
Abstract
Objective:
To assess the long-term effect of all treatment options for pediatric bipolar disorders on body mass index (BMI) and to explore individual characteristics associated with less BMI increase during psychotropic medication exposures.
Methods:
A retrospective cohort study was conducted by using the 1995 to 2010 General Electric Electronic Medical Record database. Individuals aged 18 years or younger who had a new bipolar disorder episode were identified. Treatment exposure was defined based on the medication regimens patients received, which include atypical antipsychotic (AT) monotherapy, mood stabilizer (MS) monotherapy, antidepressant (AD) monotherapy, AT+MS polytherapy, AT+AD polytherapy, MS+AD polytherapy, and no treatment. Both treatment exposure and BMI were coded as time varying, which could change from month to month. According to the duration of treatment and the availability of BMI measures, individuals were followed for up to 3, 6, 9, and 12 months since the treatment initiation. Repeated-measures mixed models were applied to compare the impact of different medication regimens and the length of drug exposure on BMI after adjusting for the baseline BMI, sociodemographic factors, comorbidities, and psychotherapy.
Results:
A total of 2299 treated and 4544 untreated children and adolescents who met the inclusion criteria were identified. Analysis using repeated-measures mixed models showed that those on AT monotherapy (the reference group) had a gradually diminished, but statistically significant, monthly increase in BMI during all durations of drug exposure (3 months: 0.36 kg/m2, 6 months: 0.20 kg/m2, 9 months: 0.17 kg/m2, and 12 months: 0.16 kg/m2). As compared with AT monotherapy, the magnitude of increase in BMI associated with MS, AD monotherapy, and no treatment was significantly less at all time points, indicating less steep slopes of BMI change over time compared with AT monotherapy, especially during the short-term exposure. The combinations of AT with other psychotropic medications (ATMS, ATAD) were associated with a similar BMI increase as AT monotherapy. Individual characteristics found to be associated with a less increase in BMI during psychotropic medication exposure were being younger and having a higher baseline BMI.
Conclusion:
The long-term use of atypical antipsychotics, both as monotherapy or in combination with other psychotropic medications in children and adolescents with bipolar disorder, was associated with a steady and cumulative increase in BMI.
Introduction
A
AT and mood stabilizers (MS) have been associated with weight gain in children and adolescents (Fedorowicz and Fombonne 2005; Corell and Carlson 2006). Previous studies report that 40.8% of children and adolescents with bipolar disorder are “at-risk for overweight” and 22.1% are “overweight” (Goldstein et al. 2008) compared with about 35.5% and 18% among all youth in the United States (Ogden et al. 2006). In 2013 alone, 42 million children less than the age of 5 were overweight or obese (World Health Organization 2014). Childhood obesity has both immediate and long-term health effects (CDC, Accessed 2015). Obese children and adolescents are at a greater risk of having prediabetes (Li et al. 2009; CDC 2011), bone and joint problems, sleep apnea, and social and psychological problems, including low self-esteem and stigmatization (Dietz 2004; Daniels et al. 2005; DHHS 2010). Long-term effects include likelihood of adult obesity (Guo and Chumlea 1999; Freedman et al. 2001, 2005, 2009), increasing the risk of heart disease, diabetes, stroke, several types of cancer, and osteoarthritis (DHHS 2010).
A systematic review of nineteen studies involving data collected from 24 individual medication trials (open label or randomized controlled trials) by Correll et al. on 684 children and adolescents (mean age: 12.3 years) with bipolar disorder showed a significant increase in weight associated with the use of MS and AT. Polytherapy with MS plus AT caused more weight gain than MS monotherapy but not different than atypical antipsychotic monotherapy (Correll 2007). There are also limited observational studies comparing the risk of weight gain associated with AT and MS in the adolescent population (Chengappa et al. 2002; Patel et al. 2007; Castro-Fornieles et al. 2008; Macmillan et al. 2008; Kompoliti et al. 2010; Ghate et al. 2012). The findings are generally consistent with the conclusion of the systematic review, although most of these studies are not limited to children and adolescents with bipolar disorder.
Despite the evidence, there are still unanswered questions regarding the risk of weight gain associated with psychotropic medication use in children. Bipolar disorder is a chronic disorder that often requires long-term treatment. The existing studies all have short durations of follow-up [mean of 15.4 ± 12.7 weeks for clinical trials (Correll 2007) and 4 to 12 weeks for observational studies], which is not enough to inform the long-term impact of the psychotropic medications, especially psychotropic polytherapy. Also, medication utilization and management for bipolar disorder is complex in real-world practice. Many patients go through a process in which drugs are titrated, augmented, or switched. These patients are often censored in clinical trials and excluded in most observational studies. The findings of these studies may not fully reflect the risk faced by patients who are undergoing treatment for bipolar disorder. Moreover, medications used in the treatment of bipolar disorder include not only AT and MS but also antidepressants (AD) (American Psychiatric 2002; Ng et al. 2009). Some AD have been associated with weight gain in adults; the existing literature that examined medications associated with weight change in pediatric bipolar disorder, however, has focused solely on AT and MS. The comparison of the effect of all available treatment regimens on weight in children and adolescents with bipolar disorder has not yet been conducted in a real-world setting. Lastly, despite weight gain as a common side effect among treated bipolar cases, it is known that at least some patients are not affected (Torrent et al. 2008). It remains unexplored whether patients with certain characteristics could prevent or attenuate this adverse effect of psychotropic medications.
Therefore, the objectives of our study were to assess the long-term effect of all treatment options for pediatric bipolar disorders on body mass index (BMI) and to explore factors protecting children and adolescents from a BMI increase associated with psychotropic medication exposure.
Methods
Data source
This study was conducted by using the General Electric (GE) Centricity electronic medical record (EMR) research database. The data include longitudinal ambulatory health records from 1995 through 2010 for around 10 million patients, and they represent more than 70 consortium member institutions across 40 states. The database records patient information such as detailed demographics, payment types, patient diagnosis and procedural information, vital signs, and laboratory test results. Medication list entries (both prescription and over-the-counter drug use) include the start and stop dates along with the reason for stopping the medication. For each patient visit, the specialty of physician who attended to the patient and the practice type are also documented. The database is de-identified in accordance with the Health Insurance Portability and Accountability Act and has been used widely in published literature (LaFleur et al. 2011; McAdam-Marx et al. 2011; Ghate et al. 2013).
Sample population
The individuals eligible for inclusion were: (1) less than 18 years of age; (2) had a diagnosis of bipolar disorder (ICD-9-CM code: 296.0, 296.1, 296.4, 296.5, 296.6, 296.7, 296.8) after a minimum of 180 days (also known as the baseline/washout period) free of both bipolar diagnosis and prescription (defined as index bipolar diagnosis); according to the receipt of psychopharmacotherapy after the index diagnosis, individuals identified were further categorized as (1) untreated defined as never receiving any psychotropic medications, and (2) treated defined as receiving at least 3 months of prescription medication for bipolar disorder; individuals who received less than 3 months of psychotropic prescriptions or those who did not have BMI measures taken at baseline and during follow-up were excluded. The index prescription date was defined as the date on which the patient received the first bipolar-related medication, namely AT (AT), MS, or AD after the index bipolar diagnosis. The baseline BMI was defined as a BMI measure taken on or within 30 days before the index diagnosis (for the untreated) or index prescription date (for the treated), and the follow-up BMI was defined as the values that were reported during the 12-month period after the index diagnosis (for the untreated) or index prescription (for the treated) date.
Study design
This study used a retrospective cohort design in which patients were followed for 3, 6, 9, and 12 months from the index diagnosis (for the untreated) or prescription (for the treated) date, to compare the impact of different medication regimens and the length of drug exposure on BMI.
Exposure
The monthly psychotropic medication exposure of each patient during the follow-up period was ascertained by the prescription orders, the number of refills, and the documented discontinuation date. In the absence of documented discontinuation date, the last prescription record in the database was considered the last prescription before discontinuation. The medication regimens that patients received include AT monotherapy, MS monotherapy, AD monotherapy, AT+MS polytherapy, AT+AD polytherapy, and MS+AD polytherapy. Although AD monotherapy has been associated with manic switch, we observed that some patients in our cohort received the regimen briefly. The exposure to treatment regimens was coded as time varying, which could change from month to month.
Outcome
The outcome of interest was “monthly change in BMI,” which was calculated as the difference between the measures taken each month during follow-up and at the baseline. To do the calculation, all available BMI measures during the follow-up were identified, and months without a BMI measure were coded as missing. For months with multiple BMI measures available, the average of all BMI measures in the month was used.
Statistical analysis
Figure 1 shows a schematic of patients' BMI measures and treatment regimens as recorded over the follow-up period. Among the treated cases, BMI measures for each month were attributed to the treatment regimen prescribed to the patient for that particular month.
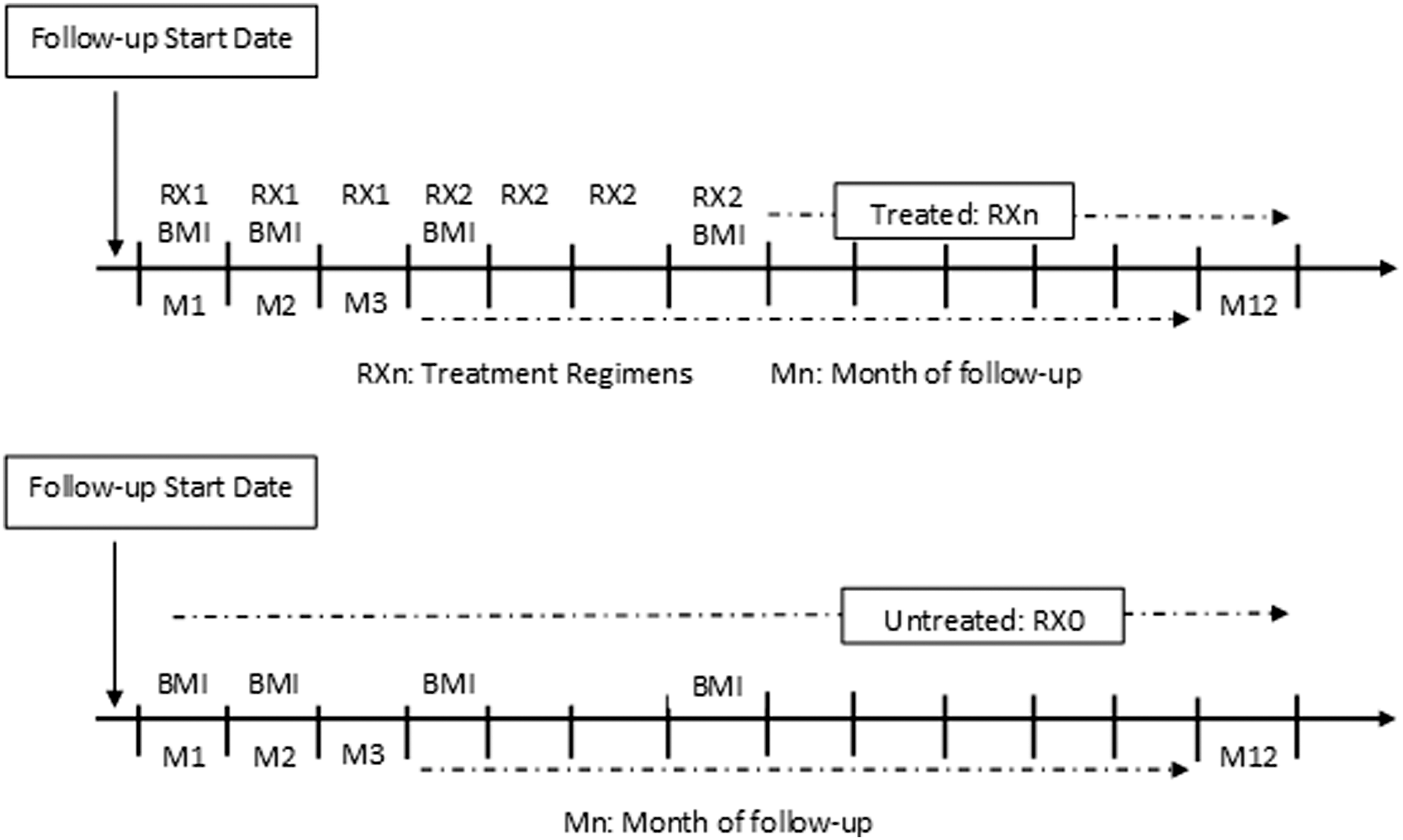
Schematic of a patient's BMI and treatment measure. BMI, body mass index.
A repeated-measures mixed model was applied to compare the risk of increase in BMI across treatment regimens, including the option of no treatment, during various follow-up periods. Mixed model is a flexible approach that is used to account for the presence of auto-correlation among repeated (monthly) exposure and outcome measures within each individual. The dependent variable of the model was monthly change in BMI from baseline to 3, 6, 9, and 12 months after the treatment initiation. The primary independent variable was the type of treatment regimen that patients received in each month. To determine the nature of autocorrelation among the observations nested under each patient, the Akaike Information Criterion value of the models assuming different covariance matrices was compared, and autoregressive heterogeneous variance-covariance structure was found to be the best fit.
Covariates controlled in this study were patient demographics, including age, gender, race, insurance type, and region; and clinical characteristics, including baseline and concurrent psychosocial and behavioral intervention, baseline BMI, and psychiatric comorbidities (anxiety disorder, attention-deficit hyperactivity disorder, depression, learning disability, oppositional/conduct disorder, and substance use disorder).
To further explore whether patients with certain characteristics and the utilization of medication concurrent with psychosocial or behavioral interventions could attenuate the adverse effect of psychotropic medications, a logistic regression analysis was conducted to explore the differences in demographic, baseline BMI, and psychiatric comorbidities between children and adolescents whose BMI had increased during the treatment versus those whose BMI stayed stable.
All analyses were carried out by using Statistical Analysis Software 9.3 (SAS, Cary, NC). This study was approved by the Institutional Review Board at the University of Houston.
Results
Cohort characteristics
As presented in Figure 2, a total of 17,779 children and adolescents with a diagnosis of bipolar disorder were identified. Of these identified bipolar cases, 7360 (41.4%) were ever treated and 10,419 (58.60%) were untreated. After excluding those treated cases who were not prescribed any guideline-recommended first-line treatment for bipolar disorder (AT or MS) (N = 897); those without a 180-day treatment-free period before the index diagnosis (N = 2371); and those without a minimum of one BMI measure at baseline and one during the follow-up (N = 1793), the treated group consisted of 2299 children and adolescents with a new treatment episode for bipolar disorder. For the untreated group, after excluding those individuals who did not have a documented activity after the bipolar diagnosis (N = 3538), and those without baseline and follow-up BMI measures (N = 2337), the final untreated group consisted of 4544 children and adolescents.
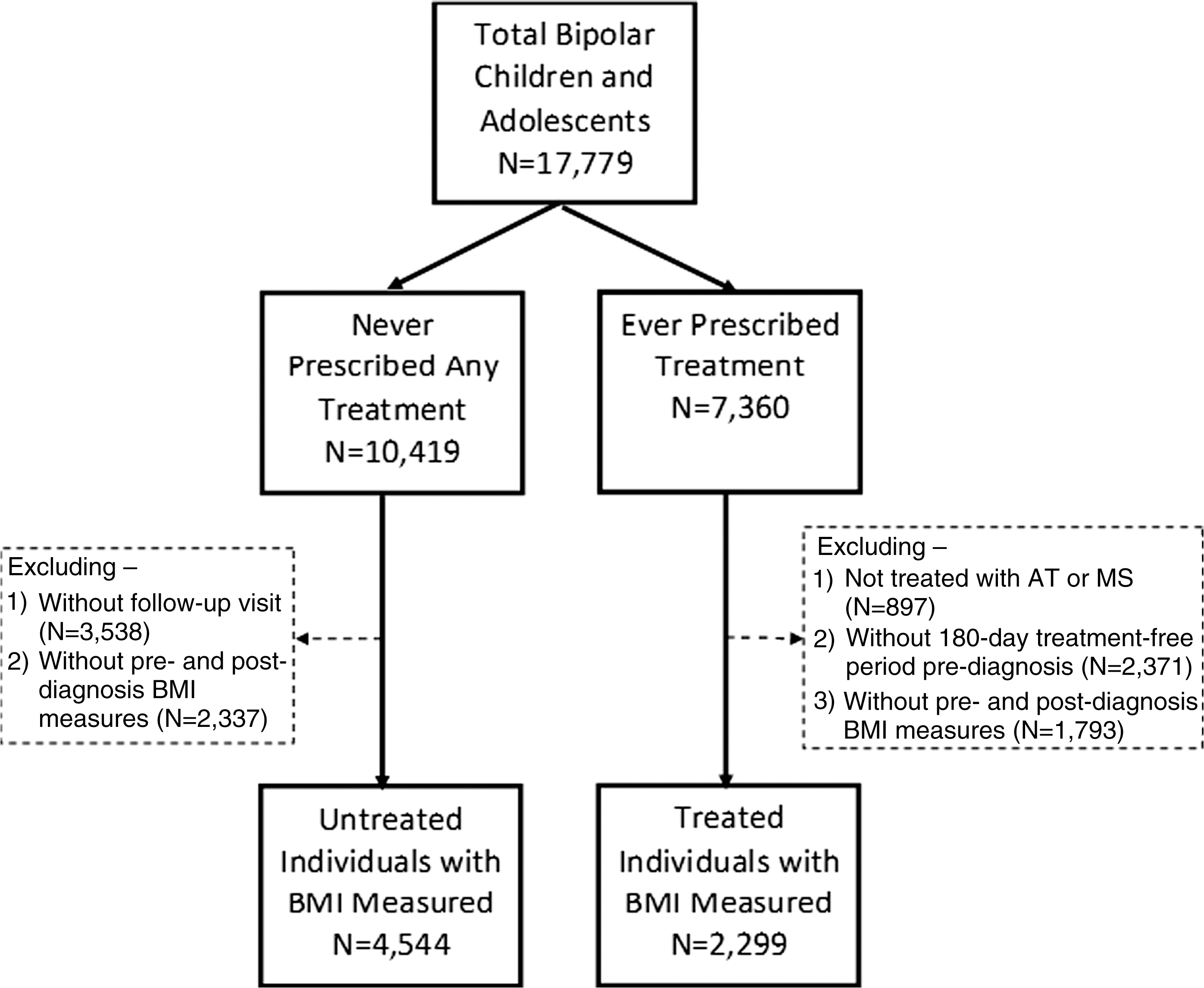
Schematic representation of cohort selection.
As presented in Table 1, the plurality of both the treated and untreated groups were white [treated: N = 1067 (46.41%); untreated: N = 1883 (41.44%)] and had commercial insurance [treated: N = 806 (35.06%); untreated: N = 1432 (31.51%)]. Both groups had comparable mean ages (treated: 13.51 ± 3.87; untreated: 13.77 ± 3.80), comprising roughly equal proportions of males (treated vs. untreated: 48.42% vs. 47.63%) and females (treated vs. untreated: 51.28% vs. 52.37%).
AD, antidepressants; ADHD, attention deficit/hyperactive disorder; AT, atypical antipsychotics; MS, mood stabilizers; ODCD, oppositional/conduct disorder.
Treatment utilization patterns
About 77% (N = 1766) of treated individuals were initiated treatment with monotherapy, and 23.19% (N = 533) were initiated treatment with polytherapy. The most commonly prescribed psychotropic monotherapy was AT monotherapy (N = 846), followed by MS monotherapy (N = 715) and AD monotherapy (N = 205). Of the 1766 patients who were initially prescribed monotherapy, 966 (54.70%) had treatment augmentation during the 1-year follow-up period, and of the 533 patients who were initiated treatment on polytherapy, 293 (55%) were switched to monotherapy. In total, 54.76% (N = 1259) of all individuals in the cohort were ever prescribed polytherapy. The commonly prescribed combination regimens were AT and MS (ATMS) (N = 444), AT and AD (ATAD) (N = 440), and MS and AD (MSAD) (N = 375).
Absolute change in BMI associated with the initial psychotropic regimens
Figure 3 presents the mean BMI of all patients at the baseline and the mean BMI of those individuals with BMI measures available at the last quarter of the 12-month follow-up period. The average BMIs of these individuals are presented by treatment regimens that they received at the time when the BMIs were measured. It was found that the highest increase in mean BMI among those treated was seen in those on AT monotherapy (1.20 ± 2.26 kg/m2), followed by those on ATMS combination (1.04 ± 2.71 kg/m2), ATAD combination (1.01 ± 3.24 kg/m2), AD monotherapy (0.72 ± 2.18 kg/m2), MS monotherapy (0.62 ± 2.37 kg/m2), and MSAD combination (0.61 ± 3.01 kg/m2). In the untreated individuals, the increase in mean BMI during the 12-month study period was 0.69 ± 2.64 kg/m2.
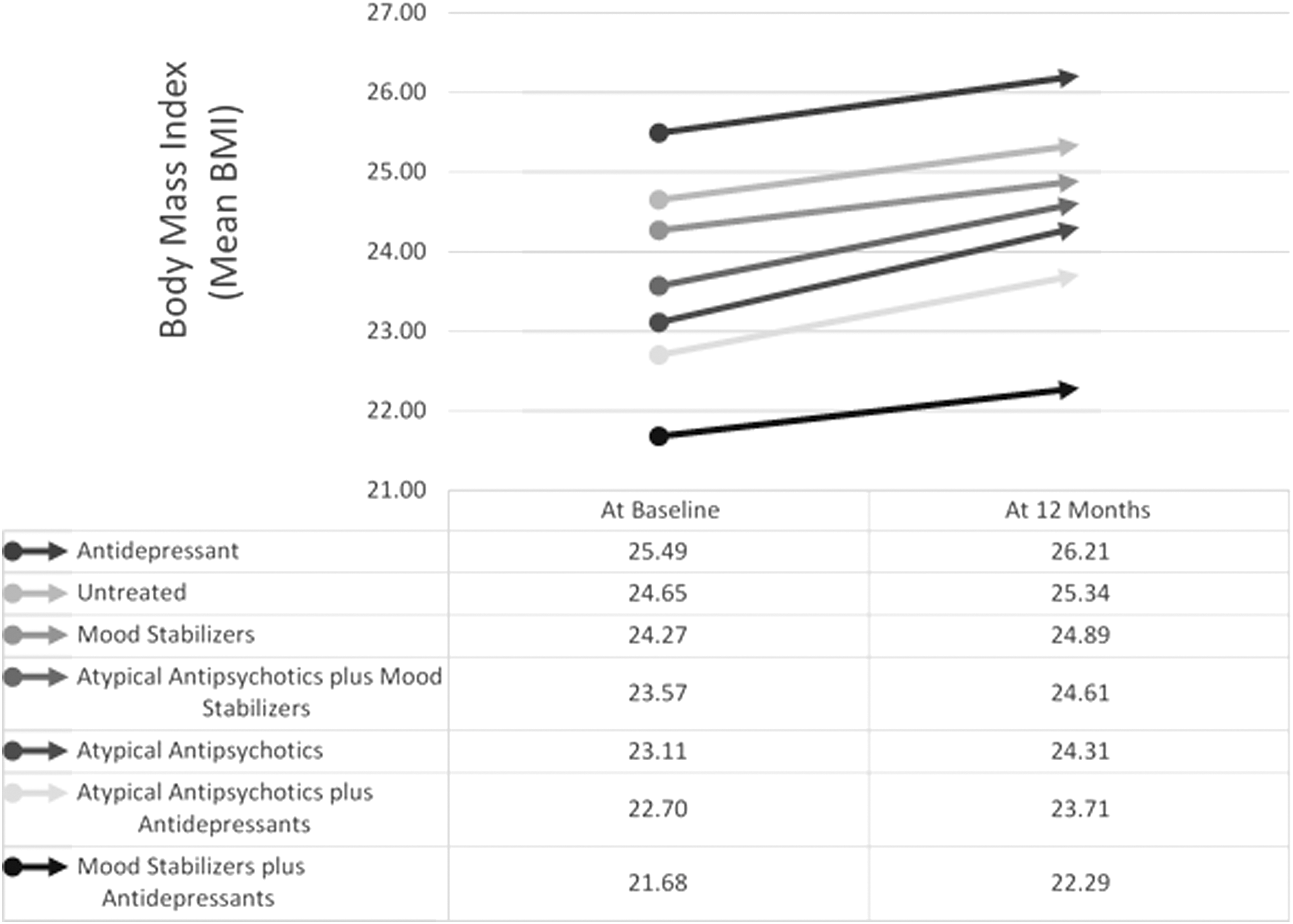
Treatment regimen effect on body mass index. BMI, body mass index.
Multivariate analysis on the association between treatment regimens and the corresponding change in BMI
Table 2 presents the estimated change in BMI associated with each treatment regimen during the 3-, 6-, 9-, and 12-month follow-up periods by using the repeated-measures mixed model. In all comparisons, AT monotherapy was used as the reference group and the effect of the treatments, time, and the interaction effect between the two were assessed.
AT, atypical antipsychotics; AD, antidepressants; BMI, body mass index; MS, mood stabilizers.
Treatment and time effect
The time effect estimated in the model indicated that the longer the use of AT (the reference group), the larger the cumulative increase in BMI. Each additional month of exposure to AT was associated with a 0.36 kg/m2 increase in BMI during the 3-month follow-up (p < 0.0001), 0.20 kg/m2 increase for the 6-month follow-up (p < 0.0001), 0.17 kg/m2 for the 9-month follow-up (p < 0.0001), and 0.16 kg/m2 for the 12-month follow-up cohort (p < 0.0001). The magnitude of the estimates suggested that the increase in BMI associated with AT monotherapy diminished over time and became stabilized after 6 months of the treatment.
As compared with AT monotherapy, the magnitude of change in BMI observed among untreated bipolar cases and in those treated with MS or AD monotherapy was significantly less at all time points, indicating less steep slopes of increase in BMI over time due to natural growth and development and the exposure to other psychotropic monotherapy regimens. The effect estimate for those untreated was similar to that for those treated with MS or AD monotherapy. For instance, the increase in BMI associated with these regimens was 0.16 kg/m2 (untreated), 0.24 kg/m2 (MS monotherapy), and 0.30 kg/m2 (AD monotherapy) less than AT monotherapy during the first 3 months of the follow-up period. The differences were reduced to 0.04 kg/m2 (untreated), 0.06 kg/m2 (MS monotherapy), and 0.07 kg/m2 (AD monotherapy) less than AT monotherapy when reaching the end of the 12-month follow-up period.
Among those who received the combination of ATMS, or ATAD, the changes in BMI relative to the AT monotherapy recipients were still negative; however, the majority of these differences were minor (−0.02 to −0.04 kg/m2), and none were statistically significant.
Baseline BMI
Children and adolescents who were overweight or obese at baseline were less likely to have increased BMI during the psychotropic treatment. Every 1 U higher BMI at baseline led to 0.04 kg/m2 (p < 0.0001), 0.04 kg/m2 (p < 0.0001), 0.03 kg/m2 (p < 0.0001), and 0.03 kg/m2 (p < 0.0001) less increase in BMI at 3, 6, 9, and 12 months of follow-up, respectively.
Age
Older children and adolescents had a greater increase in BMI. Every 1 year of additional age led to 0.04 kg/m2 (p < 0.0001), 0.04 kg/m2 (p < 0.0001), 0.03 kg/m2 (p < 0.0001), and 0.03 kg/m2 (p < 0.0001) increase in BMI at 3, 6, 9, and 12 months of follow-up, respectively.
Other covariates
Gender, race, geographical region, type of insurance, and comorbid conditions were not associated with change in BMI during follow-up.
Predictors of “increase in BMI” among atypical antipsychotic users
Given that the AT regimen was found to be associated with the most BMI gain and these drugs were also the most commonly used therapeutic category in patients with bipolar disorder (N = 1385, 60%), an ad hoc analysis was conducted to explore, within the atypical antipsychotic users, the factors that protected patients from excessive BMI gain. Of the 1385 atypical antipsychotic users, 65% (N = 896) showed an “increase in BMI” at the end of follow-up. As presented in Table 3, the logistic regression analysis identified baseline BMI, number of months on AT, and region as the significant predictors of increase in BMI. With each 1 kg/m2 increase in baseline BMI, it was 4% less likely that the subject would experience an increase in BMI at the end of follow-up (OR 0.96; CI 0.95–0.98), whereas with each additional month of exposure to AT, a patient was 1.1 (OR 1.10; CI 1.06–1.14) times more likely to experience increased BMI. Those residing in the South region were 1.32 (OR 1.32; CI 1.20–1.40) times more likely to have an increase in BMI compared with those who resided in the Midwest region.
AT, atypical antipsychotics; ADHD, attention deficit/hyperactive disorder; BMI, body mass index; CL, confidence interval.
Discussion
The findings of our analysis not only confirm the risks of weight gain associated with antipsychotic regimens as reported by previous short-term pediatric studies (Martin et al. 2000; Correll 2007; Fleischhaker et al. 2007; Correll et al. 2010; Maayan et al. 2011; Fiedorowicz et al. 2012; Almandil et al. 2013) but also provide evidence to support that prolonged exposure to antipsychotic medications in children and adolescents is associated with a continuous increase in BMI.
The majority of the weight gain associated with antipsychotics exposure in children occurred during the acute treatment phase rather than the maintenance. Such a plateau effect has been reported in previous long-term antipsychotic studies using adult samples (Kinon et al. 2001). The magnitude of change in BMI associated with antipsychotic medications during the first quarter of the treatment (0.36 kg/m2) was ∼1.5 times more than the increase in the second quarter (0.20 kg/m2), and more than twofold the change during the third and fourth quarters (0.16 kg/m2).
The increase in BMI associated with psychotropic regimens should be interpreted within the context of growth and development, as children and adolescents experience continuous and steady increases in BMI between ages 10 and 20. Our analysis on untreated individuals with bipolar diagnosis found that the average annual increase in BMI was 0.69 kg/m2 in this group. The magnitude is concordant with the annual BMI increase due to normal growth and development (0.5–0.6 kg/m2) estimated based on the growth curve (Kuczmarski et al. 2002). As compared with untreated cases, children and adolescents who initiated their treatment on AT monotherapy had a much higher annual cumulative increase in BMI (1.20 kg/m2). The multivariate mixed model showed that the difference in BMI change between AT monotherapy recipients and untreated cases was the greatest (0.16 kg/m2) during the first quarter of the treatment, and it then diminished to 0.05 kg/m2 in the second quarter and 0.04 kg/m2 in the third and fourth quarter. By the end of the 1 year follow-up, though the difference was minor, it still remained statistically significant. The comparison indicates that there is an additional BMI increase in children and adolescents using antipsychotic medications beyond the normal BMI change due to growth and development.
For those who received combination regimens, both the absolute and relative changes of BMI were driven by AT. The cumulative annual increase in BMI was around 1 kg/m2 among those initiated on ATMS and ATAD, which was similar to that observed in those initiated on AT monotherpy. However, for those who were initiated on MSAD combination, the absolute change in BMI (0.61 ± 3.01 kg/m2) was comparable to the change observed in MS and AD monotherapy groups, but significantly lower than the BMI increase associated with AT monotherapy.
One interesting finding of our study is that the average baseline BMI of AT regimen (AT monotherapy, ATMS and ATAD combinations) recipients were lower than that in those who received AD or MS monotherapy. Among the recipients of AT regimens, those who received the combinations as the initial treatment had relative lower baseline BMI than the AT monotherapy recipients. The utilization pattern probably reflects that providers were fully aware of the risk of weight gain associated with AT and psychotropic combinations, and have purposefully avoided to use these regimens in overweight and obese children and adolescents.
More interestingly, in all models, children and adolescents with higher baseline BMI experienced a less absolute increase in BMI during the follow-up. The exact mechanism of psychotropic medication-associated weight gain is still undetermined, but evidence points to their affinities for histamine H1, serotonin 5-HT2, and dopamine D2 receptors (Wetterling et al. 2001). These receptor activities, coupled with their influence on hypothalamic peptides and hormones, may affect energy homeostasis, causing an increase in appetite and reducing satiety (Correll and Malhotra 2004). In addition, an increase in the level of ghrelin, a peptide hormone also known as the “hunger hormone,” was observed in patients receiving long-term AT (Jin et al. 2008). The theory could explain why the lifestyle-modification effect of psychotropic medication was relatively minor among children with high baseline BMI, given that children who were overweight or obese before the treatment probably had already had a sedentary lifestyle and high carbohydrate intake.
The primary strength of our study is that the trajectory of change in BMI for different treatment regimens was observed during different follow-up periods, making the results more intuitive. Also, instead of censoring patients when there was treatment switching or augmentation, we accounted for the issue by defining treatment as a time-varying exposure. Our findings suggest that extended exposure to antipsychotic medications is associated with a chronic, continuous increase in BMI beyond the range of BMI variation due to growth and development. Given that bipolar disorder is a disease that requires long-term management using psychotropic medications and nearly 60% of pediatric cases received regimens including AT, the continuous increase in BMI associated with these medications could affect children's and adolescents' health in adulthood. Children and adolescents who are obese and overweight have a high likelihood of being obese in their adulthood. A study by Whitaker et al. (1997) found that ∼80% of children who were overweight at age 10–15 years were obese adults at age 25. Childhood obesity is associated with adult cardiovascular adverse outcomes and impaired glucose tolerance (Sinaiko et al. 1999; Srinivasan et al. 2002; Bhargava et al. 2004; Baker et al. 2007). It is also associated with long-term health risks such as type 2 diabetes, hyperlipidemia, and hypertension (Stigler et al. 2004). Further study is needed to develop specific weight management strategies for this high-risk population.
Despite the strengths, the study has some limitations. The EMR database used in the study contains only information regarding prescription orders rather than the actual utilization of medication. To ascertain the dates of medication exposure, we developed an algorithm that combines information, including the date of prescription orders, number of refills, and the discontinuation date documented in the database. Even with the application of this algorithm, a misclassification of drug exposure was still possible if a patient did not take the medication as prescribed. Moreover, the database does not contain complete information on socioeconomic status, diet, physical activity, and health status of patients' parents. Although controlling for baseline BMI partially accounted for these unmeasured confounding, it limits our ability to further explore potential solutions for psychotropic medication-related BMI increase.
Conclusion
The long-term use of AT, both as monotherapy or in combination with other psychotropic medications in children and adolescents with bipolar disorder, was associated with a steady and cumulative increase in BMI.
Clinical Significance
The findings support the current guideline that recommends intensive weight/BMI monitoring during the first 12 weeks of antipsychotic treatment, and continuous monitoring every 6 months during the rest of the treatment course. Given the significant long term health consequences of childhood overweight and obesity, it is important to conduct future studies to understand the BMI trajectory after the discontinuation of antipsychotic treatment.
Footnotes
Disclosures
No competing financial interests exist.