
Abstract
Introduction:
Attention-deficit/hyperactivity disorder (ADHD) is one of the most prevalent neuropsychiatric disorders of childhood and adolescence. Stimulants are usually the first choice of drug; however, as many as 20% of patients do not respond to them. Stimulants may also worsen comorbid sleep, mood, and anxiety disorders, and they are associated with problems of misuse and diversion. Bupropion, a dopamine and norepinephrine reuptake inhibitor, is a promising nonstimulant alternative with reports of positive outcomes for ADHD management in both adolescent and adult populations. This study systematically reviews clinical trials on the subject.
Methods:
Using the keywords bupropion or Wellbutrin or Zyban or Elontril and attention deficit hyperactivity disorder or ADHD or ADDH, a preliminary search on the PubMed and Ovid databases yielded 25,455 articles published in English between January 1, 1988 and May 1, 2016. Of these, there were only six articles on clinical trials involving children. Full articles were also reviewed for references of interest.
Results:
All available open, controlled, and randomized trials demonstrated bupropion's efficacy in improving ADHD symptoms. The three head-to-head trials found that bupropion had efficacy comparable to methylphenidate (p > 0.05). However, a large double-blind, placebo-controlled multicenter study of bupropion found smaller effect sizes for bupropion, as quantified using teacher and parent ratings of ADHD symptoms, than methylphenidate. In terms of tolerability, a head-to-head trial found that headache was observed more frequently in the methylphenidate-treated group than in the bupropion-treated group, whereas the frequency of other side effects did not differ significantly.
Conclusion:
Current findings should be interpreted with caution because of the very limited database. Bupropion should be considered for pharmacological management of childhood and adolescent ADHD, but more randomized controlled trials with larger sample sizes are warranted. There is also some evidence of its benefits in children with comorbid ADHD and conduct, substance use, or depressive disorders.
Introduction
A
Stimulants are usually the first choice of drug; however, as many as 20% of patients do not respond to the two standard stimulants, methylphenidate and amphetamine (Forness et al. 1992). A total of 2 to 4% of children are also unable to tolerate stimulant medication because of severe side effects (Greenhill et al. 2001). Side effects of methylphenidate use include headache, nausea, vomiting, and appetite suppression (Sonuga-Barke et al. 2009). Studies have also suggested that long-term use is associated with decreased height velocity (Zhang et al. 2010). Although uncommon, stimulants may also worsen comorbid sleep, mood, and anxiety disorders (Coughlin et al. 2015), and they are associated with problems of misuse and diversion (Wilens et al. 2008). Furthermore, studies have found that many parents do express concern about “overmedicating” their child when it comes to stimulant use, and they worry about the short- and long-term side effects of stimulants (Hansen and Hansen 2006). A study examining parental attitudes and opinions also reported that the use of stimulants to treat childhood ADHD was often thought of by parents to cause dependence and predispose their child to the use of controlled substances later on in life (Lazaratou et al. 2007). For these reasons, a nonstimulant medication might be an attractive alternative.
Bupropion is a dopamine and norepinephrine reuptake inhibitor commonly indicated for depression and smoking cessation (Paul 2008). It is a promising nonstimulant alternative with several reports of positive outcomes for treatment of ADHD in both adolescent and adult populations (Cantwell 1998). Bupropion also has multiple formulations available on the market, including a relatively newer extended release formulation that lasts all day (Clayton and Stahl 2005). This study reviews published clinical trials on the subject. Some randomized, placebo-controlled, or open trials have been done to compare the efficacy and tolerability of bupropion with those of methylphenidate, but these trials often had a limited sample size. A systematic review, which has not been done hitherto, is necessary in appraising the suitability of bupropion use for ADHD in children and adolescents and generating hypotheses for further research.
Methods
Using the keywords bupropion or Wellbutrin or Zyban or Elontril and attention deficit hyperactivity disorder or ADHD or ADDH, a preliminary search on the PubMed and Ovid databases yielded 25,455 articles published in English between January 1, 1988 and May 1, 2016. Together, PubMed and Ovid covers a wide variety of databases including MEDLINE, PreMEDLINE, EBM (Evidence Based Medicine) Reviews, Cochrane Database of Systematic Reviews, and EMBASE (Excerpta Medica Database, a major biomedical and pharmaceutical database well known for its international scope). As shown in Figure 1, of the 25,455 articles, there were only 6 articles on clinical trials involving children and adolescents (i.e., up to 19 years of age). All full articles were also reviewed for references of interest.
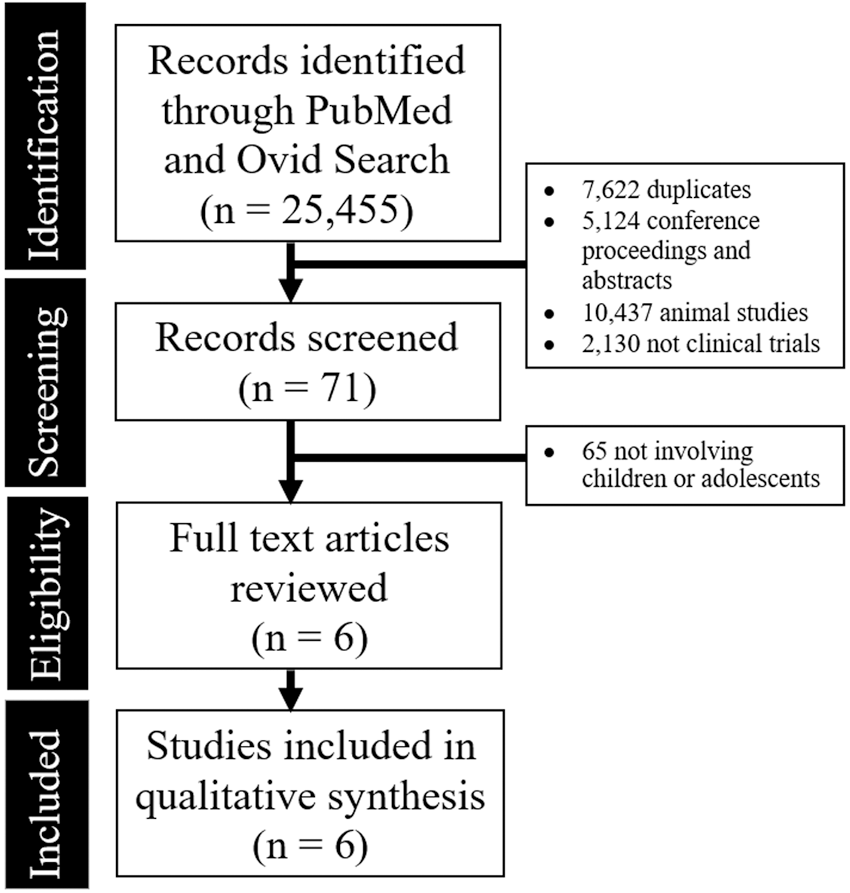
PRISMA diagram showing the studies identified during the literature search and abstraction process.
Any open, controlled, or randomized trials of bupropion conducted in children and adolescents formally diagnosed with ADHD and presenting scores of ADHD rating scales were eligible for review.
Despite best efforts, a meta-analysis was not feasible as these clinical trials had significant heterogeneity of study design and dissimilar measures. The small number of trials (and small sample size of these trials) also limited the quality and possibility of a meta-analysis.
Results
As summarized in Table 1, all available open, controlled, and randomized trials reported positive effects of bupropion in improving childhood ADHD symptoms. In general, the studies reported that bupropion had efficacy comparable to stimulants, but more studies are needed. The three head-to-head trials that compared bupropion and methylphenidate found that bupropion was equally efficacious (i.e., not significantly different, p > 0.05). However, a large double-blind, placebo-controlled multicenter study of bupropion (mean dose 3 to 6 mg/(kg·day)) including 109 children aged 6 to 12 years revealed smaller effect sizes for bupropion, as quantified using teacher and parent ratings of ADHD symptoms, than for methylphenidate (Conners et al. 1996).
ADHD, attention-deficit/hyperactivity disorder; CGI, clinical global impressions; IR, immediate release formulation; NS, formulation not specified; SR, sustained release formulation.
In terms of tolerability, most of the studies reviewed showed that bupropion was better tolerated than methylphenidate; in a head-to-head trial, headache was observed more frequently in the methylphenidate-treated group, whereas the frequency of other side effects, for example, decreased appetite did not differ significantly between the bupropion-treated and the methylphenidate-treated groups (Jafarinia et al. 2012).
Discussion
All available clinical trials support bupropion's efficacy in improving childhood ADHD symptoms. In general, bupropion appears to have efficacy comparable to stimulants, and is well tolerated, but more studies are needed. It is hard to conclusively comment on the tolerability of bupropion as compared with that of methylphenidate as limited data exist and little is known about the long-term tolerability of bupropion because the longest study duration was only 16 weeks.
Headache is a common side effect of methylphenidate that affects patient adherence to treatment (Ahmann et al. 1993). Although bupropion appears more tolerable in this regard, it is hard to assess the safety of bupropion use without quality longitudinal studies. Some studies have reported rare occurrence of serious adverse events with bupropion use, such as “serum sickness-like” reaction (Hack 2004) and seizures (Ross and Williams 2005). With the immediate release formulation, the rate of seizure is 0.4% at doses of 300 to 450 mg/day; however, the rate increases significantly at doses more than this level (Clayton and Stahl 2005). With the sustained release formulation, the rate is 0.1% at the target dose of 300 mg/day (Dunner et al. 1998). However, the occurrence of these events remains largely unpredictable.
Although bupropion is often taken to be a dopamine and norepinephrine reuptake inhibitor, it is in fact able to potentiate central nervous system activity of both dopamine and norepinephrine neurotransmitters through various other mechanisms that are still not completely understood (Ascher et al. 1995). As the etiology of ADHD seems to be the dopamine-deficit hypothesis (Swanson et al. 2007), bupropion's multipronged actions on dopamine and norepinephrine could account for its demonstrated utility in ADHD treatment. In addition, because of its unique actions, it is perhaps unsurprising that some of the trials have found bupropion beneficial in children and adolescents with comorbid ADHD and conduct, substance use (Riggs et al. 1998), or depressive disorders (Daviss et al. 2001). This further supports the role of bupropion in the management of ADHD as the incidence of comorbidity is high, for example, depressive disorders occur in 20% to 30% of ADHD patients (Michielsen et al. 2013).
Although this review focused on the comparison of bupropion and methylphenidate, the comparison of bupropion and other nonstimulant medications, for example, atomoxetine and alpha agonists would also be of interest. Atomoxetine, a popular FDA-approved nonstimulant, reported to have efficacy comparable to methylphenidate (Kratochvil et al. 2002), is associated with common side effects of anorexia, weight loss, nausea, nervousness, abdominal pain, and somnolence (Yildiz et al. 2011). There are rare but worrying reported side effects such as increased suicidality (Bangs et al. 2008) and severe liver injury (Lim et al. 2006) with atomoxetine use. However, a detailed comparison and discussion of bupropion in relation to other nonstimulants was not possible because of the paucity of data comparing bupropion and other nonstimulants. This is an area that certainly deserves further research.
The limitations of this systematic review must be addressed. Without clear patient level data, several potential confounders (e.g., intelligence quotient of the child) that may be associated with outcome of ADHD treatment cannot be accounted for. Furthermore, many of the trials involving bupropion lack a placebo group; the high response rates observed in some of these trials may, therefore, be attributed to placebo response. The generalizability of these findings may also be limited by the fact that the study subjects in the synthesized trials were of the combined ADHD subtype, it remains to be demonstrated that the three ADHD subtypes defined in Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) are in fact facets of the same condition. Data on the etiology and treatment of the inattentive and hyperactive-impulsive subtypes are still major research deficits today (Woo and Rey 2005). However, the studies reviewed did show improvement in neurocognitive parameters such as sustained and selective attention and memory retrieval with bupropion use, which may extend to all ADHD subtypes.
This study is also limited by being a single-author review, but utmost efforts have been made to ensure accuracy and fidelity of study selection, data extraction, analysis, and interpretation. An extensive range of databases have also been included in the literature search process.
Conclusion
Given current best evidence, bupropion may be efficacious and well tolerated in children and adolescents with ADHD. However, current findings should be interpreted with caution because of the very limited database. As a nonstimulant alternative to methylphenidate, bupropion should be considered for use in the management of childhood and adolescent ADHD. There is also some evidence of its benefits in children with comorbid conduct, substance use, or depressive disorders. More randomized controlled trials with larger sample sizes and involving clinically relevant subjects with comorbid depressive disorders are warranted. Future research should also compare the efficacy and tolerability of bupropion with those of other nonstimulant medications such as atomoxetine or alpha agonists, as there is scarce literature on the topic.
Clinical Significance
The search for nonstimulant alternatives for the management of ADHD in children is ongoing. As many as 20% of patients do not respond to stimulants, and stimulants may also worsen comorbid sleep, mood, and anxiety disorders and lead to problems of misuse and diversion. This is the first systematic review on the use of bupropion for the management of child and adolescent ADHD. A thorough review of available trials found that among children with ADHD, bupropion appears to have clinical efficacy and tolerability comparable to methylphenidate, but more studies are needed. As a nonstimulant alternative, bupropion should be considered for pharmacological management of childhood and adolescent ADHD. There is also some evidence of its benefits in children with comorbid ADHD and conduct, substance use, or depressive disorders. However, current findings are based on a very limited database and require further research. Directions for future research include more randomized controlled trials with larger sample sizes and a detailed comparison of bupropion with other nonstimulants such as atomoxetine and alpha agonists.
Footnotes
Disclosures
No competing financial interests exist.