
Abstract
Background:
Lisdexamfetamine (LDX) is a prodrug and consists of an active moiety, d-amphetamine, bound to lysine. Clinically, d-amphetamine becomes available postcleavage of the prodrug in the blood stream. Clinical effects of LDX in attention-deficit/hyperactivity disorder (ADHD) have been shown to persist up to 14 hours; however, pharmacokinetic (PK) data of LDX and amphetamine in ADHD adults are not currently available.
Objectives:
(1) To examine PK data of LDX and d-amphetamine in plasma and (2) to compare such PK data with Time-Sensitive ADHD Symptom Scale (TASS) ratings (PK vs. pharmacodynamic [PD]).
Methods:
Plasma d-amphetamine/LDX levels and TASS ratings were obtained immediately before morning dosing and then 0.5, 1, 2, 4, 6, 8, 10, and 12 hours postdosing in 21 adults with ADHD treated with 5 weeks of single-blind LDX up to 70 mg/day (after 1 week single-blind placebo). ADHD Rating Scale scores were obtained at the beginning of the visit, before morning dosing.
Results:
LDX levels peaked at 1.5 hours after administration (T max) and then rapidly declined (levels were negligible at 6 hours and area under the plasma concentration versus time curve, AUC = 45.9, C max = 25.0, and half-life [t 1/2] = 0.5 hours). Levels of d-amphetamine peaked at (T max) 4.4 hours and then slowly declined (AUC = 641.6, C max = 67.9, and t 1/2 = 17.0 hours). No statistically significant correlations were seen between d-amphetamine levels and TASS scores.
Conclusions:
(1) Prodrug LDX levels peaked fairly rapidly and declined, while d-amphetamine levels peaked 3 hours later than LDX levels and persisted throughout the day and (2) the absence of PK/PD correlations between PK data and TASS ratings may be due to the subjects being tested in a controlled nonattention demanding environment.
Introduction
A
Lisdexamfetamine (LDX) is a prodrug amphetamine preparation (d-amphetamine bound to lysine) and as such is inactive. After absorption in the gastrointestinal tract, it is converted to active d-amphetamine through hydrolysis in the bloodstream (Pennick 2010), which is thought to create its sustained duration of effect. LDX is FDA approved for treating adult ADHD and has a clinical duration of up to 14 hours (Adler et al. 2008, 2013), documented efficacy in adults (Weisler et al. 2014), and relatively smooth and consistent effects throughout the day (Adler et al. 2013). We previously presented results from this study comparing the clinical effects of LDX to mixed amphetamine salts (Adler et al. 2014).
To our knowledge, there have been no studies looking at the pharmacokinetic (PK) and pharmacodynamic (PD) properties of LDX adults with ADHD. However, the PKs of LDX have been studied in healthy adults, adults with schizophrenia, and children with ADHD (Krishnan and Stark 2008; Boellner et al. 2010; Ermer et al. 2013, 2015; Martin et al. 2014). The PK properties of LDX, such as C max and area under curve (AUC), are dose proportional in children with ADHD (Biederman et al. 2007a; Boellner et al. 2010), adult volunteers (Krishnan et al. 2008; Ermer et al. 2010), and subjects with schizophrenia (Martin et al. 2014). LDX has been shown to have lower interpatient variability in PK properties when compared to mixed amphetamine salts extended release in children with ADHD (Biederman et al. 2007b; Ermer et al. 2007) and in healthy adults (Ermer et al. 2010). We now present data on the PKs and PDs of LDX and its active metabolite, d-amphetamine, after 5 weeks of LDX treatment in 24 adults with ADHD.
Methods
The methods of this clinical trial were presented earlier in a study by Adler et al. (2014), which presented the clinical effects of LDX compared to those of immediate-release mixed amphetamine salts (MAS-IR), and are briefly reviewed here. Patients were recruited via local advertising and from the adult ADHD program at New York University School of Medicine. Participants were required to abstain from any ADHD medication before baseline visit, defined as visit 0 (1 week for stimulants, and 3 weeks for nonstimulants). The study was to last 14 weeks, during which the medication regimen consisted of 1 week of single-blind placebo (PBO) treatment, 5 weeks of single-blind LDX treatment, 3 weeks of single-blind PBO washout, followed by 5 weeks of open-label treatment with MAS-IR. All single-blind treatment was patient, and not investigator, blind. LDX was initiated at 30 mg/day once daily and titrated over the first 2 weeks in increments of 20 mg/day, up to a dose of 70 mg/day at the discretion of the investigator based on the clinical effects on ADHD and on side effects, and maintained at final dose for the final 3 weeks. MAS-IR was initiated at 15 mg/day (5 mg three times a day) and titrated over the first 2 weeks in increments of 15 mg/day up to a dose of 45 mg/day at the discretion of the Principal Investigator, and maintained at final dose for final 3 weeks. Adult ADHD diagnosis was established via the Adult ADHD Clinician Diagnostic Scale (ACDS v.1.2), as well as other baseline clinical examinations. ADHD symptoms were assessed at each visit via ADHD Rating Scale with adult prompts and Time-Sensitive ADHD Symptom Scale (TASS). The TASS is an 18-item scale, matching the DSM ADHD symptoms, presented in self-report form; the scale has been validated as a measure of ADHD symptoms throughout the day (Adler et al. 2011a) and has effectively measured effects of LDX (Adler et al. 2014) and mixed amphetamine salts (Adler et al. 2011b). On the final visit of the single-blind LDX treatment, plasma concentrations of LDX and LDX-derived d-amphetamine were measured at 0, 0.5, 1, 2, 4, 6, 8, 10, and 12 hours postdosing. This visit included the previously mentioned assessments, including TASS, which was used for later correlation of the symptom ratings throughout the day with plasma levels of LDX and d-amphetamine (PD). The TASS was administered before morning dosage and at 2, 4, 6, 8, 10, and 12 hours after. PK analyses included maximum plasma concentration (C max), time to C max (T max), half-life (t 1/2), and area under the plasma concentration versus time curve over one dosing interval (AUC, τ = 0–24 hours). All of the PK measures reported are the means of the measures computed for each subject. t 1/2 was computed for each subject from their peak level; the mean of these t 1/2 estimates was then reported for each group. Pearson correlations of LDX and d-amphetamine levels with TASS scores were calculated using STATA 14.0.
The study was conducted at the General Clinical Research Center at Bellevue Hospital Center (New York, NY) and was approved by the New York University Institutional Review Board and the Bellevue Hospital Institutional Review Board. The General Clinical Research Center is part of the National Institutes of Health—funded the New York University Clinical Translational Science Institute. All patients signed a written informed consent before enrollment. The study was conducted in accordance with the ethical principles originating from the Declaration of Helsinki and was consistent with good clinical practice.
Results
A total of 24 subjects completed the PK visit, with usable data for only 21 of these subjects due to non-collection of samples and inadequacy of analysis (negligible levels in one subject). The subjects ranged in age from 19 to 55 years (mean = 34.9 ± 8.2 years); 16 were men and 8 were women; 16 were Caucasian, 6 were African American, 1 was of Asian descent, and 1 was of Pacific Hawaiian descent. Seventeen participants had the combined subtype of ADHD and seven had predominantly the inattentive subtype. Most patients were titrated to a maximal allowed dose of LDX (LDX: 75.0%), the mean ± standard deviation final dose of LDX was 62.5 ± 14.2 mg/day (the dose range during the final visit for LDX was 30–70 mg/day). The mean ADHD-RS score after 5 weeks of LDX treatment was 18.24 (±11.38), with an average of 52% (±25%) decrease from baseline and with 14/21 subjects having a greater than 50% decrease. The mean total TASS morning score after 5 weeks of treatment with LDX was 23.29 (±16.99).
LDX levels peaked early postdose at about 1.5 hours (T max) and then rapidly declined to negligible levels at about 6 hours. The area under the plasma concentration versus time curve (AUC) = 45.9 ng/mL · h, C max = 25.0 ng/mL, and half-life (t 1/2) = 0.5 hours (Fig. 1). LDX-derived d-amphetamine levels peaked at 4.4 hours (T max) and then slowly declined (AUC = 641.6 ng/mL · h, C max = 67.9 ng/mL, and t 1/2 = 17.0 hours) (Fig. 1).

LDX and d-amphetamine levels in the plasma 0–12 hours (pharmacokinetic at a mean dose of 62.5 (±14.2) mg/day of LDX). LDX, lisdexamfetamine.
The average total TASS scores immediately before the morning dosage was 23.28 (±17.4) during the visit before the morning dosage, 15.6 (±25.4) at 4 hours, 15.8 (±22.7) at 8 hours, and 21.8 (±25.79) at 12 hours. Pearson correlation coefficients between TASS scores and d-amphetamine serum levels during visit 6 were not significant (r = −0.0346, ns) (Fig. 2). TASS scores were not correlated with serum LDX levels as well (r = −0.05, p = 0.058). Correlations between d-amphetamine serum levels and change in TASS scores from baseline (time 0 on visit 6) were also not significant (r = 0.03, p = 0.75).
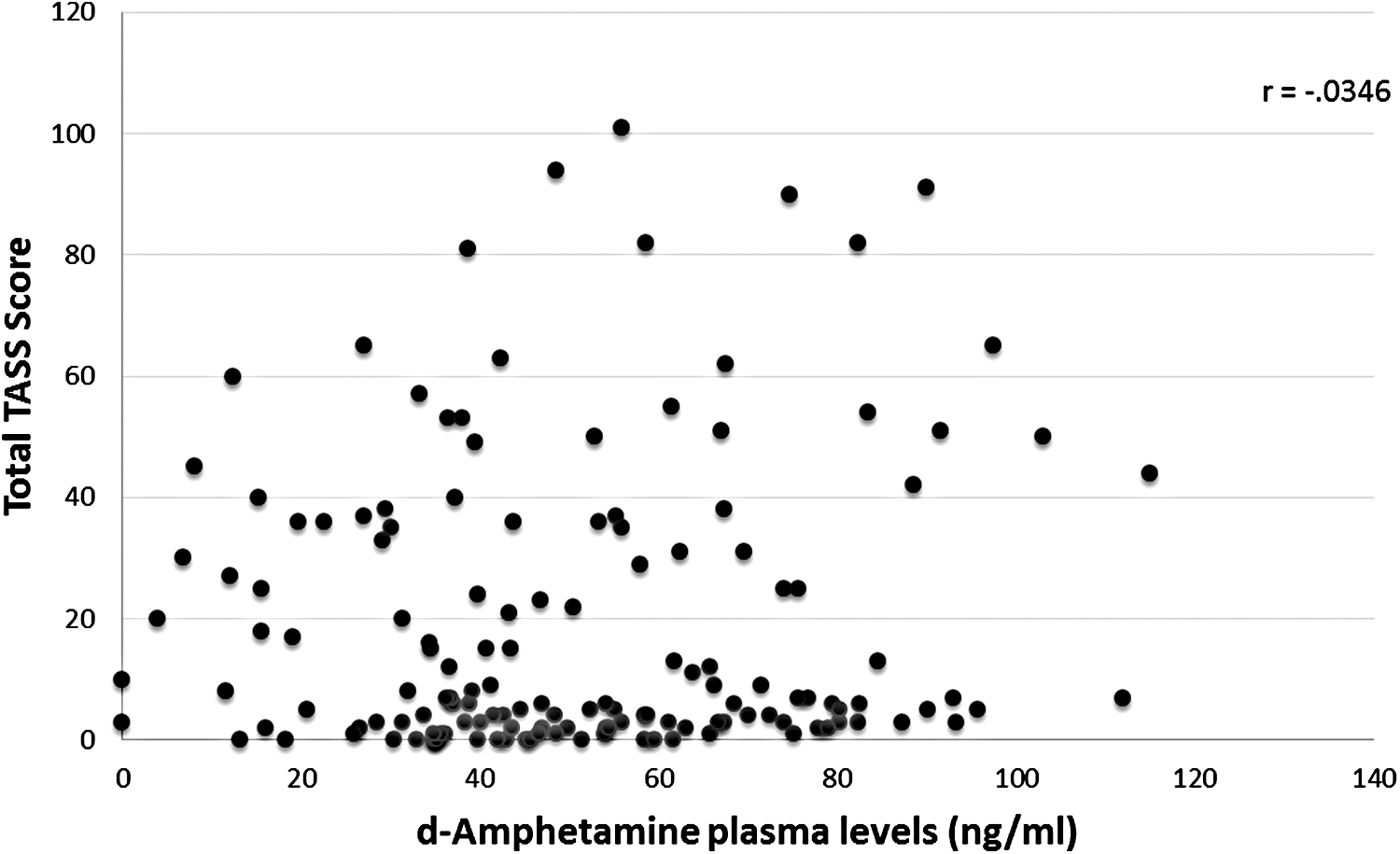
d-Amphetamine levels versus total TASS score throughout visit 6. TASS, Time-Sensitive ADHD Symptom Scale.
Discussion
As expected, levels of the prodrug LDX peaked fairly rapidly (at 1.5 hours) and then declined just as rapidly (to nondetectable levels at 6 hours), while the levels of amphetamine peaked 3 hours later (at about 4.4 hours) and persisted throughout the day (with substantial levels at 12 hours). These results are similar to those observed in children with ADHD, where the median time to C max was about 1 hour for LDX and 3.5 hours for d-amphetamine (Boellner et al. 2010), and also similar to those seen in healthy adults (1 hour and 4–6 hours, respectively) (Ermer et al. 2010). The longer t 1/2 noted for d-amphetamine after LDX administration of circa 17 hours is likely longer than prior reports of the t 1/2 of the non-prodrug form of d-amphetamine because of prodrug nature of LDX (Ermer et al. 2010).
There were no statistically significant correlations between levels of d-amphetamine and TASS scores. The TASS scores remained relatively stable throughout visit 6 (the PK visit), although at this visit they were significantly lower than those found at baseline (at Visit 0), perhaps showing a possible floor effect (where low TASS scores limited possible improvement) on the TASS correlations. The lack of correlation between plasma levels of d-amphetamine and TASS could in theory be partially due to the fact that the severity of ADHD symptoms is often situationally dependent, such that symptoms are more prominent when individuals are performing less interesting or more difficult tasks (Adler and Cohen 2004). In this trial, subjects remained in a controlled non-attention demanding environment, which could potentially distort TASS ratings, compared to prior trials involving the TASS where subjects conducted their normal day to day activities. Post-hoc analyses of data from the 15 subjects with total TASS scores greater than 10 at time 0 at visit 6 revealed no significant correlation between their TASS scores and d-amphetamine levels (r = 0.0002, ns) as well. However, there was a significant change in the TASS Inattention subscore from time 0 to 4 hours and at time 12 h (paired T-test, 0–4 hours: p = 0.003; analysis of variance 0, 4, 12 hours: F = 3.694, df = 2, p = 0.034).
After multiple dosings, plasma d-amphetamine levels remain at about 20% from the previous day's C-max and this PK analysis was conducted 5 weeks into treatment with LDX; it is not clear if the next morning presence of d-amphetamine is due to accumulation from multiple doses or secondary to the pharmacologic properties of LDX. It is likely that lower TASS scores were found the morning of visit 6 as d-amphetamine was still found in the blood stream from the previous day's dose. The post-hoc analyses seemed to detect some significant effect on TASS Inattention scores, although without a correlation to d-amphetamine plasma levels. This finding perhaps should be elucidated better in further studies. Subsequent studies can also examine PKs at specific time points throughout the day with patients performing attention demanding tasks and/or undergoing neuropsychological testing (e.g., Continuous Performance Task).
Conclusions and Clinical Significance
This study highlights to clinicians findings regarding the PKs of LDX in children to adults with ADHD. The knowledge of increasing plasma levels of the prodrug over several hours, with rapid decline and increasing plasma levels of amphetamine peaking circa 3 hours later and persisting through 12 hours after administration may be helpful to clinicians in monitoring treatment throughout the day for adults with ADHD who are receiving LDX.
Footnotes
Disclosures
Dr. L.A.A.—Grant/Research: Sunovion Pharmaceuticals, Purdue Pharmaceuticals, Enzymotec, Shire Pharmaceuticals, Theravance, Lundbeck, Department of Veterans Affairs; Consultant: Sunovion Pharmaceuticals, Enzymotec, Alcobra Pharmaceuticals, Theravance, National Football League, Major League Baseball, Rhodes Pharmaceuticals; Royalty payments (as inventor) from NYU for the license of adult ADHD scales and training materials since 2004. In the past three years, Dr. S.V.F. received income, potential income, travel expenses, and/or research support from Rhodes, Arbor, Pfizer, Ironshore, Shire, Akili Interactive Labs, CogCubed, Alcobra, VAYA Pharma, NeuroLifeSciences, and NACE. With his institution, he has U.S. patent US20130217707 A1 for the use of sodium–hydrogen exchange inhibitors in the treatment of ADHD. He is principal investigators of