
Abstract
Objective
: This study examines the effects of parental stimulant medication treatment on parent ratings of parent–child functioning. Ratings of parent–child functioning in the home setting and immediately following a laboratory-based parent–child interaction were collected.
Method
: Participants were 20 parents who along with their children (ages 5–12 years) were diagnosed with Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) attention-deficit/hyperactivity disorder (ADHD). Parents completed an open-label titration to determine their optimal dose of lisdexamfetamine (30, 50, or 70 mg/day) and then completed a month-long double-blind randomized pharmacological intervention for parental ADHD. Effects of parental stimulant medication administered for an extended duration were assessed by parent ratings of parent–child functioning in the home setting and immediately following a laboratory parent–child interaction task conducted at an academic mental health center. Data were collected from September 2010 to June 2013.
Results
: Stimulant medication versus placebo was associated with larger reductions in parental ADHD (d = 1.01–1.09), impairment (d = 0.67–0.82), and executive dysfunction (d = 0.74–0.94) in the home setting. No significant benefits of stimulant medication emerged in measures of parenting or child behavior at home. In the laboratory setting, parents treated with stimulant medication versus placebo reported fewer ADHD symptoms (d = 1.01–1.05) and their interaction was more successful (d = 0.83) and pleasant (d = 0.92). Several additional trends emerged showing beneficial effects of stimulant medication on parent–child functioning.
Conclusion
: Parents treated with stimulant medication evidenced some improvements in parent–child functioning, which support the use of pharmacological intervention to improve functioning in families with parent–child ADHD.
Clinical Trials Registration
: NCT01127607.
Introduction
A
Several recent studies providing pharmacological intervention for parents with ADHD have evidenced some benefits in parenting performance, but results have been inconsistent, perhaps due to methodological differences, including notable variability in treatment duration and assessment of treatment outcome. For example, several studies have reported few improvements in self-reported or observed parent–child behavior when stimulant medication has been administered to parents acutely (Chronis-Tuscano et al. 2010; Babinski et al. 2014). However, a number of benefits, including increased parental responsiveness and praise, emerged in an observational parent–child interaction laboratory task when stimulant medication was administered over a longer period of time (i.e., mean duration of 8 weeks; Waxmonsky et al. 2014). It remains to be seen whether benefits from stimulant medication administered over an extended duration observed in laboratory parent–child interactions are meaningful to parents and generalize to the home setting. The largest pharmacological treatment study of maternal ADHD to date failed to detect parent-reported improvement in child functioning after 12 weeks of pharmacological treatment (Jans et al. 2015), although medication effects on the parent–child relationship had not been explored.
This study examined parent and child functioning following a month-long double-blind randomized pharmacological intervention for parental ADHD. Parents completed ratings of parent–child functioning in the laboratory and home setting. It was hypothesized that parents treated with medication compared to placebo would report less impairment in their own and their child's functioning.
Methods
Procedures were approved by the Western institutional review board. Parents provided written consent, and children were assented before enrollment. Participants were parents who, along with their children (ages 5–12), were diagnosed with ADHD. Parent–child dyads were recruited from an academic mental health center and from community advertisements. Parental ADHD was diagnosed through a comprehensive assessment conducted by a clinician with an MD/PhD verifying that participants met full criteria for any Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) subtype of ADHD, including childhood onset. A score of 28 or higher on the clinician-administered ADHD Rating Scale (ADHD-RS; DuPaul et al. 1998) along with at least moderate severity (i.e., 4 or greater) on the Clinical Global Impressions Severity subscale (CGI-S; Guy 1976) and evidence of family impairment (i.e., 5+ on the family subscale of the Sheehan Disability Scale [SDS]; Sheehan et al. 1996) were required. Due to the administration of stimulant medication, current psychiatric comorbidities, assessed by the Structured Clinical Interview for DSM-IV Axis I Disorders (First et al. 1997), or medical conditions that could be worsened by stimulants (e.g., psychotropic medication use, active substance abuse, high blood pressure, pregnancy, breast feeding) were exclusionary. Parents already medicated for ADHD were required to stop treatment before enrollment.
Children were required to meet DSM-IV ADHD criteria based on parent report on the Disruptive Behavior Disorders Rating Scale (DBD-RS; Pelham et al. 1992) and the Diagnostic Interview Schedule for Children (Shaffer et al. 2000), which also assessed comorbidities beyond oppositional defiant disorder (ODD) or conduct disorder (CD). Children requiring urgent psychiatric treatment (e.g., active suicidal ideation) were ineligible. Child stimulant medication status did not impact eligibility, although parents were required to maintain the child's medication treatment throughout the study. Children treated with stimulant medication were required to be unmedicated during the parent–child task (described below) to increase the likelihood of challenging behaviors. Children treated with nonstimulant medications for ADHD were ineligible.
Procedures
Parents completed a 3-week, open-label lisdexamfetamine (LDX) trial. LDX, provided by Shire Pharmaceuticals, was started at 30 mg and could increase to 50 mg for week 2 and 70 mg for week 3. Optimal dose was defined as a physically tolerable dose that produced an ADHD-CGI of 1 or 2 (much/very much improved) plus a 30% or greater reduction of symptoms as measured by the ADHD-RS. Raters of the ADHD-RS and ADHD-CGI were not blind to medication dose during the medication optimization phase. Titration ended early if the optimal dose was achieved before week 3. More detailed information on titration is presented elsewhere (Waxmonsky et al., 2014). After dose optimization, a brief within-subjects evaluation of the observable effects of acute LDX treatment was conducted (Babinski et al. 2014; Waxmonsky et al. 2014), followed by a double-blind between-group evaluation in which parents were randomly assigned to either receive their optimally dosed LDX or a placebo. At the end of this phase (∼8 weeks later), parents completed ratings of parent–child functioning. A laboratory-based parent–child interaction task (Eyberg et al. 2010) was also completed, after which parents completed ratings of parent–child functioning during the task. Children were unmedicated during the laboratory task but could use ADHD medication on intervening days (75% of child completers regularly used medication). Five minutes of the interaction simulated a homework situation, and parents were instructed to assist their child as they saw fit. Parents and children were also given a developmentally appropriate nonacademic task consisting of 3 minutes of quiet time while the parent completed paperwork (and was instructed not to play with the child) and 5 minutes of joint play.
Thirty parent–child dyads initiated the study, with 22 completing medication titration. During titration, five parents dropped out due to side effects while two were lost to follow-up and one participant withdrew consent. A total of 20 parents completed all study procedures (10 placebo, 10 LDX, by random assignment), as two participants were lost to follow-up during the between-subjects evaluation (Waxmonsky et al. 2014). Participant characteristics are presented in Table 1. No significant demographic differences emerged between participants treated with LDX versus placebo. Participants with and without complete data did not differ by age, gender, race, marital status, income or child age, gender, race, or IQ (p > 0.25).
The sum scores are presented for the ADHD-RS and DBD-RS.
Parent-reported family functioning in the home setting
Parenting
The Alabama Parenting Questionnaire (Shelton et al. 1996) is a 42-item measure of the frequency with which parents implement the following practices: involvement, positive parenting, poor monitoring/supervision, inconsistent discipline, and corporal punishment. Items are rated from 1 (never) to 5 (always), with higher scores indicating greater use of each parenting practice. Summed subscale scores are reported. The total normed score from the Parent Stress Index (Abidin 1986) assessed parent stress related to both adult and child functioning, with higher scores indicating greater stress. The Parent Locus of Control Scale (Campis et al. 1986) was a 26-item measure of perceived parent efficacy and control over child behavior. The total score is reported herein with items rated from 1 to 5 and lower scores indicating greater control.
Adult functioning
The ADHD-RS (DuPaul et al. 1998) measured each of the DSM-IV ADHD symptoms from 0 (not present) to 3 (severe) and was completed as an interview administered by an advanced doctoral clinical psychology trainee and a board-certified child and adolescent psychiatrist. ADHD-RS sum scores were calculated, with higher scores indicating greater ADHD severity. The SDS (Sheehan et al. 1996) measured parent-reported impairment in work/school, social life, family/home responsibilities on the following scale: 0 (not at all), 1–3 (mildly), 4–6 (moderately), 7–9 (markedly), and 10 (extremely). The Brown ADD Rating Scale for Adults (BADDS; Brown 1996) assessed executive functioning impairment, with T-scores for total executive dysfunction, and subscales assessing activating to work, attention to tasks, sustained effort, affect regulation, and memory.
Child functioning
Parent report on the DBD-RS (Pelham et al. 1992) assessed child ADHD, ODD, and CD severity. The DBD-RS includes Diagnostic and Statistical Manual of Mental Disorders, 3rd edition Revised (DSM-III-R) (American Psychiatric Association 1987) and DSM-IV symptoms of ADHD, with each item scored 0 (not at all) to 3 (very much). Mean scores for each subscale are reported. The Impairment Rating Scale for Children (Fabiano et al. 2006) assessed child impairment across a range of domains, including academic and family functioning. Items are rated from 0 (no problem, does not need treatment or special services) to 6 (extreme problem, definitely needs treatment or special services).
Post-interaction ratings
Immediately following the parent–child interaction task, parents completed ratings of their own ADHD symptoms, parenting behaviors and mood, and child behavior during the interaction. Parents completed the Parent–Child Interaction Measure for ADHD, created by the study investigators to assess relevant parent behaviors during the interaction. This measure included 12 items assessing parental ADHD symptoms found to impact parental performance (Johnston et al. 2012), three items assessing parent practices impacted by parental ADHD symptoms (Johnston et al. 2012), and two items assessing perceived success in the interaction (see Table 3 and Fig. 1 for scale items). Items were rated from 0 to 6, with higher scores indicating more severe ADHD symptoms, more frequent implementation of parenting behaviors, and greater success, respectively. The Positive and Negative Affect Schedule (PANAS; Watson et al. 1988) and the IOWA Conners (Loney and Milich 1982) were also administered to assess parent mood and child behavior during the interaction, respectively. Higher scores on the PANAS indicate greater emotional intensity. The IOWA Conners yields subscores for inattentive–impulsive–overactive and oppositional–defiant child behavior, with higher scores describing more severe child behaviors.
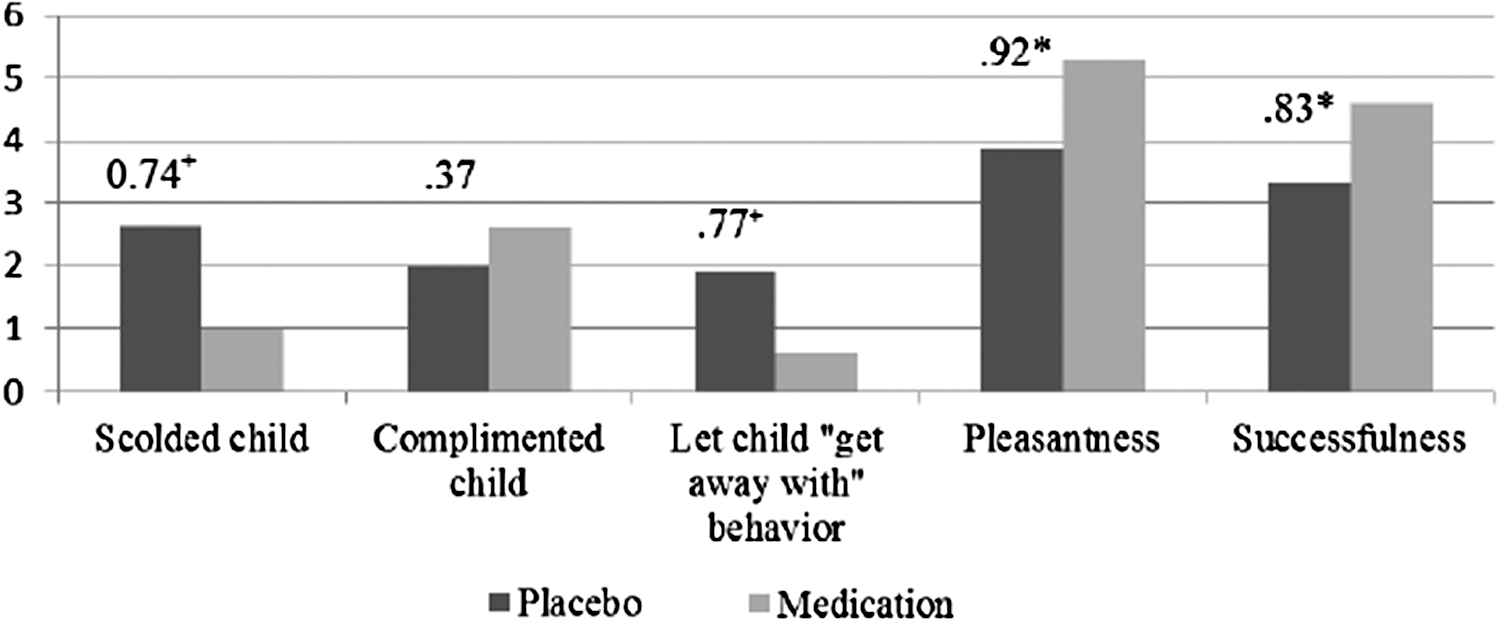
Post-interaction ratings of parent management and success. Items depicted were selected from the post-interaction rating form developed by the study investigators. Each item was rated from 0 to 6, with higher levels indicating greater use of each parenting strategy or higher intensity of pleasantness and successfulness. * = p < 0.05, + = p < 0.10.
Data analytic plan
Analysis of covariance assessed for group differences in the home setting with treatment (medication vs. placebo) as a between-subjects factor while controlling for pretreatment values for each variable. To test for differences between parents' post-interaction ratings, one-way ANOVAs were computed with treatment (medication versus placebo) as the between-subjects factor. Given the modest sample size for this exploratory study, effect sizes (Cohen's d) were also calculated and interpreted when they were 0.80 or above (Cohen 1992). Trends (i.e., p < 0.10) were also interpreted.
Results
Effects of extended medication treatment on functioning in the home setting are reported in Table 2. Medication compared to placebo was associated with significant and large reductions in parental ADHD symptoms on the ADHD-RS, and attention, affect, and overall executive functioning on the BADDS. There were also several trends with large effects on other parent-reported functional outcomes, including decreased social impairment, overall impairment, and effort and memory for parents treated with medication versus placebo. No statistically significant differences emerged regarding parenting or child functioning in the home setting.
CD, conduct disorder; ODD, oppositional defiant disorder; APQ, Alabama Parenting Questionnaire (Shelton et al. 1996); PSI, Parenting Stress Index (Abidin 1986); PLOC, Parent Locus of Control (Campis et al. 1986); ADHD-RS, ADHD Rating Scale (DuPaul et al. 1998); SDS, Sheehan Disability Scale (Sheehan et al. 1996); BADDS, Brown ADD Rating Scale for Adults (Brown 1996); DBD-RS, Disruptive Behavior Disorder Rating Scale (Pelham et al. 1992); IRS-C, Impairment Rating Scale for Children (Fabiano et al. 2006).
Stimulant medication effects on post-interaction ratings of parent management and success are presented in Figure 1, and effects on parental ADHD symptoms, mood, and child behavior are presented in Table 3. Parents treated with medication versus placebo reported more success in their interaction (i.e., pleasant interaction with child, felt interaction was successful) and lower levels on several parental ADHD-related symptoms (i.e., impulsive, not focused on interaction, did not think through consequences, and frustrated waiting for turn) with large effects. A trend also emerged showing that parents treated with medication versus placebo reported feeling less rushed and interrupting their child less frequently. While no statistically significant differences emerged regarding parenting or child behavior, a trend suggested that parents treated with medication versus placebo reported lower rates of scolding or reprimanding their child and more consistent discipline (i.e., lower scores on “let child ‘get away with’ misbehavior”). There was also a trend for parents treated with medication to report less negative affect and less defiant child behaviors, with moderate effects for both.
Parental ADHD items were rated from 0 to 6, with higher scores indicating more severe levels of each symptom. PANAS ratings range from 10 to 50 for each subscale, and higher subscale scores correspond to greater emotional intensity. Ratings on the IOWA Conners range from 0 to 15, and higher scores indicate more severe behavioral difficulty.
ADHD, attention-deficit/hyperactivity disorder; PANAS, Positive and Negative Affect Schedule.
Discussion
This study examined improvement in parent–child functioning during a pharmacological intervention for parents, who, along with their child, were diagnosed with ADHD. Stimulant medication administered over an extended duration was associated with significantly lower parental ADHD symptoms and executive functioning impairments in the home and laboratory. Medication compared to placebo was also associated with less impaired parenting, most notably in the laboratory interaction, and there were several trends supporting additional moderate to large medication effects regarding parent and child behavior. Few effects on parenting or child behavior outside of the laboratory emerged.
Parents treated with stimulant medication compared to those receiving placebo reported significantly less severe ADHD symptomology and executive dysfunction; the size of these effects was consistent with those observed in previous stimulant medication trials for adults with ADHD (Schweitzer et al. 2004; Weisler et al. 2006; Adler et al. 2008). Effect sizes on measures of impairment (i.e., SDS) were also consistent with those observed in previous medication trials (Medori et al. 2008), despite less impaired baseline scores in the current study. Of note, previous pharmacological studies of parents with ADHD have primarily linked improvements in parenting performance with reductions in parental ADHD symptoms (Chronis-Tuscano et al. 2008; Waxmonsky et al. 2014) and have not examined medication effects on executive functioning and impairments as a potential factor in improving parent–child functioning. Our findings suggest that improvements in these domains may also be important mechanisms underlying parenting improvements with stimulant medication treatment.
LDX was associated with some benefit in parenting performance in the laboratory-based parent–child interaction. Compared to parents receiving placebo, those treated with LDX reported more success during the interaction. Although not statistically significant at the p < 0.05 level, several other moderate to large benefits in parenting were evidenced, including less frequent implementation of negative parent practices (i.e., scolded or reprimanded the child) and inconsistent discipline (i.e., let child “get away with” misbehavior), during the interaction. These findings support those of several other studies that have identified these negative parenting practices among parents with ADHD and have shown them to be malleable with pharmacological treatment (Evans et al. 1994; Chronis-Tuscano et al. 2008; Waxmonsky et al. 2014). Interestingly, the effects we obtained from providing parents with stimulant medication over an extended duration appear somewhat larger than effects demonstrated from acute stimulant medication for parents (Waxmonsky et al. 2014).
While not statistically significant at the p < 0.05 level, moderate and large medication effects on oppositional child behavior and parental mood, respectively, were demonstrated in the laboratory. Although research on families of children with ADHD has demonstrated robust associations among parenting, parental mood, and oppositional child behavior (Johnston et al. 2014), studies have not specifically identified how parental ADHD is related to parental mood and child behavior. Our results suggest that medicating parents may impact children's oppositional behaviors through reduction in negative parenting practices (Chronis-Tuscano et al. 2011). In addition, reductions in parental negative mood affect dysregulation on the BADDS, and measures of ADHD suggestive of emotional impulsivity demonstrated during the interaction (e.g., impulsive, frustrated waiting for turn) point to the importance of considering improvements in emotion regulation as a potential factor mediating stimulant-related improvements in parenting performance (Mazursky-Horowitz et al. 2015).
Compared to the laboratory setting, medication effects on parenting and child behavior were generally not reported in the home setting. Of note, there were moderately lower amounts of corporal punishment reported by parents using stimulant medication continuously. The association between parental stimulant medication treatment and reductions in corporal punishment is consistent with previous work by Chronis-Tuscano et al. (2008) and is intriguing given that corporal punishment has been found to mediate the intergenerational transmission of ADHD from parent to child (Tung et al. 2014). The failure to detect more robust differences in other areas of parenting and child behavior is generally consistent with previous studies that have assessed parents' ratings in the home setting (Wietecha et al. 2012; Babinski et al. 2014). Even when parents have self-reported improvements in parenting with medication (Chronis-Tuscano et al. 2008), these improvements have not clearly been demonstrated across all domains of parenting, and numerous studies administering stimulant medication to children with ADHD have not consistently reported improvements in parent functioning and stress more generally (Chronis et al. 2003; Wietecha et al. 2012). It is likely that the long-standing impaired parent–child interactions characteristic of many families in which both a parent and child are diagnosed with ADHD are not sufficiently improved by providing pharmacological intervention for parents with ADHD for just a few weeks. Given the lack of clear improvements in parent functioning, which theoretically should precede improvement in child functioning (DeGarmo et al. 2004), the lack of improvement in child behavior in the home setting is not surprising.
There are also several other potential contributors to the more pronounced medication effects in the laboratory setting compared to the home setting. While child stimulant medication was withheld during the laboratory setting in an effort to increase the likelihood of challenging behavior, 75% of children in the study received medication at home during the course of the double-blind trial, which may have reduced variability in parent–child functioning and our ability to detect benefits of parental stimulant medication in the home setting. The relatively mild levels of parent ratings of their child's impairment and symptoms compared to other studies are consistent with this “floor” hypothesis (Chronis-Tuscano et al. 2008, 2010). In addition, difficulties in self-perception, documented among parents with ADHD (Liu et al. 2013), may also have impacted our ability to detect statistically significant differences. It may be more difficult to detect changes using a single rating over a long period of time (as was done for home ratings in the between groups trial) than having parents reflect only on brief discrete time periods (Babinski et al. 2014). Moreover, parents may more accurately report changes in their own and their child's behavior immediately following a specific interaction than on a single rating encompassing a multitude of different interactions over an extended timeframe (average of eight weeks in this study). Therefore, more immediate and repeated assessments of parent–child functioning (e.g., ecological momentary analysis) may provide more specific information regarding parent–child functioning than traditional more generalized assessments. In addition, observational and collateral reports may provide more accurate ratings of improvement for adults with ADHD.
Several additional limitations are worth noting. First, our exploratory study involved a modest sample size. This adversely impacted our ability to detect significant results, despite medium to large effects demonstrated across several domains, and precluded exploration of potential mediators and moderators of treatment outcome, including gender, child treatment status, and child comorbidities. Participating parents were relatively high functioning, evidenced by their insight that ADHD was impacting their parenting and several demographic characteristics (e.g., educational attainment, married status, impairment severity). The results of this study describe treatment-seeking parents with ADHD and may not generalize to the broader population of adults with ADHD.
Conclusions
Overall, these results echo findings from previous reports within this same sample, which have found observable improvements in parent and child functioning within the laboratory setting (Babinski et al. 2014; Waxmonsky et al. 2014), and point to pharmacological treatment of parents with ADHD as a possible pathway to improve the functioning of families with parent–child ADHD. However, effects were not reliably detected in the home setting, and benefits on child behavior were less clear. It is not clear if effects fail to translate outside the laboratory setting or if the employed methodology was too coarse to detect them. Therefore, future studies should assess for changes in home behavior over multiple time points, anchored to specific tasks (e.g., homework, bedtime).
Clinical Significance
Results reinforce that pharmacological intervention for parents alone is insufficient to ameliorate impaired parent–child interactions among parent–child ADHD dyads. Multimodal treatment, targeting both parent and child ADHD symptoms and impairments, may be necessary to evoke meaningful and robust changes in parenting behavior for adults with ADHD that persist outside of the laboratory. Future research should aim to identify optimal intervention procedures to benefit families in which both a parent and child have ADHD.
Footnotes
Acknowledgments
This study was fully funded by an investigator-initiated grant from Shire Pharmaceuticals (NCT01127607). Drs. Waxmonsky and Waschbusch were the principal investigators.
Disclosures
This study was fully funded by an investigator-initiated grant from Shire Pharmaceuticals. Drs. Waxmonsky and Waschbusch were the principal investigators. All authors contributed to the discussion and interpretation of results. In the past three years, Dr. Waxmonsky has received research funding from Shire (this study), Noven Pharmaceuticals, and Janssen (drug donation), as well as NIMH, and served on the advisory board for Noven and as a speaker for CME talks by Quintiles. Dr. Waschbusch has received research support from Shire, Inc. (this study) while Dr. Pelham has served on the advisory board for Noven Pharmaceuticals. Both have also received funding from NIMH. Dr. Pelham has also received funding from NIAAA and the IES. All other authors have no disclosures to report.