
Abstract
Objective:
This is a feasibility study evaluating the safety, tolerability, and potential anxiolytic efficacy of the α2 agonist guanfacine extended-release (GXR) in children and adolescents with generalized anxiety disorder (GAD), separation anxiety disorder (SAD), or social phobia/social anxiety disorder.
Methods:
Youth aged 6–17 years with a primary diagnosis of GAD, SAD, and/or social anxiety disorder were treated with flexibly dosed GXR (1–6 mg daily, n = 62) or placebo (n = 21) for 12 weeks. The primary aim of this study was to determine the safety and tolerability of GXR in youth with anxiety disorders, which involved the analysis of treatment-emergent adverse events (TEAEs), the emergence of suicidal ideation and behaviors, vital signs, and electrocardiographic/laboratory parameters. Exploratory efficacy measures included dimensional anxiety scales (Pediatric Anxiety Rating Scale [PARS] and Screen for Child Anxiety Related Emotional Disorders [SCARED]), as well as the Clinical Global Impression–Improvement (CGI-I) scale. As this was an exploratory study, no inferential statistical analyses were performed.
Results:
GXR was safe and well tolerated. Treatment-related mean ± standard deviation changes in heart rate (GXR: 1.8 ± 12 beats per minute [bpm] decrease; placebo: 0.5 ± 11 bpm decrease), systolic blood pressure (GXR: 2.3 ± 11 mm Hg decrease; placebo: 1.7 ± 11 mm Hg decrease), or diastolic blood pressure (GXR: 1.3 ± 9 mm Hg decrease; placebo: 0.9 ± 7 mm Hg increase) were similar between treatment groups. TEAEs, including headache, somnolence/fatigue, abdominal pain, and dizziness, were consistent with the known safety profile of GXR. No differences were observed between treatment groups for PARS and SCARED scores, although at endpoint, a higher proportion of subjects receiving GXR versus placebo demonstrated CGI-I scores ≤2 (54.2% vs. 31.6%), as rated by the clinician investigator.
Conclusions:
GXR was well tolerated in pediatric subjects with GAD, SAD, and/or social anxiety disorder.
ClinicalTrials.gov
Identifier:
NCT01470469.
Introduction
A
Generalized anxiety disorder (GAD), separation anxiety disorder (SAD), and social phobia/social anxiety disorder are the most frequently occurring childhood anxiety disorders (Wehry et al. 2015) and frequently cooccur. As such, these three childhood anxiety disorders are often referred to as the “pediatric anxiety triad” (Walkup et al. 2008). Importantly, many (Walkup et al. 2001, 2008), but not all (Rynn et al. 2001, 2007; Strawn et al. 2015a), psychopharmacologic studies in children and adolescents have treated the pediatric anxiety triad as a monolith, rather than focusing on individual diagnoses. The reasons for this approach are multifactorial (e.g., including phenomenologic, clinical, theoretical, and epidemiologic data) and are the result of high rates of comorbidity among the triad disorders (Walkup et al. 2008), comparable onset patterns (Beesdo et al. 2010), common neurocircuitry (Blackford and Pine 2012; Strawn et al. 2012b), and similar responses to pharmacotherapy and psychotherapy, especially cognitive behavioral therapy (CBT) (Compton et al. 2010; Kendall et al. 2010; Strawn et al. 2012a).
Current evidence-based treatment options for these anxiety disorders include psychotherapy (i.e., CBT) and pharmacologic treatment, as well as combination treatment (i.e., pharmacotherapy + psychotherapy) (Keeton et al. 2009; Wehry et al. 2015). In fact, the extant evidence base (Strawn et al. 2012a) and practice guidelines (Connolly and Bernstein 2007) regarding these “triad disorders” suggest that selective serotonin reuptake inhibitors (SSRIs) represent first-line psychopharmacologic treatments for these conditions, with preliminary clinical data also supporting use of serotonin-norepinephrine reuptake inhibitors (SNRIs) (Keeton et al. 2009; Rynn et al. 2011; Strawn et al. 2015a). In a recent meta-analysis of the efficacy of SSRIs and SNRIs in pediatric anxiety disorders (i.e., GAD, SAD, and social anxiety disorder), all evaluated medications (duloxetine, fluoxetine, fluvoxamine, paroxetine, sertraline, and venlafaxine) demonstrated efficacy compared with placebo, with an effect size estimate of 0.62 (95% confidence interval: 0.34–0.89; p = 0.009) (Strawn et al. 2015b). However, it is estimated that ∼2 in 5 patients do not respond to SSRIs (Walkup et al. 2008), and antidepressant medications may be associated with class-specific tolerability concerns (e.g., activation) (Strawn et al. 2015b), highlighting the need for alternative treatments (Seidel and Walkup 2006; Rynn et al. 2011).
Guanfacine extended-release (GXR), an α2A-adrenergic receptor agonist, is approved for the treatment of attention-deficit/hyperactivity disorder (ADHD) in pediatric patients (INTUNIV 2011). Importantly, activation of the α2A receptor modulates catecholamine neurotransmission and may decrease synaptic release of norepinephrine (Bucheler et al. 2002) and, based on studies in lower animals, may enhance prefrontal cognitive functions by stimulating postsynaptic α2A receptors on pyramidal cells in the prefrontal cortex, thereby enhancing prefrontal connectivity (Arnsten et al. 2007; Arnsten and Jin 2012). With regard to its effects on anxiety, administration of guanfacine to rodents blocks working memory impairments induced by anxiogenic agents (Birnbaum et al. 2000) and may protect cognitive performance during stress via second messenger systems (e.g., protein kinase A). Furthermore, agents that decrease norepinephrine release or dampen its postsynaptic effects appear to attenuate fear responses (Soeter and Kindt 2015) and produce anxiolytic effects (Tanaka et al. 2000). In this regard, norepinephrine is intimately involved in fear processing (e.g., sensitization and fear conditioning) and has been implicated in pediatric anxiety disorders (Bremner et al. 1996). Thus, it is not surprising that previous studies support the role for adrenergic agonists, particularly α2A agonists, in the treatment of anxiety disorders (Newcorn et al. 1998).
Given the limitations of antidepressants in the treatment of pediatric anxiety disorders [e.g., class-specific side effects (Strawn et al. 2015b), heterogeneity in response (Compton et al. 2014), and rates of nonresponse (Wehry and Strawn 2014)], the goal of this study was to increase the psychopharmacologic armamentarium for these chronic and often relapsing disorders (Ginsburg et al. 2014) that are associated with significant morbidity and mortality. Specifically, the primary objective of the current feasibility study was to evaluate the safety and tolerability of GXR in children and adolescents aged 6–17 years with a primary diagnosis of GAD, SAD, or social anxiety disorder. Exploratory objectives included various assessments of efficacy for GXR in children and adolescents with one of the pediatric anxiety triad disorders (GAD, SAD, or social phobia/social anxiety disorder).
Methods
Study design
In this double-blind, placebo-controlled, phase 2 study, children and adolescents with GAD, SAD, or social anxiety disorder were randomly assigned to either GXR or placebo (3:1 ratio) via an interactive response technology system. Subjects were screened at 32 sites in the United States, and eligible individuals were enrolled into a 6-week dose-optimization period, followed by a 6-week maintenance period, a 2-week taper period, and a 7- to 9-day follow-up period off treatment. Study doses of GXR ranged from 1–6 mg per day. At baseline, GXR was initiated at a dose of 1 mg in all subjects who were not randomly assigned to placebo. During dose optimization, GXR was titrated weekly, to a maximum of 0.12 mg/(kg·d) (not exceeding 6 mg per day), based on investigator-assessed clinical response, tolerability, and the clinician-investigator's judgment. In subjects weighing <50 kg at baseline, GXR dose was titrated to achieve a daily dose of 0.06–0.12 mg/kg (INTUNIV 2011), whereas in subjects weighing ≥50 kg, GXR dose was titrated to a daily dose of 3–6 mg.
Subjects
Subjects aged 6–17 years who met the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition, Text Revision; DSM-IV-TR) (American Psychiatric Association 2000) criteria for a primary diagnosis of one or any combination of the following disorders: GAD, SAD, or social anxiety disorder, were eligible for participation, and these diagnoses were based on a detailed psychiatric evaluation at screening, which included completion of the Anxiety Disorder Interview Schedule for DSM-IV Child and Parent Version (ADIS-C/P). Other inclusion criteria included having a score ≥4 on the ADIS-C/P Clinical Severity Rating (CSR) scale for the principal diagnosis at both the screening and baseline visits. Subjects were excluded if they had a current comorbid diagnosis of a major depressive disorder, bipolar disorder, psychosis, ADHD, eating disorder, substance use disorder, or pervasive developmental disorder other than Asperger syndrome. Study participants could not have an ADIS-C/P CSR score for any Axis I disorder greater than their ADIS-C/P CSR score for the principal diagnosis of GAD, SAD, or social anxiety disorder. Other exclusion criteria included: (1) involvement in any evidence-based psychosocial intervention intended to reduce anxiety symptoms within 14 days of baseline; (2) being considered at risk for suicide by the investigator, having previously attempted suicide, or currently demonstrating active suicidal ideation; (3) history or presence of structural cardiac or serious heart rhythm abnormalities; and (4) failure to respond to two trials of an SSRI/SNRI or one trial of CBT for the treatment of GAD, SAD, or social anxiety disorder.
All subjects' parents or legally authorized guardians provided written informed consent, and subjects provided written assent. These documents were approved by an independent ethics committee and regulatory agencies (as appropriate) before study initiation. The study was conducted in accordance with the International Conference on Harmonisation of Good Clinical Practice and the principles of the Declaration of Helsinki.
Safety assessments
Safety and tolerability assessments included incidence of treatment-emergent adverse events (TEAEs), vital signs (including weight), and electrocardiogram (ECG) parameters. Study visits occurred weekly during dose optimization, biweekly during maintenance, and weekly during dose taper. ECGs were obtained at screening, baseline, and once each during dose optimization and maintenance. Additional safety assessments included the Columbia–Suicide Severity Rating Scale (C-SSRS) (Posner 2011) and Pediatric Daytime Sleepiness Scale (PDSS) (Drake et al. 2003). The C-SSRS, a semi-structured, clinician-administered instrument, captured the occurrence, severity, and frequency of suicide-related thoughts and behaviors and was administered at screening and at all subsequent study visits. The PDSS, a self-report scale for assessing daytime sleepiness, was collected at baseline (Visit 2) and Visits 3–11 (weeks 1–12 of treatment), and questions were scored from 0–4 (never = 0; seldom = 1; sometimes = 2; frequently = 3; always = 4), with higher scores denoting increased sleepiness.
Exploratory efficacy assessments
Efficacy was explored by using the following measures: the Pediatric Anxiety Rating Scale (PARS) (2002), the Clinical Global Impressions (CGI) scale (1976), the Screen for Child Anxiety Related Disorders (SCARED) (Birmaher et al. 1997), and the Childhood Sleep Habits Questionnaire (CSHQ) (Owens et al. 2000). The PARS, a clinician-rated instrument for assessing the severity of anxiety symptoms associated with common DSM-IV anxiety disorders over time in children and adolescents aged 6–17 years, includes a 50-item symptom checklist, as well as a second section consisting of specific severity/impairment items that are rated on a 6-point Likert scale. The PARS was administered by an independent evaluator at baseline through Visit 11. The CGI–Improvement (CGI-I) scale, a global evaluation of improvement in a subject's condition over time, rated on a scale from 1 (very much improved) to 7 (very much worse), was administered at Visits 3–11. The CGI-I was completed by the principal investigator or a delegated study sub-investigator who was a licensed clinician. The final two efficacy assessments were completed by parents and study subjects. The SCARED, a tool measuring multiple anxiety symptoms, including panic symptoms, agoraphobia, and school avoidance, was completed at baseline through Visit 11. The CSHQ, which screens for common sleep problems in children (higher scores indicative of more sleep problems), was administered at baseline, Visit 8, and Visit 11.
Statistical analyses
Given the exploratory nature of this study, there was no formal sample size calculation, as the study was not powered for any statistical comparisons. Safety analyses and exploratory efficacy analyses were conducted on all subjects who had taken at least one dose of study drug and had at least one postbaseline assessment. As all efficacy analyses were exploratory and not specified a priori, no inferential statistical analyses were performed on these data.
Results
Subjects
As shown in Figure 1, 134 subjects were screened at 32 U.S. sites, and 83 subjects were enrolled (nGXR = 62; nplacebo = 21). The mean ± standard deviation (SD) number of patients randomized per site was 3.5 ± 1.7 (range: 1–8 patients per site). Demographically, the treatment groups were generally well balanced and baseline characteristics between GXR-treated subjects and those receiving placebo with regard to age, sex, race, ethnicity, anxiety disorder diagnoses, or principle diagnoses were similar (Table 1). With regard to the distribution of body mass index categories, a larger proportion of subjects classified as “overweight” or “obese” were assigned to placebo compared with GXR (38% vs. 27%; Table 1). Most study subjects had a diagnosis of GAD (42.2%), although comorbidity among the triad anxiety disorders was common. The majority of subjects completed the optimization and maintenance periods with similar completion percentages across treatment groups (Fig. 1), and the most frequently reported reasons for early study termination across treatment groups are summarized in Figure 1.
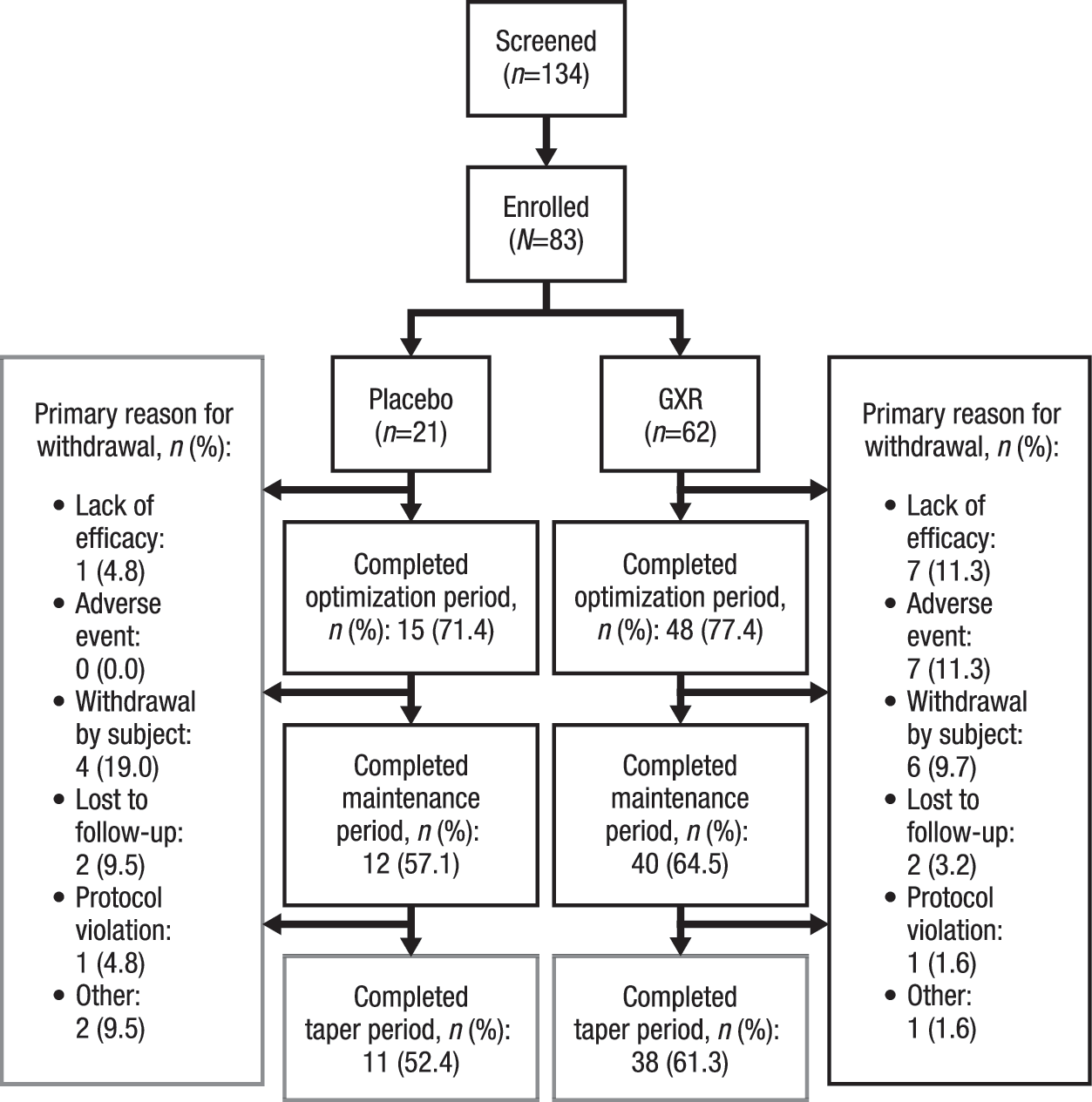
Subject flow diagram. GXR, guanfacine extended-release.
Age was calculated as the difference between the date of birth and the date of informed consent, truncated to years.
BMI was calculated as [weight(kg)/height(m)2].
The BMI categories were derived by using the Centers for Disease Control BMI percentiles for children and adolescents; underweight = BMI <5th percentile; normal = 5th percentile up to <85th percentile; overweight = BMI 85th to <95th percentile; obese = BMI ≥95th percentile. For determining BMI categorization, age in months was calculated as the difference between the date of birth and the date of informed consent.
The principal diagnosis was defined as the diagnosis with the highest clinical severity rating scale on the composite summary sheet. If ≥2 diagnoses had equal clinical severity ratings, the diagnosis that emerged first was named the principal diagnosis (i.e., generalized anxiety disorder, separation anxiety disorder, social anxiety disorder, or other).
BMI, body mass index; GXR, guanfacine extended-release; SD, standard deviation.
Dosing
The mean ± SD length of exposure to treatment was similar between subjects receiving placebo (72.3 ± 34.2 days) and those treated with GXR (79.8 ± 31.5 days); the mean ± SD optimal dose received was 2.7 ± 1.25 mg, with nearly half the GXR-treated subjects (46.8%) receiving doses of either 2 or 3 mg. The remaining subjects received 1 mg (9.7%), 4 mg (9.7%), 5 mg (6.5%), or 6 mg (1.6%).
Vital signs, weight, ECG, and laboratory results
At week 12 (Visit 11/early termination [V11/ET]), observed differences between the treatment groups in mean height or weight changes from baseline were unremarkable. At week 12 (V11/ET), subjects receiving GXR and placebo exhibited similar mean ± SD treatment-related decreases from baseline in heart rate (GXR: −1.8 ± 11.5 beats per minute [bpm]; placebo: −0.5 ± 11.1 bpm), supine systolic blood pressure (GXR: −2.3 ± 11.4 mm Hg; placebo: −1.7 ± 11.2 mm Hg), and supine diastolic blood pressure (GXR: −1.3 ± 9.1 mm Hg; placebo: 0.9 ± 7.4 mm Hg).
Electrocardiographically, similar magnitude changes from baseline were observed between groups in PR and QRS intervals at week 12 (V11/ET). Mean ± SD changes from baseline in QTc interval corrected by Bazett's formula (QTcB) at week 12 (V11/ET) were also similar between treatments (GXR: −1.3 ± 19.2 milliseconds; placebo: −1.7 ± 11.4 milliseconds), although a nonclinically significant increase in QTc interval corrected by Fridericia's formula (QTcF) was observed in GXR-treated subjects compared with placebo-treated subjects (GXR: 4.1 ± 14 milliseconds; placebo: 0.3 ± 9.4 milliseconds); no subject demonstrated an increase in QTcF above 50 milliseconds in either treatment group.
Suicidal ideation and behavior (C-SSRS)
Regarding lifetime suicidality, 4 (6.5%) subjects randomly assigned to GXR reported a history of nonspecific active suicidal thoughts (C-SSRS score of 2) compared with 3 (14.3%) subjects who were randomly assigned to placebo. In addition, 1 (4.8%) subject randomly assigned to placebo had a history of an actual suicide attempt and 1 (1.6%) subject randomly assigned to GXR had a lifetime history of an aborted suicide attempt. One GXR-treated subject reported suicidal ideation (C-SSRS severity of 1 [“wish to be dead”]) during the course of treatment (week 1) but denied “nonspecific active suicidal thoughts.” No suicidal behaviors were reported during acute treatment, and there were no suicide attempts during the course of the study.
Adverse events
A total of 334 TEAEs were reported by 64 subjects during the study (placebo: 13 [61.9%] subjects; GXR: 51 [82.3%] subjects), and the majority of these TEAEs were rated as mild or moderate in severity. In GXR-treated subjects, 8 individuals discontinued from the study due to 11 TEAEs, including tachycardia, blurred vision, fatigue (2 events), dizziness (2 events), postural dizziness, anxiety, emotional disorder, mood-related changes, and panic attack. However, as per the subject flow diagram (Fig. 1), TEAEs were reported as the primary reason for withdrawal in only 7 out of 8 subjects. The most frequent TEAEs for those receiving GXR included headache (35.5%), somnolence (27.4%), and fatigue (21.0%; Table 2). Regarding sedation, as measured by week 12 (V11/ET), mean ± SD change in PDSS total score among subjects receiving GXR did not demonstrate a clinically meaningful difference compared with PDSS scores of those receiving placebo (GXR: −1.2 ± 4.6; placebo: −0.1 ± 4.7). Overall, TEAEs among GXR-treated youth were consistent with the known safety profile of this medication (Biederman et al. 2008; Sallee et al. 2009; Connor et al. 2010; Wilens et al. 2012; Newcorn et al. 2013).
AEs, adverse events; GXR, guanfacine extended-release.
Exploratory efficacy analyses
At week 12 (V11/ET), change from baseline in PARS scores, as rated by an independent evaluator, revealed decreases in both treatment groups over time (GXR: −6.9 ± 6.6; placebo: −5.6 ± 6.3; Fig. 2A). Similarly, week 12 (V11/ET) SCARED scores decreased from baseline in both treatment groups, as rated by children (GXR: −12.6 ± 13.8; placebo: −10.6 ± 12.5; Fig. 2B) and parents (GXR: −15.2 ± 14.6; placebo: −10.1 ± 10.1; Fig. 2C). A summary of the CGI-I scores by visit and treatment group is shown in Figure 2D. At week 12 (V11/ET), 32 GXR-treated subjects had a CGI-I score ≤2 (54.2%) compared with only 6 placebo-treated subjects (31.6%), as rated by the clinical investigator. Finally, on the CSHQ, no numerical differences were detected in total mean ± SD scores between GXR- and placebo-treated subjects at week 12 (V11/ET; GXR: 48.5 ± 8.4; placebo: 50.4 ± 10.5).
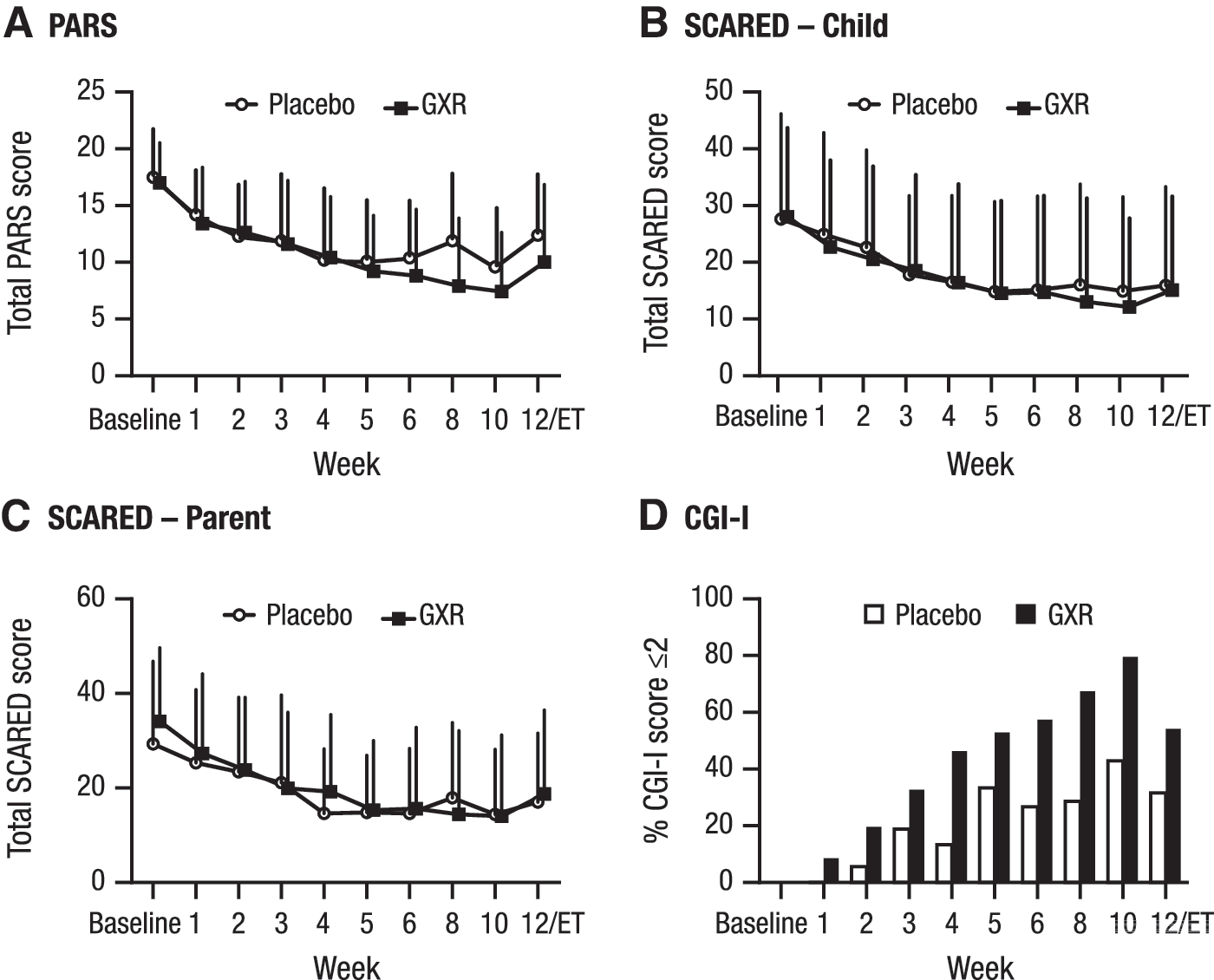
Anxiety symptoms and improvement during double-blind treatment with GXR. PARS
Discussion
This is one of the first studies to evaluate a non-antidepressant or non-benzodiazepine intervention in anxious youth and is specifically the first study to assess the safety and tolerability of GXR and to explore its potential efficacy in pediatric patients with anxiety disorders, including GAD, SAD, and social anxiety disorder. From a safety standpoint, the results reported here are consistent with the known safety profile of GXR in patients with ADHD (Biederman et al. 2008; Sallee et al. 2009; Connor et al. 2010; Wilens et al. 2012; Newcorn et al. 2013) and with the tolerability profile of guanfacine in youth with tic disorders (many of whom have cooccurring anxiety disorders) (Coffey et al. 2000); no new safety signals were identified. In addition, clinical laboratory results, vital signs, and ECG results were consistent with findings made from previous studies of GXR. Given that blood pressure and heart rate are tightly regulated by central noradrenergic tone (Guyenet 2006), a failure to detect changes in blood pressure and heart rate—which has been observed in prior randomized controlled trials of GXR in youth—may relate to the more conservative dosing in this study, as previously discussed. Taken together, the extant data regarding hemodynamic effects of GXR in youth suggest that clinicians should monitor blood pressure and pulse before initiating treatment and periodically throughout treatment with GXR, including in youth who may be treated with concomitant medications that are known to have adverse hemodynamic effects (e.g., medications with α1 antagonism).
Although this inaugural study of GXR in pediatric patients with anxiety disorders suggests that GXR is well tolerated, there are a number of important limitations. First, because of the small sample size, this study is underpowered to detect differences in efficacy between groups. Second, the unbalanced randomization may have further attenuated the ability to detect differences between treatment groups and may have inflated the placebo response rate (e.g., due to increased subject or physician expectation of randomization to active drug/treatment efficacy) (Dobson and Strawn 2016). In this regard, recent studies have shown that treatment expectation at baseline predicts placebo response in clinical trials involving antidepressants in adults (Rutherford et al. 2016) and youth (Strawn et al. 2016). Third, some of the dimensional exploratory efficacy measures (e.g., PARS) were assessed by independent evaluators, whereas the CGI-I scores were determined by the clinical investigators. As such, although the investigators who assessed global improvement may have been aware of more of the global functioning of the patients and functional impairment compared with the “independent evaluators,” they may have been more aware of the side effects associated with GXR treatment; this may have introduced possible bias.
Although this study only examined efficacy on an exploratory basis, some results warrant additional discussion. First, the dosing in this study is of particular interest, particularly with regard to guanfacine. During the 12-week acute treatment phase of this study, nearly 50% of subjects had doses of 2 to 3 mg, with a mean ± SD dose of 2.7 ± 1.25 mg. Fixed-dose studies of GXR have suggested that greater weight-based doses may be associated with increased symptomatic improvement in pediatric patients with ADHD (Sallee et al. 2009). Thus, to the extent that some anxiety symptoms may be adrenergically mediated, greater reductions in central noradrenergic tone could potentially yield greater improvement in anxiety symptoms. Second, it is possible that anxiety-related somatic symptoms may confound assessment of tolerability and adverse events, and study clinicians may have titrated GXR more slowly and more conservatively compared with youth with ADHD.
Throughout the dose-optimization and maintenance periods, numerically higher CGI-I values—as assessed by study clinicians—were demonstrated for subjects treated with GXR relative to placebo, suggesting that GXR administered to youth with anxiety disorders may lead to global improvements. However, the PARS and SCARED were conducted by the independent evaluators, whereas the CGI-I was rated by the clinical investigators, which may have contributed to this result. Although the change scores on the PARS and SCARED measures were numerically larger for the GXR groups, the differences observed were not considered to be of clinical significance. A larger, adequately powered study would provide more definitive conclusions. To have 80% power to detect an effect size of 0.4 for the PARS (Cohen's d), such a study would require ∼100 patients (randomized 1:1 to medication or placebo) or ∼264 patients (randomized 3:1, nGXR = 198, nplacebo = 66). If, however, the true effect size for GXR were putatively similar to an SSRI/SNRI for the continuous measure of anxiety (0.62) (Strawn et al. 2015b), then, ostensibly, a smaller sample would be required. Importantly, it remains unknown whether similar types of patients respond to SSRI/SNRIs versus medications with alternate mechanisms of action (e.g., anti-adrenergics), and this might also represent a limitation of using a power analysis based on SSRI response to inform the design of studies with alternative mechanisms of action. Nonetheless, it is of interest that similar percentages of patients “responded” to SSRI treatment in the Child/Adolescent Anxiety Multimodal Study (CAMS) (Walkup et al. 2008) compared with the “response rate” in this study and that both studies had a similar design (i.e., unbalanced randomization, pediatric anxiety triad diagnoses, and inclusion criteria). Finally, although there is no indication from this small study that GXR may be a successful treatment for anxiety, there is also no evidence to suggest that GXR increases symptoms of anxiety.
Conclusions
The results from this pilot study suggest that GXR is well tolerated in pediatric subjects with anxiety disorders, and they provide preliminary support to consider pursuing an adequately powered future efficacy study of guanfacine and potentially other antiadrenergics in youth with anxiety disorders. In addition, these data raise the possibility that GXR might be evaluated more thoroughly in patients with ADHD and cooccurring tic disorders, particularly given that α2 agonists (1) are frequently prescribed (Fiks et al. 2015); (2) reduce ADHD and tic symptoms in this population (Bloch et al. 2009) and (3) that patients with tic disorders commonly present with anxiety symptoms (Coffey et al. 2000). Broadly, these results suggest that the evaluation of anti-adrenergics will be of particular importance given that many youth do not respond adequately to first-line psychopharmacologic (e.g., SSRIs and SNRIs) or psychotherapeutic (e.g., CBT) interventions.
Clinical Significance
The favorable tolerability profile of GXR observed in this study suggests that clinicians may use GXR—as clinically appropriate—without fear of worsening anxiety symptoms. In this regard, extrapolation of this study data to youth with ADHD and cooccurring anxiety disorders could suggest that GXR might provide a benefit for the treatment of comorbid anxiety, while not being associated with a risk for worsening anxiety, as may be a concern with stimulant medications. However, it is important to note that not all studies suggest a link between worsening anxiety and psychostimulant treatment (Coughlin et al. 2015). Finally, if supported by adequately powered clinical trials, anti-adrenergics medications may represent important adjunctive agents for anxious youth with partial responses to traditional first-line pharmacotherapies who have experienced intolerable side effects with traditional first-line interventions.
Footnotes
Acknowledgments
The authors thank Alison McMorn for her contributions to the study. Under the authors' direction, Wilson Joe, PhD, of MedErgy, provided editorial assistance for this publication. Shailesh Desai, PhD, of Shire, also reviewed and edited the article for scientific accuracy. Shire provided funding to MedErgy for editing support. Although the sponsor was involved in the design, collection, analysis, interpretation, and fact checking of information, the content of this article, the ultimate interpretation, drafting/reviewing/editing of the article, and the decision to submit it for publication in the Journal of Child and Adolescent Psychopharmacology were made by the authors independently. Study statistician: M.H.
Disclosures
Dr. Strawn has received research support from Eli Lilly, Edgemont, Shire, Forest Research Laboratories, Lundbeck, the National Institute of Mental Health (NIMH), and Neuronetics. He has received royalties from Springer for the publication of two texts and has received material support from Assurex Health. Dr. Compton has received research support from the NIMH and Shire, and currently serves on the editorial board of the Journal of Consulting and Clinical Psychology, Journal of Child and Adolescent Psychopharmacology, and BMC Psychiatry. Dr. Albano has received research support from the NIMH and currently receives honorarium from the American Psychological Association and royalties from Oxford University Press for editorial positions. Dr. Robertson and Mr. Hamdani are employees of Shire and hold stock and/or stock options at Shire. Dr. Rynn has received research support from Eli Lilly and Shire, as well as from the NIMH and the National Institute of Child Health and Human Development.