
Abstract
Objective:
The aims of this study were (1) to assess obsessive-compulsive symptoms (OCS) dimensionally in a school-aged community sample and to correlate them with clinical and demographical variables; (2) to determine a subgroup with significant OCS (“at-risk for OCD”) using the Child Behavior Checklist (CBCL-OCS) and (3) to compare it with the rest of the sample; (4) To review the CBCL-OCS subscale properties as a screening tool for pediatric OCD.
Methods:
Data from the Brazilian High Risk Cohort were analyzed. The presence and severity of OCS were assessed through the CBCL-OCS subscale. DSM-IV psychiatric diagnoses were obtained by the Developmental and Well-Being Assessment. Behavioral problems were assessed using the Strengths and Difficulties Questionnaire, the Youth Strengths Inventory, and the CBCL internalizing and externalizing behavior subscales.
Results:
A total of 2512 (mean age: 8.86 ± 1.84 years; 55.0% male) children were included. Moderate correlations were found between OCS severity and functional impairment (r = 0.36, p < 0.001). Children with higher levels of OCS had higher rates of psychiatric comorbidity and behavioral problems (p < 0.001). A score of 5 or higher in the CBCL-OCS scale determined an “at-risk for OCD” subgroup, comprising 9.7% of the sample (n = 244), with behavioral patterns and psychiatric comorbidities (e.g., tics [odds ratios, OR = 6.41, p < 0.001]), anxiety disorders grouped [OR = 3.68, p < 0.001] and depressive disorders [OR = 3.0, p < 0.001] very similar to those described in OCD. Sensitivity, specificity, positive predictive value, and negative predictive value of the CBCL-OCS for OCD diagnosis were, respectively, 48%, 91.5%; 15.1%, and 98.2%.
Conclusions:
The dimensional approach suggests that the presence of OCS in children is associated with higher rates of comorbidity, behavioral problems, and impairment. The “at-risk for OCD” group defined by the CBCL revealed a group of patients phenotypically similar to full blown OCD.
Introduction
T
Moreover, longitudinal studies suggest that OCS can persist over time (Fullana et al. 2009) and increase the risk of developing OCD (Black and Gaffney 2008; Fullana et al. 2009), which supports a dimensional approach during evaluation.
Notwithstanding, only a small number of studies have assessed the presence of OCS in juvenile populations and the findings are not consistent across studies. For example, the reported prevalence rates of OCS range between 2% (Flament et al. 1988; Brynska and Wolanczyk 2005) and 19% (Valleni-Basile et al. 1994; Vivan Ade et al. 2014; Alvarenga et al. 2015), although most studies report a prevalence of ∼10% (Fullana et al. 2009; Mahfouz et al. 2009; Shams et al. 2011; Canals et al. 2012). Results on gender distribution are also inconclusive (Fontenelle and Hasler 2008). Most studies point out equal distribution between boys and girls (Zohar et al. 1992; Apter et al. 1996; Essau et al. 2000), but two studies reported OCS as more prevalent among girls (Brynska and Wolanczyk 2005; Vivan Ade et al. 2014) whereas two others found OCS being more common in boys (Canals et al. 2012; Jaisoorya et al. 2015). Regarding psychiatric comorbidity, the most frequently co-occurring conditions are major depression, anxiety disorders, tics, Tourette syndrome, and attention-deficit/hyperactivity disorder (ADHD) (Zohar et al. 1992; Heyman et al. 2001; Peterson et al. 2001; de Mathis et al. 2008; Shams et al. 2011; Canals et al. 2012; Lebowitz et al. 2012; Vivan Ade et al. 2014; Ortiz et al. 2015). The prevalence of overall comorbid conditions reported in juvenile OCS/OCD samples vary from 56% to 91% (Shams et al. 2011; Lebowitz et al. 2012; Vivan Ade et al. 2014). Concerning intelligence, one study showed no association between OCD and IQ levels (Douglass et al. 1995). In contrast, two other studies reported an association of OCS with lower IQs and lower global cognitive functioning (Zohar et al. 1992; Heyman et al. 2001) and another study did find that the OCD cases had a higher IQ (Peterson et al. 2001). In terms of the longitudinal course, most studies indicate that OCS increase with age (Apter et al. 1996; Heyman et al. 2001; Fullana et al. 2009).
Many of these inconsistencies are probably due to the diverse populations studied and to the different methodological approaches used to perform the diagnostic evaluation. Most of these studies consider OCS as a category (Apter et al. 1996; Mahfouz et al. 2009; Vivan Ade et al. 2014; Alvarenga et al. 2015), whereas a dimensional approach could be more informative, since obsessive-compulsive phenomena are expressed as a continuum from normal development to severe symptoms (Fontenelle and Hasler 2008).
The Child Behavior Checklist (CBCL) subscale for OCD (Nelson et al. 2001) is an internationally validated instrument that allows OCD and other pediatric psychiatric disorders to be dimensionally assessed. Huzdiak et al. (2006) had shown the CBCL to be a valid screening tool for OCD, with moderate sensitivity (75.3%–84.9%) and high specificity (82.2%–92.5%). Moreover, scores on the CBCL were found to have a positive predictive value (PPV) of OCD diagnosis based on Diagnostic and Statistical Manual of Mental Disorders, Third Edition Revised (DSM-IV) (American Psychiatric Association 1987) criteria (PPV) ranging between 70.5% and 83.3% and a negative predictive value (NPV), between 88.2% and 91.6%.
This study has four main objectives: (1) To study the OCS distribution viewed from a dimensional perspective in a large community (nonclinical) pediatric sample using the CBCL; (2) To assess the association of OCS with demographic (gender, age, and socioeconomic status) and clinical variables (IQ and other behavioral problems); (3) To stratify our sample into at-risk for OCD based on the CBCL cutoff (Hudziak et al. 2006) and unaffected controls; to compare at-risk versus unaffected control groups regarding demographic (gender, age, and socioeconomic status) and clinical variables (psychiatric comorbidities, IQ, and other behavioral problems); and (4) To reassess the psychometric properties of the CBCL-OCS as screening instrument for OCD, comparing with our previous sample of OCD defined by Developmental and Well-Being Assessment (DAWBA) with DSM-IV criteria.
Materials and Methods
Participants and data collection
Participants were 2512 school-aged children ranging from 6 to 12 years from a large community school-based cohort from the National Institute of Developmental Psychiatry (INPD) (
Clinical assessment and instruments
Socioeconomic status
It was stratified into five classes from A (higher) to E (lower), according to a Brazilian classification system (Jannuzzi and Baeninger 1996).
Psychiatric diagnoses
They were obtained using the Brazilian Portuguese version of the DAWBA (Goodman et al. 2000), based on DSM-IV criteria. The DAWBA is validated in Brazil and can be administered by lay interviewers. Diagnoses were rated by two senior child psychiatrists. For OCD diagnosis we used the DAWBA and the DSM-IV criteria.
Global functioning
The Strengths and Difficulties Questionnaire (SDQ), Youth Strengths Inventory (YSI), and the Social Aptitude Scale (SAS) were used to evaluate, respectively, the functional impairment, positive attributes, and social abilities.
The SDQ is a 25-item questionnaire with five symptom subscales: Emotional, hyperactivity, conduct, social, and pro-social (Goodman 1999). The SDQ impact scores were used to evaluate functional impairment, burden, and social distress. The YSI is a 24-item scale designed to assess the child's positive attributes divided in two blocks of questions; the first block consists of characteristics of the child (e.g., “responsible, grateful”) while the second block accesses the child's attitudes that pleases the caregiver (e.g., “helps around at home,” “polite”) (Vidal-Ribas et al. 2015). The SAS is a 10-item scale designed to evaluate the individual's social abilities (Liddle et al. 2009).
Cognitive skills measurement
We assessed the estimated global IQ using the vocabulary and block design subtests of the Weschler Intelligence Scale for Children, 3rd edition–WISC-III (Wechsler 2002), the Tellegen and Briggs method (Tellegen and Briggs 1967), and Brazilian norms (Figueiredo 2001; do Nascimento 2002).
Behavioral problems
The CBCL (Achenbach 1991) is a dimensional instrument, one of the most widely used measures to evaluate behavioral problems. It has been validated in Brazil (Bordin et al. 2013) and includes a total score and several subscales. In this study we focused on the internalizing and externalizing behavior scores as well as the total score. OCS were quantified using the scale proposed by Nelson et al. (2001), which consists of eight items from the CBCL, with scores varying from 0 to 16. To define the at-risk for OCD group a cutoff point of 5 was used based on the work of Huzdiak et al. (2006).
Statistics
The correlations between OCS and the dimensional variables were estimated nonparametrically using the Spearman's test. To calculate the p-values of the quantitative variables, the Mann–Whitney's test was used. The Fisher's test was used to calculate the association between the categorical variables and the control or at-risk for OCD groups. To estimate the odds ratios (OR), we used a multiple logistic regression (LR) model. The variable selection was performed by the stepwise method with the Akaike's criterion. The normality of the data was verified by the Anderson–Darling test with a significance level of 0.05. All analyses were conducted in the R3.1.3 program.
Ethics
This study was approved by the Ethics Committee of the University of São Paulo School of Medicine and all parents provided their written consent.
Results
OCS distribution
The OCS distribution among the 2512 children was calculated according to scores on the CBCL-OCS subscale varying from 0 to 16. The highest score in our study was 14. Frequencies of each score are shown in Figure 1.
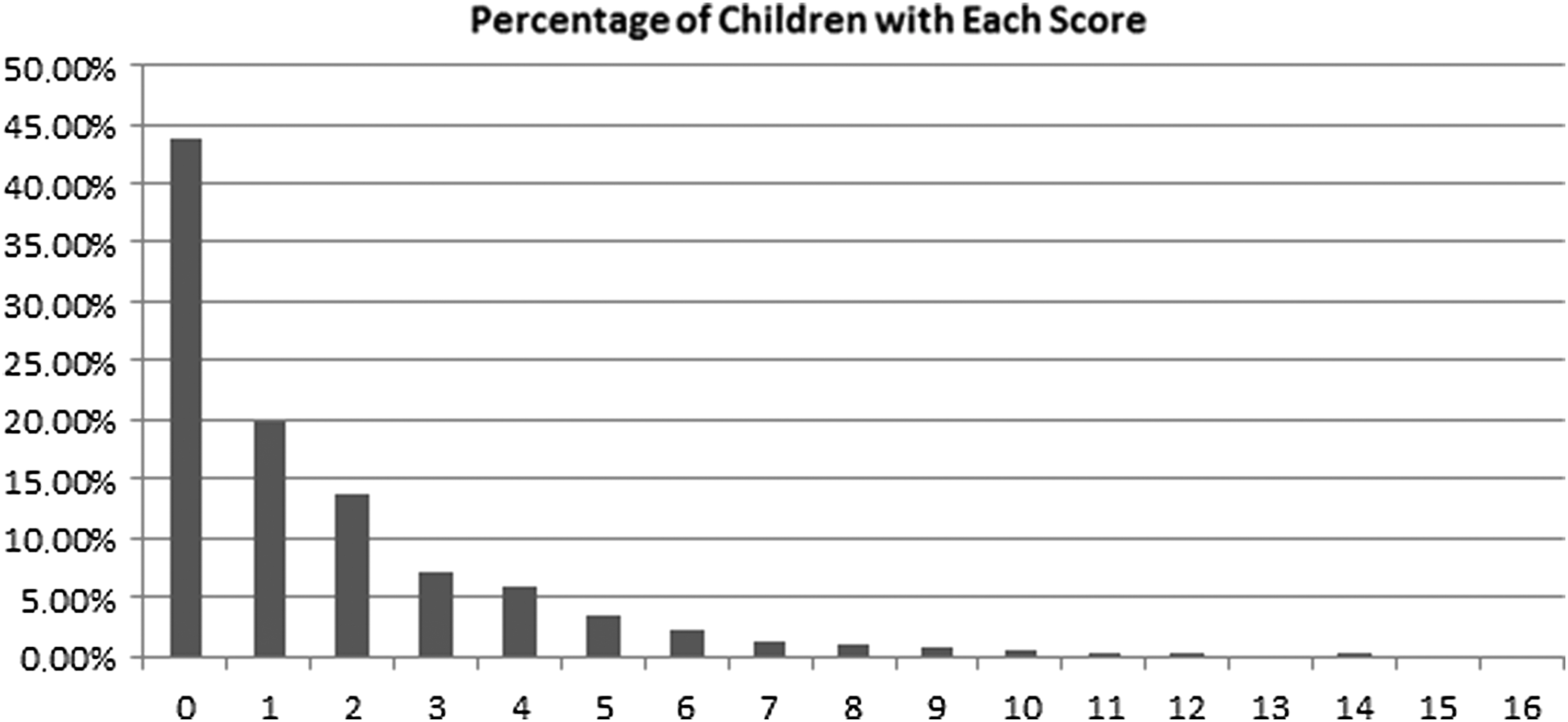
Distribution of CBCL-OCS Scores among 2512 school-aged children. x-axis: Score on the CBCL-OCS; y-axis: Percentage of children (total = 2512) with each score. CBCL-OCS, Child Behavior Checklist–Obsessive-Compulsive Subscale.
Dimensional perspective: correlation of quantity of OCS with sociodemographic and clinical variables
The correlations of demographic and clinical variables with the OCS are presented in Table 1. There were no significant correlations between gender, socioeconomic status, or IQ with the quantity/severity of the OCS. On the other hand, the severity of OCS was slightly associated with age, and moderate to strong positive correlations were found between the severity of OCS and total, internalizing and externalizing behavior scores on the CBCL. Furthermore, moderate correlations between the SDQ impairment scores and the severity of OCS were found. In contrast, we found that OCS ratings were inversely correlated with the child's positive attributes as assessed by the YSI and their social aptitude (SAS).
CBCL-OCS criteria by Nelson et al. (2001): Score ranging from 0 to 14.
Socioeconomic status: Brazilian classification that categorizes families in five classes (A–E) according to educational level and income; CBCL: Child Behavior Checklist; CBCL total: Total score on CBCL; externalizing behavior: Score on CBCL externalizing behavior dimension; internalizing behavior: Score on CBCL internalizing behavior dimension; functional impairment: Scores on the SDQ impact session; positive attributes: Measured by scores on YSI; social abilities: Measured by scores on SAS.
OCS, obsessive-compulsive symptoms; SAS, Social Aptitude Scale; SDQ, Strengths and Difficulties Questionnaire; YSI, Youth Strengths Inventory.
Comparison of at-risk for OCD group versus unaffected controls
Two hundred forty-four children (9.7% of the total sample) scored 5 or more on the CBCL-OCS subscale and were identified as being at-risk for OCD. The remainder of the children (n = 2268) were considered unaffected controls. Table 2 shows the mean scores and standard deviations on different clinical sociodemographic and clinical variables for these two groups. There were significant differences in the CBCL total, internalizing and externalizing scores between the at-risk for OCD group and the unaffected controls, with the at-risk for OCD group presenting higher scores on all measures. On the measure of functional impairment, the SDQ impact score, there were also significant differences between groups, with the at-risk for OCD group also presenting a higher score. On the Social Aptitudes Scale and the YSI the at-risk for OCD group presented significantly lower scores as well. There were no significant differences between groups regarding gender, socioeconomic status, and age.
Socioeconomic status: Brazilian classification that categorizes families in five classes (A–E) according to educational level and income; CBCL: Child Behavior Checklist; CBCL total: Total score on CBCL; externalizing behavior: Score on CBCL externalizing behavior dimension; internalizing behavior: Score on CBCL internalizing behavior dimension; functional impairment: Scores on the SDQ impact session; positive attributes: Measured by scores on YSI; social abilities: Measured by scores on SAS.
OCD, obsessive-compulsive disorder; SAS, Social Aptitude Scale; SDQ, Strengths and Difficulties Questionnaire; YSI, Youth Strengths Inventory.
The at-risk for OCD group had higher ORs for each of the assessed psychiatric conditions as compared to the unaffected control group (Table 3): Anxiety disorders as a group, separation anxiety, panic disorder and generalized anxiety, and major depression (ORs higher than nine times of being present in the at-risk for OCD group). Eating disorders, Tic disorders, conduct disorder and social phobia, oppositional defiant disorder, and ADHD were also more likely to occur in the at-risk for OCD group (Table 3).
At-risk for OCD group: Determined by cutoff score 5 on OCS-CBCL; GAD: generalized anxiety disorder; MDD: major depressive disorder; ADHD: attention-deficit/hyperactivity disorder; ODD: Oppositional defiant disorder; others: Includes pervasive developmental disorder, stereotypic behavior, psychosis, and selective mutism grouped.
CI, confidence interval; OCD, obsessive-compulsive disorder; OR, odds ratios.
LR was modeled to discriminate which impact variables or comorbidities were more strongly associated with the at-risk for OCD group (Table 4). Tic disorder (OR: 6.41, 95% confidence interval [CI]: 2.12–19.38), anxiety disorders as a group (OR: 3.68, 95% CI: 2.51–5.41), major depressive disorder (OR: 3.00, 95% CI: 1.65–5.47), and disorders with lower prevalence such as psychotic disorders, autism, and selective mutism grouped (OR: 4.12, 95% CI: 1.32–12.85) were strongly associated with the at-risk for OCD group. There was also a small, but significant, association of SDQ scores and externalizing behavior measured by the CBCL externalizing behavior subscale score (without the diagnosis of ADHD or any disruptive behavior disorder) with the at-risk for OCD group.
Anxiety disorders: Includes separation anxiety, social and specific phobia, generalized anxiety and panic disorder and agoraphobia; MDD: Major depressive disorder; Other (grouped): Includes psychotic disorders, pervasive developmental disorder, selective mutism; functional impairment: Measured by SDQ impact session; CBCL ext: Child Behavior Checklist Externalizing Behavior Dimension.
CI, confidence interval; OR, odds ratios; SDQ, Strengths and Difficulties Questionnaire.
Comparison of OCS-CBCL scores and DAWBA OCD section scores
Finally, we compared the at-risk for OCD group according to the CBCL (scores equal and above cutoff of 5) with the OCD and control groups defined in our previous work using the DSM-IV criteria and the DAWBA (Alvarenga et al. 2015) (Fig. 2). In this analysis, of the 2512 children, we obtained 77 children diagnosed with OCD. Sensitivity, specificity, PPV, and NPV of the CBCL-OCS with the cutoff of 5 were calculated. Results were as follows: sensitivity: 48%, specificity: 91.5% PPV: 15.1%, and NPV: 98.2%.
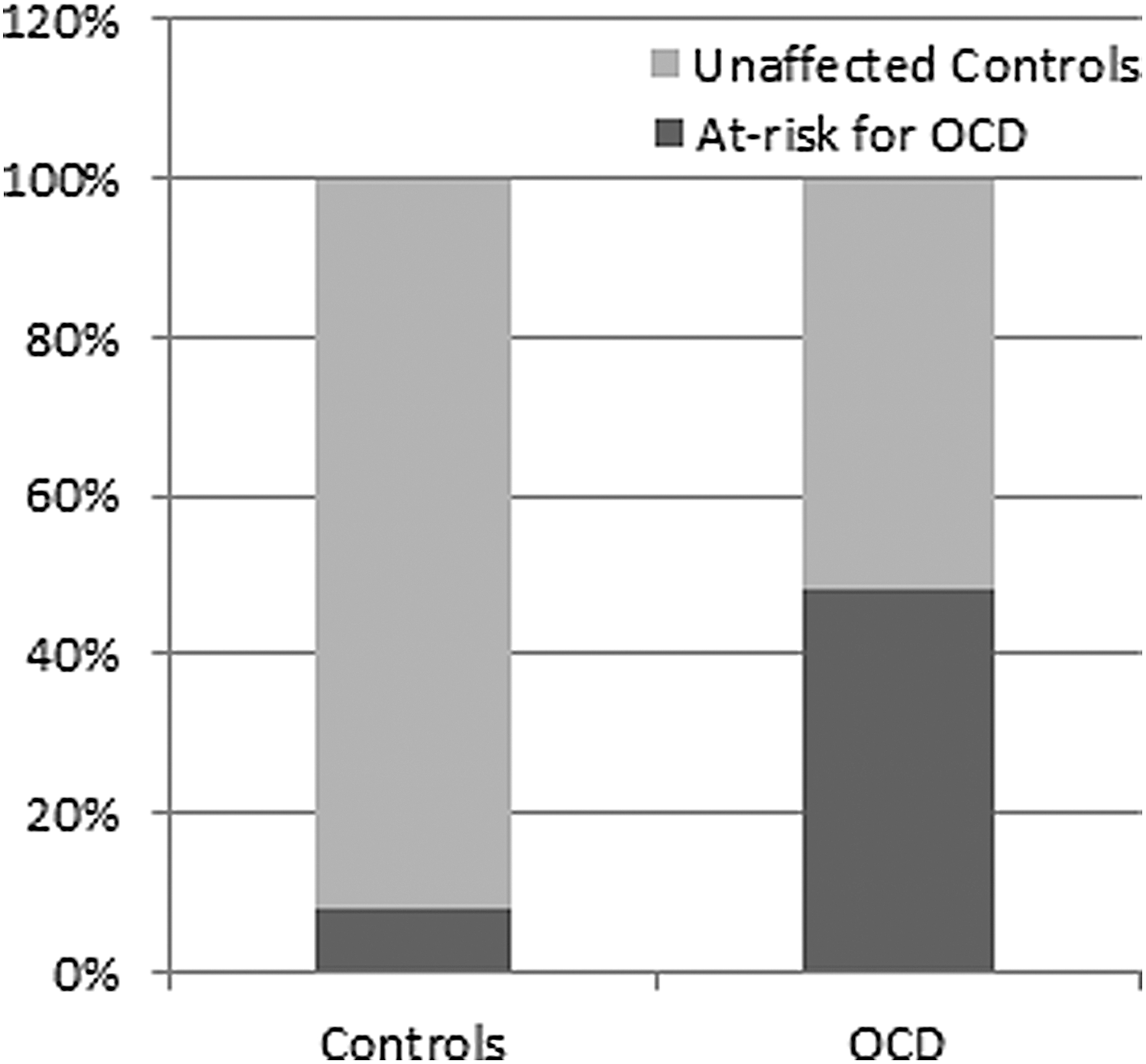
Percentage of at-risk for OCD using the CBCL in the OCD and control groups according to DSM-IV criteria using the DAWBA. x-axis: Control and OCD according to DSM-IV criteria using the DAWBA. y-axis: Percentage of at-risk for OCD according to the CBCL in each group. CBCL, Child Behavior Checklist; DAWBA, Developmental and Well-Being Assessment; OCD, obsessive-compulsive disorder.
Discussion
To our knowledge, this is the first study to address the OCS in youth population using a dimensional approach. The OCS distribution among the studied population follows a convex downward curve, as expected. Our results indicated that the severity of OCS did not differ between genders and it is (slightly) associated with increasing age. This is in agreement with most of the previous studies (Zohar et al. 1992; Valleni-Basile et al. 1994; Essau et al. 2000; Heyman et al. 2001; Shams et al. 2011; Canals et al. 2012), but in contrast to others that reported a discrete higher prevalence of OCS in boys (Flament et al. 1988; Alvarenga et al. 2015) and to other studies that suggested higher rates of OCS in girls (Brynska and Wolanczyk 2005; Vivan Ade et al. 2014).
There were nonsignificant correlations between OCS and socioeconomic status. This finding is consistent with most epidemiological studies of OCS in pediatric populations (Flament et al. 1988; Douglass et al. 1995; Brynska and Wolanczyk 2005; Shams et al. 2011; Jaisoorya et al. 2015), although there are studies that associate OCS with lower socioeconomic status (Heyman et al. 2001; Voltas et al. 2014). Likewise, we found no correlation between global IQ and OCS. These data are in line with findings from studies by Douglass et al. (1995), but not others (Zohar et al. 1992; Heyman et al. 2001; Peterson et al. 2001; Grisham et al. 2011). The dimensional approach allows the conclusion that IQ is not related to the severity of OCS, which may explain some of the inconsistencies in the previous literature data.
On the other hand, OCS severity was moderately correlated to functional impairment, as well as to internalizing and externalizing behaviors. This was an expected result that supports the idea of a continuum between mild OC symptoms and low impairment in contrast to severe OC symptoms and high functional impairment (Apter et al. 1996; Fontenelle and Hasler 2008). The analysis of positive attributes and social aptitudes showed negative correlations, also expected, but surprisingly, mild correlations. These results is in accordance to Grisham et al. (2011) who reported that social isolation and internalizing and conduct problems in childhood predicted later OCD.
The prevalence of children with significant OCS or at-risk for OCD was 9.7% using the criteria of the CBCL-OCD subscale (5 or more OCS) (Nelson et al. 2001; Hudziak et al. 2006). These data are in accordance with prevalence rates reported in four different studies (Apter et al. 1996; Fullana et al. 2009; Shams et al. 2011; Canals et al. 2012) but differed from others (Flament et al. 1988; Zohar et al. 1992; Valleni-Basile et al. 1994; Mahfouz et al. 2009; Vivan Ade et al. 2014). The differences in OCS prevalence rates may have been due to different methodological approaches.
The at-risk for OCD group had several internalizing, externalizing, and social behavior problems compared to the unaffected control group. This finding meets with studies on the most recent literature that emphasize the pathological and maladaptive features of OCS, instead of the normal or adaptive aspects of OCS (Fullana et al. 2009; Canals et al. 2012; Alvarenga et al. 2015). The at-risk group was also at increased risk for generalized anxiety, major depression, separation anxiety, and tic disorder.
The more robust analysis (LR model) indicated that tic disorder, anxiety disorders grouped, and depression were strongly associated with the presence of OCS. These comorbidities resemble the pattern reported in full-blown pediatric OCD (Flament et al. 1988; Zohar et al. 1992; Heyman et al. 2001; de Mathis et al. 2008; 2013; Shams et al. 2011; Canals et al. 2012; Vivan Ade et al. 2014; Voltas et al. 2014; Ortiz et al. 2015). OCS were significantly associated with functional impairment even when controlled by the pattern of comorbidities When considering the positive attributes and social aptitude, no associations were found. This is probably because the presence of psychiatric comorbidity has a synergistic action worsening the functional impairment already caused by the OCS. This information is relevant, since not only full blown OCD, but “just OCS” (Pauls et al. 1995) are commonly associated with other psychiatric disorders in children. In the present report, 61% of the at-risk for OCD group showed, at least, one psychiatric comorbidity, which is in accordance with earlier studies (Heyman et al. 2001; Shams et al. 2011; Canals et al. 2012; Vivan Ade et al. 2014). Interestingly, not only internalizing behavior, but also externalizing behavior was associated with OCS. The role of externalizing behaviors in OCS has been recently emphasized in the literature (Grisham et al. 2011; Lebowitz et al. 2011; Alvarenga et al. 2015). Coercive behavior was positively correlated to OCS severity, as it is used to impose family accommodation (Geller et al. 1996; Peris et al. 2008; Lebowitz et al. 2011).
Finally, the proposed model of screening using CBCL-OCS criteria in our sample resulted in excellent specificity and NPV, however, with low sensitivity and PPV, which undermines its use as a single screening tool for clinical OCD. On the other hand, it is plausible that the at-risk group for OCD by the CBCL criterion determines a subgroup with a high index of psychopathology and pattern of comorbidity that resembles the full-blow OCD, which makes us question the validity of the DSM-IV categorical model for pediatric OCD.
This study has several limitations. It is a cross-sectional study, susceptible to recall bias. Correlations of the severity of OCS with clinical and sociodemographic variables would be better examined in a longitudinal design. All diagnoses were established by proxy (mothers in 91.5% of cases). Furthermore, questionnaires were applied by a lay interviewer despite checked by senior psychiatrists.
Conclusions
A dimensional approach associates the severity of OCS with increasing psychopathology (behavioral and social problems, psychiatric comorbidity). Clinically significant OCS are a prevalent phenomenon in children (prevalence around 10%) and are associated with older age, higher frequency of behavioral problems, functional impairment, and psychiatric comorbidities. The pattern of psychiatric comorbidities found in the “OCS” group resembles that found in full-blown OCD. The cutoff point of 5 or higher in the CBCL proposed in the literature determined an at-risk for OCD group very similar phenotypically to OCD, but its use as a single screening tool may be questioned. On the other hand, our results question the validity of the use of a categorical diagnosis for pediatric OCD.
Clinical Significance
The dimensional approach of the psychopathological phenomena, as an alternative to the categorical method, is one of the targets of current nosology in psychiatry. This study provides new evidence for the existence of a positive association between OCS severity and functional impairment in youth, which supports the notion of a continuum between OCS and OCD. From a clinical perspective, these data suggest that early intervention, directed at children with subclinical symptoms detected by mean of a screening tool like the CBCL-OCD, appears relevant to prevent the development of more severe psychopathology and greater functional impairment.
Footnotes
Acknowledgments
The authors of this article would like to acknowledge the professors Giovanni Salum, Guilherme Polanczyk, Jair Mari, Luis Rohde, and Rodrigo Bressan for the work involved in carrying out this cohort.
Disclosures
Laura O. Saad and Raony C. Cesar: No disclosure; Maria C. do Rosário: Acted as a speaker for Shire and Novartis in the last 5 years; Marcelo C. Bastituzzo, Marcelo Q. Hoexter, and Gisele G. Manfro: No disclosure to report; James F. Leckman: Received support from the National Institutes of Health (salary and research funding), Tourette Association of America (formerly the Tourette Syndrome Association), Grifols (formerly Talecris), UBS Optimus Foundation, the Open Road Alliance, John Wiley & Sons (book royalties), McGraw-Hill (book royalties), and Oxford University Press (book royalties). He also serves on the scientific advisory boards of National Organization for Rare Disorders (NORD) and the Brain and Behavior Research Foundation (formerly NARSAD). Roseli G. Shavitt: Travel grant from Lundbeck to attend the 23rd Annual International OCF M; Eurípedes C. Miguel and Pedro G. Alvarenga: No disclosure to report.