosis with both ADHD and BD; ND, nicotine dependence; mFTQ, modified Fagerström Tolerance Questionnaire; ASRS, ADHD self-report scale; MDQ, Mood Disorder Questionnaire.
Modified Fagerström Tolerance Questionnaire
Current smoking behavior was categorized by the regular use of nicotine in the previous 6 months. Nicotine dependence was assessed by the modified mFTQ. The original instrument uses a five-point Likert scale for all seven items (excluding the question of “What brand of cigarettes do you smoke?”). Higher mFTQ scores indicate a greater degree of physical nicotine dependence. In the modified version, most items are coded “0” or “1,” except the questions about the amount of daily cigarette smoking and the frequency of inhalation, which are scored “0” to “2.” The mFTQ shows high sensitivity in screening adolescents who smoke (Prokhorov et al. 1998). The greatest concordance with the diagnosis in the Diagnostic and Statistical Manual of Mental Disorders—Fourth Edition (DSM-IV; American Psychiatric Association 1994) demonstrated in a previous study used a cutoff of 3 for the mFTQ (Wilens et al. 2008).
ADHD Self-Report Scale
The ASRS is an 18-item questionnaire developed in conjunction with the revision of the WHO Composite International Diagnostic Interview. This self-report is based on DSM-IV criteria and is used to screen for symptoms of ADHD over the previous 6 months. The efficacy and reliability of the Chinese version of the ASRS have also been reported in an adolescent population (Yeh et al. 2008). This questionnaire is composed of inattention and hyperactivity–impulsivity subscales, each of which contains nine items. Symptom frequency is measured on a five-point scale (0: “never,” 1: “rarely,” 2: “sometimes,” 3: “often,” and 4: “very often”). Respondents with a sum score of 24 or greater on either subscale are considered highly likely to have ADHD (described in this article as clinical ADHD). Scores of 17–23 are classified as likely to have ADHD and 0–16 are classified as unlikely (described in this article as subclinical ADHD and controls, respectively).
Mood Disorder Questionnaire
The MDQ is a self-administered questionnaire to screen for bipolar spectrum disorders. The first section of the MDQ is composed of 13 brief yes-or-no statements related to manic/hypomanic symptom items derived from DSM-IV criteria. There are also two complementary sections on symptom clusters and the severity of problems rated on a four-point scale (“none” to “severe”). The MDQ shows good sensitivity in patients with good insight, but it may be less useful in patients who overestimate their function. Therefore, we ignored the third section because of the possibility of inaccurate reporting, especially since there is little or no impairment with hypomanic episodes and subthreshold symptoms (Hardoy et al. 2005; Kim et al. 2008). To investigate all of the symptoms of BD, a respondent whose score indicated 7 or more symptom items was simultaneously classified in the BD group (first and second sections). This modification was also adopted in other research to increase the overall sensitivity without having a significant effect on specificity (Miller 2004; Yang et al. 2011).
Statistical analysis
We conducted the statistical analyses with SPSS version 19.0 (SPSS, Inc., Chicago, IL). In addition to descriptive statistics, Fisher's exact test, independent t-tests, and Chi-square tests were used to analyze the data. We used logistic regression models to estimate the risk of clinical ADHD, subclinical ADHD, or BD relative to smoking status and nicotine dependence. The results of the logistic regression analyses are shown as odds ratio (OR) with 95% confidence intervals (95% CI). Univariate and multivariate regression analyses were used to identify whether the ADHD and BD symptoms were associated with the level of nicotine dependence.
To help demonstrate the relationships (Fig. 2), the structural equation model (SEM) was used to examine the mediation effect, and standardized path coefficients were calculated using Amos 6.0 software (SPSS, Inc.). The ASRS scores were used as predictor variables (X), and the mFTQ (Y) was used as the outcome (path c). In this simple mediation model, the scores of MDQ (M) served as the mediator variable, and the mediation ratio (PM) was calculated by the ratio of indirect effects to total effects. The indirect effect of X through M can be measured as the product of a and b (ab). The total effect of X on Y (c) can be expressed as the sum of the direct and indirect effects: c = c′ + ab (MacKinnon and Dwyer 1993; Baron and Kenny 1986). To examine the mediation hypotheses, we performed the Sobel test, with|Z| > 1.96 indicating that the variable is considered a mediator (Sobel 1982).
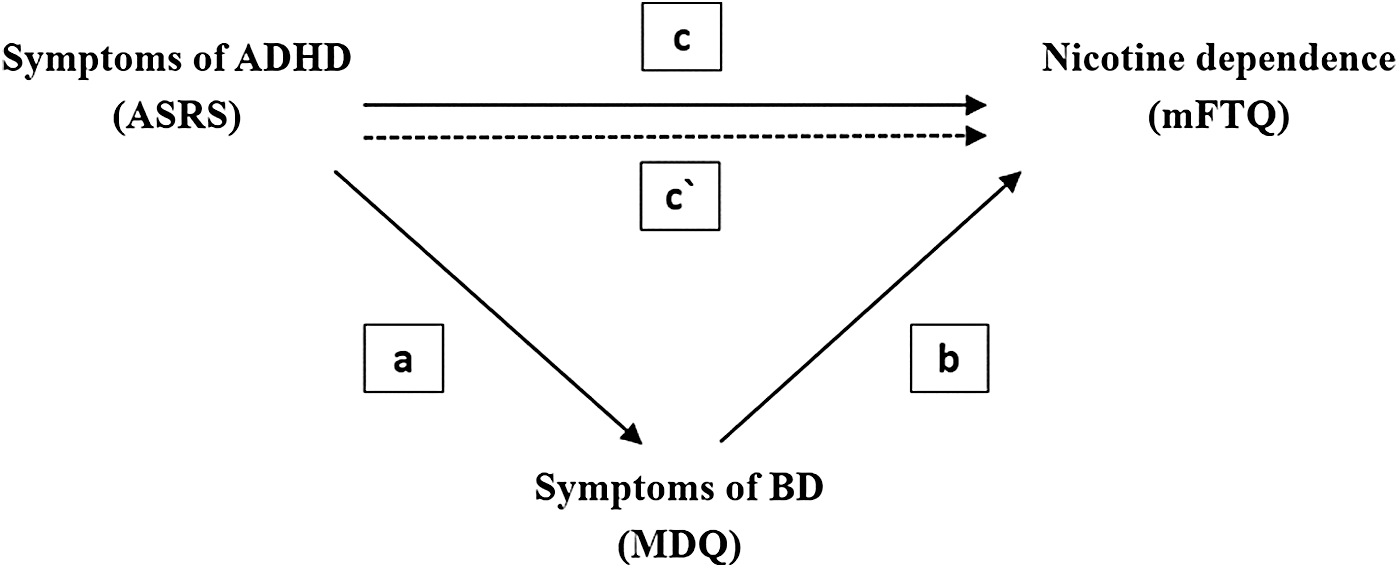
The mediation model demonstrates that symptoms of ADHD exert an indirect effect on the level of nicotine dependence through the symptoms of BD. (a) A simple model of the association between symptoms of ADHD (X) and symptoms of BD (M). (b) A simple model of the association between symptoms of BD (M) and the level of nicotine dependence (Y). (c) The simple mediation model a direct effect (ADHD symptoms [X] affect the level of nicotine dependence [Y] indirectly through BD symptoms [M]).
Results
Descriptive analyses
There were 2311 males (82.6%) and 488 females (17.4%) in the final sample. During the screening, 3.6% of the students had a family history of mental illness and 4% had ever visited a psychiatric outpatient department, but did not receive regular psychopharmacological medication. Among them, 14.4% were regular smokers and 2.3% were nicotine dependent. There were 136 subjects (4.8%) who were classified as the ADHD group (with an ASRS score higher than 17), and 170 (6.1%) were classified as the BD group. There were 18 (0.6%) subjects who met the criteria for both ADHD and BD and were classified as the comorbid group. Table 1 shows the demographic data. There was no significant difference in the gender ratio between groups (healthy controls: 82.3%, ADHD: 85.3%, bipolar: 84.1%, comorbid: 88.9%, χ2 = 1.646, p-value = 0.649). However, the mean age of the control group was slightly lower compared with the other three groups (p < 0.001).
Control group = without ADHD or BD symptoms.
ADHD group: ASRS ≥24.
BD group: MDQ ≥7 and with moderate or severe function impairment.
Current Smoker = regular nicotine use in the previous 30 days.
Nicotine dependence = mFTQ ≥3.
Post-hoc: (control < BD < ADHD + BD < ADHD).
ADHD, attention-deficit/hyperactivity disorder; BD, bipolar disorder; MDQ, Mood Disorder Questionnaire; mFTQ, modified Fagerström Tolerance Questionnaire; ASRS, ADHD self-report scale.
Logistic regression
Participants with symptoms of ADHD, BD, or comorbidity of both ADHD and BD were more likely to use cigarettes (healthy controls: 12.9% [n = 319], ADHD group: 20.3% [n = 27], BD group: 25.3% [n = 43], comorbid group: 44.4% [n = 8], p-value <0.01). Table 2 shows the risk factors for smoking. Compared to the subjects who were not current cigarette users, males smoked twice as much as females (OR 2.30, 95% CI 1.60–3.30, p-value <0.01). Having symptoms of ADHD predicted more cigarette use (subclinical ADHD: OR = 1.34, 95% CI = 1.04–1.71, p-value = 0.02; clinical ADHD: OR = 1.69, 95% CI = 1.08–2.66, p-value = 0.02). Symptoms of BD also increased the risk of smoking (OR = 1.59, 95% CI = 1.09–2.32, p-value = 0.02).
p < 0.05; ** p < 0.001.
Adjusted for child's age, family history of psychiatric illness, and substance use.
ADHD, attention-deficit/hyperactivity disorder; BD, bipolar disorder; ASRS, ADHD self-report scale; OR, odds ratio; CI, confidence interval; SE, standard error; Beta, standardized regression coefficients.
The prevalence rate of nicotine dependence also showed variation between groups (healthy controls: 1.8% [n = 45], ADHD group: 3.7% [n = 5], bipolar group: 12.3% [n = 21], comorbid group: 5.6% [n = 1]; p-value <0.01). In pairwise comparisons, the BD group had a higher rate of dependence than the ADHD and control groups, but there was no statistical difference in nicotine dependence between the ADHD and control groups. In regard to the prevalence of smoking, both male gender and symptoms of BD showed four times (OR 4.60) and six times (OR = 6.14) the risk for nicotine dependence, respectively (p-value <0.01).
Mediation analysis
SEM was conducted to test whether symptoms of ADHD and BD were associated with nicotine dependence. As shown in Figure 2, we found that symptoms of ADHD were associated with nicotine dependence (Path c: standardized coefficient = 0.107, p < 0.01), and symptoms of ADHD were associated with symptoms of BD (Path a: standardized coefficient = 0.310, p < 0.001). Moreover, symptoms of BD were also associated with nicotine dependence (Path b: standardized coefficient = 0.136, p < 0.001). The standardized direct effect of symptoms of ADHD on nicotine dependence was no longer significant after controlling for the symptoms of BD (Path c′: standardized coefficient = 0.066, p = 0.87). The mediation ratio (PM) of the symptoms of BD in the association between symptoms of ADHD and nicotine dependence was 0.39. The Sobel test also revealed that the difference was significant (Z = 2.12 > 1.96).
Discussion
The prevalence of smoking was 14.4% among adolescents in our study. This prevalence rate was lower than that in reports from the United States, where 44% of American adolescents had ever used cigarettes before the 12th grade, and one-fifth of them were current smokers (Johnston et al. 2010). In 2013, the Centers for Disease Control and Prevention (CDC) reported that 22.9% of high school students in the United States used a tobacco product, including cigarettes (12.7%) and cigars (11.9%) (Arrazola et al. 2014). The varied parenting styles, cultures, and regulations might be responsible for the differences in prevalence rates between countries (Gau et al. 2009). The rate of nicotine dependence in our study (2.3%) was lower than that in Western countries (12%–20% in the United States and 23.4% in Germany) (Kandel et al. 2005; DiFranza et al. 2010; Bogdanovica et al. 2011). This might have been due to the demographic characteristics of our sample as well as the study methodology, such as the different assessment criteria. For example, the mFTQ and DSM-IV may capture different aspects of dependence (Kandel et al. 2005).
Previous studies reported that a mood disturbance may double the risk of nicotine use and individuals with BD had high rates of being lifetime smokers (88.5%) and current smokers (69%) (Lasser et al. 2000; Waxmonsky et al. 2005; Diaz et al. 2009). The higher impulsivity associated with BD may increase the start of smoking by adolescents, and the trend remained significant after adjustment for other comorbid conditions (Heffner et al. 2012). We found that symptoms of BD could predict smoking by adolescents. Compared to attentional or motor impulsivity, mood disturbance may also predict the progression from nonsmoker to experimental smoker and regular user in the future among adolescents (Mayhew et al. 2000).
The regulatory benefit of nicotine may reduce emotional discomfort or variability and act to reinforce smoking. It has been suggested that the experience of dysregulated anger was highly correlated with the use of nicotine (Cougle et al. 2013). A former study enrolled 119 treatment-seeking adolescents for a study about motivation to smoke, and a reduction in negative effect, but not stimulation, had a strong mediating effect on anger regulation (Mischel et al. 2014). Their results also suggested that coping itself was more important for youths with affective disorders rather than the effect of the substance. Adolescence is a period of emotional volatility and immature regulatory ability; negative urgency (engaging in risky behavior when facing distress) and negative reinforcement can also explain the affective dimension of the early onset of the use of nicotine (Orlando et al. 2001; Cheetham et al. 2010).
We found that symptoms of ADHD also had a significant correlation with the current use of nicotine in this study. A meta-analysis including 27 studies with a demographic profile similar to ours (74.2% males; mean age: 18.9) indicated that children with a diagnosis of ADHD were twice as likely to use nicotine within their lifetimes (Lee et al. 2011). Several studies examined the relationship between ADHD symptoms at a nonclinical level and smoking in adolescents and found that symptoms of both inattention and hyperactivity/impulsivity significantly increased the risk of ever having smoked (Kollins et al. 2005). Young adults with symptoms of ADHD become more attentive and often experience euphoria with the first administration of nicotine (McClernon et al. 2008). This abnormality in reward salience can lead to greater levels of nicotine reinforcement and facilitate the use of nicotine in this population.
Although the severity of ADHD symptoms was an independent factor for a higher prevalence of cigarette consumption, our study implied that symptoms of BD may be crucial as well, and both symptoms tend to be more severe in adolescents as the two disorders are comorbid. Therefore, the higher percentage of smoking in this comorbid group may also be linked to a more severe presentation of the disease. To the best of our knowledge, our results were the first to show that adolescents with ADHD symptoms and comorbid BD were six times more likely to smoke than the normal control group (OR = 5.82). They also had a greater risk of smoking than the groups with symptoms of ADHD (OR = 1.25) or BD (OR = 1.51) alone. This suggests that comorbid ADHD and BD made those adolescents more vulnerable to smoking.
Our investigation was the first to show that BD symptoms had a greater impact on nicotine dependence than ADHD symptoms in adolescents. This mechanism could be multifactorial and complicated since both BP and ADHD share common risk factors, including functional neuroanatomy, candidate genes, and neurotransmitter systems (Blond et al. 2012). When individuals first smoke, positive reinforcement influences the use of nicotine, but as nicotine dependence develops, even at an early stage, the motivation for smoking progresses from positive reinforcement to negative reinforcement (Baker et al. 2004; Mathew et al. 2014). For those with symptoms of BD who self-medicate with nicotine as a coping strategy, the biological vulnerability to nicotine may soon make them dependent on it.
Previous studies found that nicotinic acetylcholine receptors were more active in BD (Picciotto et al. 2015). Single-photon emission computed tomography (SPECT) emission scans in bipolar patients also supported the idea that nicotine receptor upregulation in BD and the availability of nicotinic acetylcholine receptor (nACHR) could be biomarkers for mood disorders (Picciotto et al. 2015). Fluctuations in nicotine concentration after chronic use also influenced the dynamic equilibrium between the activation and desensitization of nicotine receptors and resulted in mood disturbances, especially withdrawal-induced agitation or depression (Picciotto et al. 2008; van Enkhuizen et al. 2014). Following a period of nicotine exposure, the upregulated receptors may elicit a negative affect that a smoker could avoid by maintaining a high nicotine level in the blood (Picciotto et al. 2008). This suggests that the behavior will be more affected in adolescents with symptoms of BD based on the neurobiological and affective model of motivation.
In line with previous studies investigating the risks of nicotine dependence, one of our novel findings was that BD symptoms were not only related to the level of nicotine dependence but also mediated the impact of the symptoms of ADHD. The manifestations of ADHD become less noticeable as children grow into adolescence, during which mood disturbances emerge significantly (Dilsaver et al. 2003). Symptoms of ADHD may be attenuated immediately since nicotine delivers rewards and reduces some of the cognitive and behavioral deficits caused by ADHD (Kollins and Adcock 2014). On the other hand, the underlying emotional problem may be induced by regular smoking because of the activation and desensitization of nicotine receptors (Picciotto et al. 2008; van Enkhuizen et al. 2014). Due to this bidirectional relationship between the use of nicotine and BD symptoms, BD becomes a more crucial factor and even a mediator between ADHD and nicotine dependence during adolescence.
Several limitations need to be considered while interpreting the results of our study. First, all outcomes were based on self-administrated questionnaires. Second, we did not collect depressive symptoms other than the bipolar symptoms for the predictive value in smoking behaviors. Third, the number of subjects with nicotine dependence was small in our study. Although 22/72 (31%) of those with nicotine dependence had BD symptoms according to self-reports, only one patient reported nicotine dependence in the comorbid group with both BD and ADHD. Therefore, it might limit the interpretation of our results in the mediational analysis due to the small number of cases of nicotine dependence. Fourth, the hypothesis of mediation focuses on the nature of two symptoms and the temporal relationship, but it is hard to confirm in our study (Biederman et al. 2009, 2012). Fifth, another limitation is that the subjects were recruited from a vocation school with much more males than females. This might limit the implications of our results in the general population, especially among female adolescents. Moreover, we did not consider potential genetic and environmental factors, including family level, socioeconomic status, or peer group affiliation, which might have influenced both the mental health and exposure to smoking behaviors. There are also different methods of analysis (MacKinnon and Dwyer 1993; MacKinnon and Fairchild 2009) for testing our model that could be in a future large-scale study with clearly defined clinical case–control to identify the mediation effect between risk factors of smoking behaviors. However, we still considered it worthwhile to report our preliminary results from the analysis of smoking behaviors of adolescents in the early stages to survey the possible risk factors. We are confident about the collection process because the rates of nicotine use and dependence were similar to those in previous national studies in this age group. Previous reports also supported the reliability and validity of these self-reports in teenagers (Kollins et al. 2005; DiFranza et al. 2007). Further study is warranted to investigate the role of symptoms of BD in the development of nicotine dependence.
Conclusions
Cigarette smoking is an important behavioral problem that often begins in adolescence and may then result in daily use after the teen years. The precise mechanisms that increase the risk of smoking have not been thoroughly elucidated. Our report demonstrated that symptoms of BD carried a stronger risk of nicotine dependence than symptoms of ADHD, but symptoms of both BD and ADHD were risk factors for nicotine use. Further studies to identify mood symptoms and provide treatment in the community are needed.
Clinical Significance
Prior research suggests that some characteristics of youths are associated with further nicotine use. Despite educational strategies and public health policy targeting the primary prevention of smoking, the prevalence of nicotine use and dependence is still high. In this study, we found that bipolar symptoms may be better predictors than ADHD for nicotine dependence and have a major role as a mediator. Secondary prevention such as campaigns to increase regular screening tests to detect mood symptoms in adolescents in the early stage of smoking may help in smoking cessation programs.
Footnotes
Disclosures
All authors disclosed that there are no financial relationships with any pharmaceutical company and this study was not supported by a pharmaceutical company. There is no conflict of interest.